










 Servicios personalizados
Servicios personalizados Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkINTRODUCTION
Fat excess in the body can be harmful in the population’s health, which behaves as a multifactorial problem and predisposes to the presence of non-transmissible chronic diseases.1
Among non-transmissible chronic diseases, it can be mention cardiovascular diseases (cardiomyopathy and cerebrovascular accident), metabolic diseases (type 2 diabetes mellitus, dyslipidemia, hyperuricemia and metabolic syndrome), musculoskeletal, digestive and neoplastic diseases, which represent a high morbidity and mortality prevalence in the general population.2
The study of fat excess in the population is possible using a fast, easy and inexpensive method by quantifying anthropometric indices, of great importance in primary care due to the possibility of screening cardiovascular and metabolic diseases.3
Differences in fat excess depend on non-modifiable factors such as age, sex, race and genetics, which implies an important value in clinical practice, as it is pathophysiologically implicated in resistance to insulin action mediated by b-cell lipotoxicity, pancreatic diseases, as well as promoting a chronic inflammatory state mediated by adipokines and other substances such as leptin, resistin, angiotensinogen, pro-inflammatory cytokines and chemokines.4
The assessment of anthropometric indices is very useful in primary care and epidemiological research, it helps to predict a number of cardiometabolic diseases and allow the construction of prevention interventions.5
Body mass index is widely used among obesity indicators, and can vary according to the age, sex, and body biotype of certain individuals, so it is necessary to complement the analysis with the measurement of abdominal circumference, because it has less variation influence, however, for a better clinical evaluation, other indices such as waist-height index, waist-hip index, body fat percentage can be used.6
Cardiovascular diseases cause a considerable global mortality, with 31% of deaths due to this condition, and 71% of them occur in countries with low and middle income. Furthermore, 85% of all disabilities are caused or related to cardiovascular disease.7,8
Currently, it is known that the metabolic syndrome (MetSyn) is a condition characterized by the presence of cardiovascular and metabolic factors such as arterial hypertension, hypertriglyceridemia, hyperglycemia, abdominal obesity and high-density cholesterol. The metabolic syndrome presents a heterogeneous prevalence, thus according to the meta-analysis carried out by Hosein et al.10). in 2020, MetSyn was estimated at 8.3%, and according to Baygi et al.11 in the same year the global prevalence of MetSyn was 21%.9,10,11
In the Ecuadorian context, there is no consensus on the prevalence and optimal predictive anthropometric values of MetSyn in the general population; but the prevalence of dyslipidemia and MetSyn in military personnel is low compared to the general population.12,13,14
Therefore, this study determines to establish the optimal cutoff of anthropometric indices to predict Metabolic Syndrome in army instructors of Military Sciences career at the University of the Armed Forces in Ecuador.
METHODS
This is an analytical, non-experimental study. It was carried out in the instructors of Military Sciences career at the University of the Armed Forces, located in Ambato city - Ecuador, during the year 2020. The population of the study was 366 instructors, with a sample of 203 (95% confidence level and 5% margin of error).
The variables analyzed were:
Height and weight (measured without shoes and in underwear).
Hip circumference (HC), waist circumference (WC), measured with a non-elastic measuring tape at the level of the widest part of the buttocks and at the level of the iliac crests respectively, which is classified as: a) low (WC ≤ 93 in men and ≤ 79 in women), b) high (WC ≥ 0.94 in men and ≥ 0.80 in women).15
Body Mass Index (BMI) = weight (kg) / height2 (m), which was classified into 4 groups (underweight: ≤ 18.5, normal weight: 18.5-24, overweight: 24-30 and, obesity: ≥ 30).2
Waist-hip ratio (WHR) = waist measurement (cm) / hip measurement (cm), which was classified into 2 groups (high: ≥ 0.95 in men and ≥ 0.90 in women, low: ≤ 0.95 in men and ≤ 0.90 in women).16
Waist index height (WHtR) = waist measurement (cm) / height (cm), which was classified into 3 groups (high: ≥ 0.52, low: ≤ 0.48, and normal: 0.48 - 0.52).17
Waist circumference weight index (WRWC) = weight (kg) / waist circumference measure (cm), which was classified into 4 groups (deficit: <0.44; normal: 0.44 - 0.80, overweight: 0.80 ≤ - <0.98, obesity: ≥ 0.98).18
Body fat percentage (BFP) = 1.51 x (BMI) -0.70 x (Age) - 3.6 x (1) +1.4 (Male) and BFP = 1.2 x (BMI) + 0.23 x (Age) - 10.8 x (sex) - 5.4 (Female), which was classified into 3 groups (normal: 12-20 in males and 24-30 in females, limit: 21-25 in males and 31-33 in females, and obesity: > 35 in males and > 33 in females).19
Laboratory tests: fasting glycemia, total cholesterol and triglycerides, urinalysis.
Blood pressure (measured with a digital cuff blood pressure monitor).
It is necessary to mention that the High-Density Cholesterol-C (HDL-C) test, as it is not considered a routine lipid test in the Institution, was not evaluated in this research study.
The variable metabolic syndrome (MetSyn) was analyzed according to the pre-established criteria of the World Health Organization - WHO (MetSyn OMS), ALAD (MetSyn ALAD), ATP III (MetSyn ATP III) and Harmonizing the metabolic syndrome (MetSyn HARM).20,21
The information collection instruments were annual medical record, carried out during the month of October 2020 (laboratory tests, and medicine, dental and mental check-up), and anthropometric record, carried out in November 2020, which analyzes the general nutritional status by evaluating folds (triceps, supra scapular, supra iliac, abdominal, thigh and leg), diameters (fist, elbow and knee), perimeters (thigh, arm and calf) as well as abdominal and hip circumferences.
The pre-established inclusion criterion is to be instructor of the Military Sciences career at the University of the Armed Forces. On the contrary, the instructors with incomplete annual medical records and incomplete anthropometric records were excluded.
The information was obtained with prior authorization from the director of the Institute and the Institute's ethics committee.
The statistical analysis was performed with the SPSS -version 22- and MedCalc programs, the variables are expressed as mean ± SD for continuous variables, which were compared by Student's t test. In addition, the analysis of the receiver operating characteristics (ROC) curve using the Youden index to determine the optimal cut-off point of the anthropometric indices in the diagnosis of metabolic syndrome were considered statistically significant (< 0.05).
RESULTS
According to the ALAD criteria 8 male instructors had MetSyn (%: 4.08, SD: 0.52), with a mean age of 41 years (SD: 4). According to the ATP III criteria 15 males presented MetSyn (%: 7.65, SD: 0.52), with a mean age of 41 years (SD: 4). According to HARM criteria there were 11 males with MetSyn (%: 5.4, SD: 0.52), with a mean age of 41 years (SD: 4). Finally, according to WHO criteria, there were 15 males (%: 7.65%, SD: 0.52), with a mean age of 40 years (SD: 5), however, no women presented diagnostic criteria, and they were excluded from the study because they represented a very small proportion within the sample (n: 7).
Likewise, the most prevalent criterion was triglycerides, according to MetSyn ALAD with 3.4% (n: 7, SD: 0.35), according to MetSyn ATP III with 6,9% (n: 14, SD: 0.26), according to MetSyn HARM with 4.9% (n: 10, SD: 0.30), and according to the MetSyn WHO with 7.4% (n: 15, SD: 0.00).
The more prevalent anthropometric indexes according to MetSyn ALAD are WC with 3.9% (n: 8, SD: 0.0) and WHtR with 3.9% (n: 8, SD: 0.0), according to MetSyn ATP III overweight with 6.4% (n: 13, SD: 0.35) and WHtR with 7.4% (n: 15, SD: 0.0), according to MetSyn HARM overweight with 4.5% (n: 9, SD: 0.40) and WHtR with 5.4% (n: 11, SD: 0.0), and according to the MetSyn WHO overweight with 6.4% (n: 13: 0.35) and WHtR with 6.4% (n: 13, SD: 0.35) (table 1).
Table 1 Characteristic of the study population and MetSyn
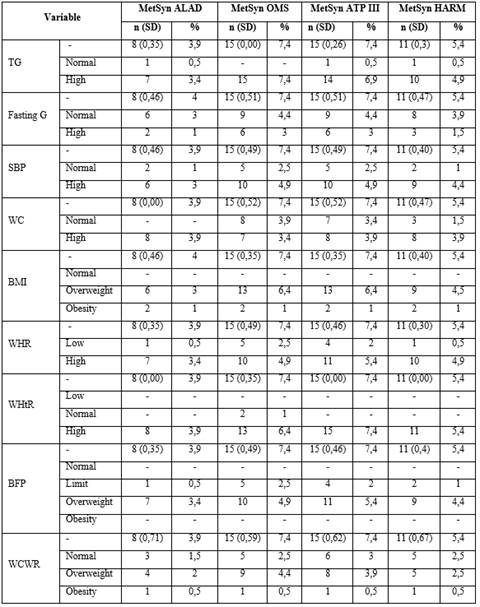
MetSyn: Metabolic syndrome, n: Number, %: Percentage, SD: Standar desviation, TC: Total cholesterol, TG: Trygliceride, Fasting G.: Fasting glucose, SBP: Systolic blood pressure, DBP: Diastolic blood pressure, WC: Waist circumference, BMI: Body mass index, WHR: Waist hip ratio, WHtR: Waist height ratio, BFP: Body fat percentage, WCWR: Waist circumference weight ratio.
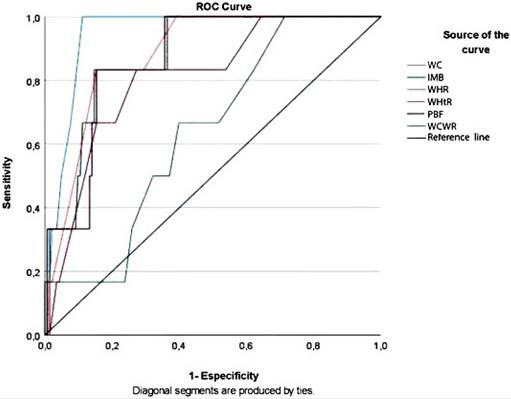
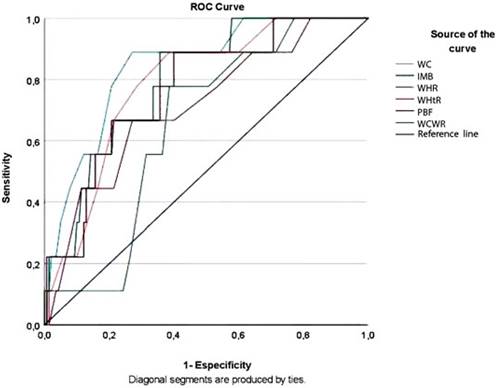
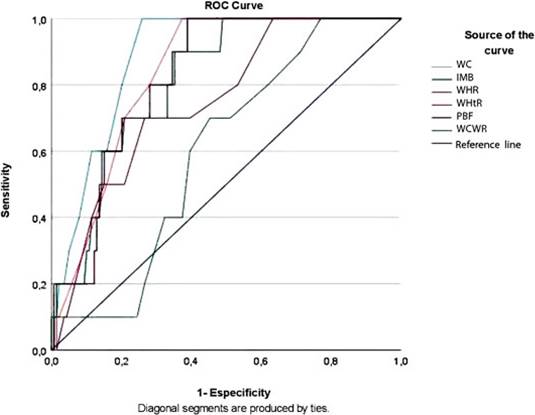
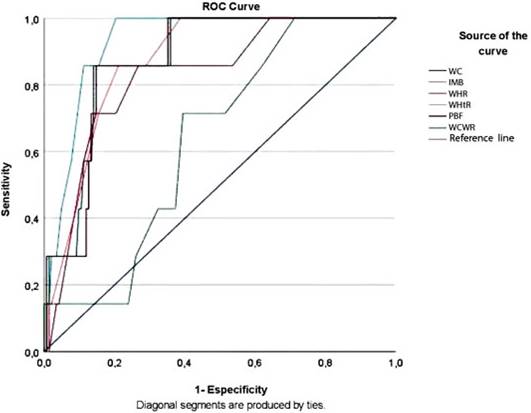
When analyzing the optimal cut-off value of anthropometric indices to present metabolic syndrome, according to MetSyn ALAD the highest AUC are WC (0.915, 95% CI 0.867-0.950) and WHtR (0.85, 95% CI 0,792 - 0,897) (with an optimal cut off of 95 cm for WC and 0.56 for WHtR). According to MetSyn ATP the highest AUC is WC (0.824, 95% CI 0,764 - 0,875) and WHtR (0.783, 95% CI 0,719 - 0,839). According to MetSyn HARM the highest AUC is WC (0.849, 95% CI 0,791 - 0,896) and WHtR (0.825, 95% CI 0,765 - 0,876). Finally, according MetSyn OMS the highest AUC is WC (0.777, 95% CI 0,712 - 0,833) and WHtR (0.721, 95% CI 0,653 - 0,783) (the optimal cut off in MetSyn ATP, HARM and OMS is 91 cm for WC and 0.53 for WHtR) (Fig. 1, Fig. 2, Fig. 3, and Fig. 4).
DISCUSSION
The prevalence of MetSyn according to the different criteria in this study, ALAD 8 male (%: 4.08, SD: 0.52), ATP III 15 male (%: 7.65, SD: 0.52), Harmonizing 11 male (%: 5.4, SD: 0.52) and finally, male WHO 15 (%: 7.65%, SD: 0.52), differ from what was observed in a meta-analysis of Mexico in non-military personnel, where the prevalence according to the IDF criteria is 54% (95% CI 0.44-0.63), ATP III 36% (95% CI 0.30 -0.42) and WHO 31% (95% CI: 0.04-0, 81),22 as well as what was observed by Herrera et al.23 in 2017, where MetSyn was presented in non-military personnel in 28.7% according to the ATPIII criteria and 37.9% according to the criteria IDF.
The prevalence of MetSyn ATP III was 7.65%, is lower than that observed in a study in Iranian military personnel, where the prevalence was 11.1% and in a study in Taiwanese military personnel (mean age: 35.9 years) where the prevalence was 15%. However, this difference is more accentuated when observing a study carried out in a population of military soldiers in Brazil (mean age: 45 years) where the prevalence was 38.54%.24,25,26
Likewise, the prevalence of MetSyn according to this study is lower than that observed in a meta-analysis in Latin American countries in non-military personnel, where it was presented in 24.9% of the population (age range: 18.8-43.3), and in a population of 10,318 non-military participants in Ecuador (age range 18-59 years) where 31.2% had MetSyn. However, it is very similar to a study in military personnel (mean age: 37 years), where 8% presented MetSyn in Ecuador.12,27,28
According to this study, the most prevalent diagnostic criterion for MetSyn is triglycerides (MetSyn ALAD: 3.9%, MetSyn ATP III: 6.9 , MetSyn Harm: 4.9%, and MetSyn WHO: 7.4%) as well as the most prevalent anthropometric indices were WC, WHtR and BMI (MetSyn ALAD: WC of 3.9%, and WHtR of 3.9%, MetSyn ATP III: overweight of 6.4% according to BMI and WHtR of 7.4% , MetSyn Harm: 4.5% overweight according to the BMI and WHtR of 5.4%, and MetSyn OMS: overweight with 6.4% according to the BMI and WHtR of 6.4%), which are similar to those observed in non-military personnel from a meta-analysis conducted by Baygi et al.,11 although in a remarkably high percentage, where triglycerides were present in 24%, overweight in 35%, obesity in 14%, abdominal obesity in 29% of the participants.11
The predictive anthropometric indices of MetSyn according to the highest AUC in this study are the WC and WHtR (MetSyn ALAD: WC: 0.915, WHtR: 0.85, MetSyn ATP III: WC: 0.824, WHtR: 0.783, MetSyn Harm: WC: 0.849, WHtR: 0.800, and MetSyn WHO: WC: 0.777, WHtR: 0.721), with optimal cuts according to MetSyn ATPIII very similar to those found in other studies (MetSyn ATP III: WC: 0.91, WHtR: 0.53). Observing that in Iran, WC and WHtR had an AUC of 0.65 and 0.64 respectively as predictors for MetSyn, with an optimal WC cut of 91 cm.27 Likewise, in another study, WC presented an AUC of 0.82 and WHtR with an AUC 0.79, in which WC presents an optimal cutoff of 89.3 cm to predict MetSyn.30
In Ecuador, in a study in children (mean age: 12 years) the optimal cut-off values to predict WC MetSyn was 92 cm and WHtR of 0.52 respectively, as well as, in older male adults (mean age 70.6 years), the optimal WC cutoff to predict MetSyn was 91.2 cm (sensitivity 73.2%, specificity 62.8%, and YI 0.36), finally, the values are similar to those observed in military personnel (mean age: 37 years), where the optimal cut was 92 cm for WC and 0.52 cm for WHtR respectively.12,31,32
Additionally, it is worth to mention that military instructors have a low prevalence of dyslipidemia, overweight, obesity and MetSyn, compared to the information observed in the general population and foreign military personnel, which could be due to intrinsic cardiovascular and metabolic protection of the physical activity they do by this population group as part of their professional duties.
This study presented limitations in its development, as it was not possible to consider HDL-C in the diagnosis of MetSyn, which is not part of the routine blood test in these personnel, for which it is recommended to carry out a study where this is included lipid profile criterion. Additionally, there is not information about the use of other existing criteria (ALAD, WHO, HARM) for the diagnosis of MetSyn in military personnel in the country.
According to this study, it is concluded that the best anthropometric indices for the diagnosis of MetSyn (represented by the higher AUC) are WC and WHtR, with an optimal cut off similar to the general population, both national and foreign, however these values are lower than the criteria established by the ALAD.

