Servicios personalizados
Servicios personalizados Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
The annual number of interprovincial travelers has steadily increased over the last decade all around the north coast and the northeast and the acquisition of travel-associated infectious diseases is one of the major problems in public health.1 In the last two years, malaria cases have been reported in jungle regions such as Loreto, Amazonas, and San Martín; in the last two, there are cities such as Bagua and Tarapoto that, although they have reported very little incidence of the disease, the risk remains latent since, in the cities that are around them, there is an increase in cases. It should be noted that the cities of Tarapoto and Bagua are commonly visited by people who travel for multiple reasons.2 To travel to tropical and sub-tropical geographic areas cause an increased probability of exposure to endemic infectious diseases like malaria.3 Transport networks continue expanding year by year, land transportation is faster and more comfortable than in past years, the volume of passengers can now move further, than ever before, these actions increase the spread of infectious diseases.4)
It is well known that the spread of travel-related infectious diseases in travelers is increased by visiting rural and remote areas more frequently, activities during travel like tours, a greater consumption of high-risk food and drink in the local market, and a lower likelihood of seeking medical consultation before their journey as a recommendation or follow recommended vaccinations before the trip.5,6,7,8 For these reasons travelers on interprovincial trips must know the impact of infectious diseases in endemic regions and have a real awareness of the risk of acquiring a travel-related affliction, these diseases can be prevented through vaccinations, antimalarial drugs, and advice from healthcare professionals. The travel agencies and the government of Peru did not provide enough and accurate information about the risk and prevention of malaria to travelers who travel to the Amazon of Peru.9 In cross-sectional surveys of travelers who visit malaria-risk areas, it has been shown that some of them comply with preventive measures for this disease.10
In this context, we want to understand the travelers' knowledge, and practices, this could provide interesting information to make health policy to plan educational interventions on this population to prevent effectively travel-related diseases. The objective of this research is to examine the traveler's knowledge, attitudes, and practices of travel-related malaria.
Methods
Study setting and sample
This cross-sectional study was performed between January and May in 2019, in two bus stations in the area of Chiclayo. The sampling method was performed by a researcher who applied anonymous questionnaires at the arrival entrance at the bus station until the passenger waits to arrive at the bus. We select the bus station which travels to the north oriental area of Peru. The passenger participated voluntarily; we do not promote any incentive; the questionnaire was not piloted and was designed based on the experience of infectologists and epidemiologists who work at a Hospital, Peru, who are experts in vector-borne diseases. We include the passengers who have 18 years or more, trips to destinations with an intermediate or high risk of malaria were selected (Amazonas, San Martin, Cajamarca, Loreto). We exclude incomplete and incorrect questionnaires. The Ethical Committee of the Universidad Nacional Pedro Ruiz Gallo approved the study with resolution 023-19. Also, permission was requested from the authorized persons of each bus station. Informed consent was obtained from participants before the survey when it was clarified that participation was voluntary. Anonymity and confidentiality of data were ensured.
Questionnaire
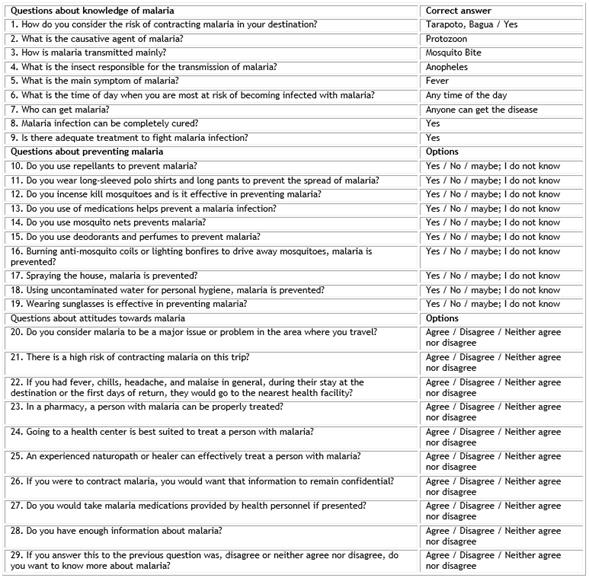
The survey consists of 29 questions, 9 knowledge questions, 9 preventing questions, 11 attitude questions. Our instrument was previously it was approved by an expert in the area of epidemiology and an expert in the area of infectious diseases in the region.
The survey questions were selected taking as a reference other similar studies concerning knowledge, attitudes, and practices about malaria in travelers.
The answers to the questions were graded as correct or incorrect, assigning a determined score and a final grade, which was as follows:
Knowledge level: It was graded through a vigesimal scale. Dividing the final marks according to the following table Poor <equal 10 (less than the 50th percentile), regular 11 to 13 (between the 50th and 70th percentile), good from 14 to 17 (greater than the 70th and lower 90th percentile), very good 18 to 20 (greater than the 90th percentile).
Attitude level: It was rated through a vigesimal scale. The final grades are divided according to the following table: inadequate from 0 to 11 (lower percentile equal to 55), and adequate from 12 to 20 (higher percentile of 55). The questions were grouped as follows:
General characteristics: Age, sex, educational level, city to which you travel, have you previously suffered from any of the following diseases (Malaria, Dengue, Bartonellosis, Leishmaniasis, or Trypanosomiasis), do you have any current physical condition?
The characteristics associated with the trip: Purpose of the trip, length of stay at the destination. You can see the questionnaire in the annex.
Statistics
The collected data were entered into Microsoft Excel using a double data entry method and then reviewed for quality control. Variables were described using absolute and relative frequencies. Global frequencies and percentages were used to present general aspects, knowledge, and practices. All analyzes were performed using STATA 12.
Results
We record data of 250 participants. The average age was 36.8 years (SD: 13.14 years), with a similar proportion between men and women. The vast majority traveled for tourism (45.2%) or personal reasons (44.8%). It was observed that the knowledge of the patients was good at 29.13%, practices were 14.74%, and attitudes 18.33% (Table 1).
Table 1 Characteristics of travelers surveyed in bus station traveling to areas of northeastern Peru
About the level of knowledge, it was found that there were no differences between sex or age; but those with a higher education degree had a better level of knowledge compared to those in secondary school (Table 2).
Table 2 Knowledge level of travelers surveyed in bus stations traveling to areas of northeastern Peru

*t-Student.
About the level of practices, it was found that there were no differences between sex or age, nor at the educational level, but it was slightly higher in those of higher grade (Table 3).
Table 3 Practices of malaria in travelers surveyed in bus station traveling to areas of northeastern Peru
*Chi-square.
Regarding attitudes, it was found that there were no differences between sex or age; but those with a higher education degree had a better attitude about malaria compared to those in secondary school (Table 4).
Table 4 Attitudes about malaria in travelers surveyed in bus station traveling to areas of northeastern Peru
*Chi-square.
Also, 60 people (24%) were asked about their self-perception of knowledge about malaria and stated they had an adequate level of self-perceived malaria knowledge. Of the 190 who reported not having enough knowledge about malaria, 49.47% were interested in learning about malaria practices, followed by 25.26% who were interested in knowing about treatment. Age in tables refers to the mean age and the units are years.
Discussion
Malaria has had a greater impact than any other infectious disease in world history. More than 300 to 500 million people worldwide are infected with Plasmodium spp., and 1.5 to 2.7 million people a year, most of whom are children, die from the infection.11 According to the WHO, malaria persists as an important cause of morbidity and mortality in risk regions; There are very few studies carried out on travelers from South America that allow us to measure how much people know about this disease and what level of attitudes they have. In Peru, malaria continues to be a public health problem, mainly in jungle regions. where there is the highest prevalence.12 The knowledge, attitudes, and practices (KAP) study carried out on the population of travelers to these regions was carried out as a strategy to gain an in-depth understanding of this problem and subsequently allow correct decision-making regarding the prevention of this disease.13
Our investigation is one of the first studies on this topic describing the knowledge, attitudes, and prevention of malaria in travelers in Peru. The potential role of this research could be used in developing strategies for this health issue. Peru is highly affected by malaria since its geography and rainy areas make this public health problem prevalent.14 Amazon regions are considered endemic for malaria.15 This is due to the humid areas presented by high rainfall.16 One of the problems associated with malaria in Peru is the treatment time that lasts up to three days in the Peruvian Amazon.17 It has been seen that in Peru the knowledge and techniques could reduce malaria in the Peruvian territory.18
The travelers need to improve their knowledge because of the participants surveyed only 29.13% had a good level of knowledge. This result is unsatisfactory compared with other surveys published from other countries with a high level of knowledge.19) We found studies with similar results. These differences may be attributed to the different populations who do not have similar characteristics, methods of collecting the data, and instruments used. The travelers did not receive any information or recommendation about the risk of malaria in the areas that travel. We think our results reflect the vast reality of the travelers because they do not investigate the risk of infectious diseases and the high frequency of the trips normalizes this.
It is important to know the travelers showed little concern about the risk of getting malaria during their travel. This result is in the line with other studies conducted in other countries with different populations where travelers have a low perception of the malaria risk. Results from this study show travelers did not receive information about the endemic areas to those who traveled, regarding measures for preventing the risk of getting malaria in the destination.5,20 The level of knowledge of prevention was low at 14.74%, the majority did not show actions to prevent the infection with malaria, in other studies we found similar results that people did not foresee the risk of malaria.21,22 In general, this behavior of travelers can be explained by the fact that they do not usually undergo health checkups until they show some symptoms.
In this study, traveler attitudes about malaria were low. This is not related to an investigation where immigrant travelers in the United States traveling to sub-Saharan, Africa, of which approximately 60% of the total of respondents affirmed to have taken an antimalarial in their last trip.23 In the same way, they also affirmed the use of repellent against mosquitoes. This shows that these people show greater concern when they travel to places at risk of malaria due to the preventive behavior of these travelers.23 Likewise, Dutch travelers who went to areas at risk of malaria showed preventive attitudes that were improving over time,24 and also in Egyptian travelers where they showed a good attitude towards vaccination and think that it is necessary before a trip.25 This demonstrates that in our country there is still ignorance and lack of concern about infectious vector-borne diseases, especially when making a trip to a place of risk, a situation that in other countries does not occur and that thanks to the same population become aware of these diseases, can promote the advancement of prevention measures in airports.
Regarding attitudes, it was found that there were no differences between sex or age; but those with a higher education degree had a better attitude about malaria compared to those in secondary school. However, in a study of Egyptian travelers, the overall attitude towards vaccination and the perceived benefits of malaria prophylaxis were significantly correlated with advancing age, but coincide in terms of correlation with the higher educational level of malaria knowledge25 and also in a reliable survey in Yaoundé, where the attitude analysis revealed that people with a university or secondary education have a better knowledge of prevention measures and treatment measures for malaria compared to those at the primary level, where gender did not have significant significance.26 We can say then that people with a higher educational level have a better attitude towards infectious diseases due to the same education and closer relationships with health professionals, regardless of gender or age.
Besides, 60 people (24%) were asked about their self-perception of knowledge about malaria and stated they had an adequate level of malaria knowledge. Of the 190 who reported not having enough knowledge about malaria, 49.47% were interested in learning about malaria prevention, followed by 25.26% who were interested in knowing about treatment. This is valuable information to generate more knowledge and propose prevention and treatment measures to travelers who go to areas at risk of any infectious disease, including malaria, either before the trip, during their stay on-site and after the trip, to ensure maximum follow-up and to avoid new outbreaks of infections.
It is important to understand how people recognize risks and communications about the risk of becoming infected with malaria.27 There are differences between people who travel through tourist agencies and those who travel for personal reasons,28 In our study, people who traveled for personal reasons had worse knowledge than those who did not. The more experienced tourists take antimalarial drugs as part of the recommendations followed to travel to malaria-endemic areas.29 Precautionary measures for young long-stay travelers and people visiting primarily for business purposes should be strengthened.27
Data were collected on travelers departing from a city on the north coast of Peru. Most of the data came from a small population and only two large bus stations, with more than five small and medium-sized terminals in the city of Chiclayo. One of the limitations regarding the sample is that people who voluntarily accessed the study were surveyed, leaving out many people. Volunteer bias and the survey has not been psychometrically validated. There is no mention of emergency self-treatment of malaria in this study, there must be a part of emergency treatment for travel to low-risk malaria areas.30 Furthermore, these surveys were conducted over a short period of months, and therefore, epidemiological trends cannot be deduced from this point prevalence studies. Since then no follow-up evaluations have been conducted and therefore current population estimates should be based on current data. Finally, the characterization of malaria in the sentinel population of travelers provides an overview of the scale of infection transmission but is not entirely representative of the general population.
The first recommendation to give is proper instruction and training, including the successful performance of the testing procedure. Some cities already apply such measures in airports, such as the city of Boston, in the United States, where most people took chemoprophylaxis before traveling, used mosquito repellent, and slept with a net in their bed.10 The population plays an important role in creating health strategies, that is why this type of study is carried out to improve the quality of prevention and interest in learning more about the diseases that can occur when traveling. The results of this study showed that travelers had low knowledge of malaria infection and do not often practice preventive measures when they travel to endemic areas. These findings show the importance of implementing better modes to communicate and educate travelers about the problem of malaria causes.