










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Articulo
 texto en
texto en  Español (pdf)
Español (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkRevista de Ciencias Médicas de Pinar del Río
versión On-line ISSN 1561-3194
Rev Ciencias Médicas vol.27 no.3 Pinar del Río mayo.-jun. 2023 Epub 01-Mayo-2023
Articles
Metabolic syndrome in older adults of the nursing home ¨ Carlos Castellano Blanco¨
1University of Medical Sciences of Pinar del Río. Faculty of Medical Sciences "Dr. Ernesto Che Guevara de la Serna". Pinar del Río, Cuba.
ABSTRACT Introduction: non-communicable diseases impede social and economic development worldwide, with a tendency to increase in incidence and mortality, a context in which the Metabolic Syndrome is inserted. Objective: To determine the incidence of metabolic syndrome in older adults of the ¨Carlos Castellano Blanco¨ nursing home in Pinar Del Rio. Methods: a descriptive observational study was carried out in the Nursing Home already mentioned, in the period from January to September 2020. The universe consisted of 160 elderly adults, 54 of whom had a diagnosis of Metabolic Syndrome, leaving a sample of 40 elderly who met the inclusion criteria. The information was extracted from individual medical records, used to form a database in Microsoft Excel and processed by calculating absolute and relative frequencies and Chi-square test (X2) to establish the relationship between variables. Results: metabolic syndrome was diagnosed in 34 % of the older adults, predominantly in the male sex (60 %) and in the 60 to 69 years age group (62,5 %). Arterial hypertension, elevated triglycerides and type 2 diabetes mellitus were the most frequent components of the metabolic syndrome. Non-alcoholic fatty liver disease represented 52 % of the patients and microalbuminuria 20 % of the sample; older adults without alterations in glycemic control predominated. Conclusions: the degenerative changes in the elderly justify the high frequency, particularities of the Metabolic Syndrome and the high risk of complications and mortality.
Key words: METABOLIC SYNDROME; AGED; INSULIN RESISTANCE.
INTRODUCTION
The global burden and threat of non-communicable diseases impede social and economic development, a context in which the Metabolic Syndrome (MS) is inserted, as it is related to the diseases with the highest mortality and shows an increasing trend in its incidence.1 The scientific community relates MS to the pandemic of obesity, diabetes and recognizes that its prevalence increases with age,2
The pathogenesis of MS is complex, with insulin resistance and the association with diabetes, obesity, hypertension, steatohepatitis and proinflammatory and prothrombotic factors playing a key role, which gives it clinical relevance and explains its importance as an entity associated with high vascular risk, factors that lead to an increase in morbidity and mortality of atherosclerotic origin.3
There is no pathognomonic diagnostic test for MS, so different societies and groups have developed a set of criteria for its diagnosis in clinical practice,4 since in its first definition the diagnosis focused on demonstrating insulin resistance (IR), which is a difficult parameter to measure in practice, but in 2001, the National Cholesterol Education Program (NCEP) Adult Treatment Panel III (ATP III), introduced criteria for the diagnosis of MS,5 which are among the most widely used at present and which we assume in this work.6
It has been found that the prevalence of this syndrome increases with aging, regardless of the concept applied, so, considering age as the main non-modifiable risk factor, it was considered of great importance to study the prevalence of MS in the population over 60 years old, since the combination of actions on several modifiable cardiovascular risk factors associated with MS could prevent atherosclerosis and reduce mortality significantly among older adults and the ¨Carlos Castellano Blanco¨ nursing home in the province of Pinar Del Rio, it was valued, because of the presence of older adults, which is a suitable scenario for this type of study, the main objective was to determine the incidence of metabolic syndrome in older adults in the nursing home ¨Carlos Castellano Blanco¨ of Pinar Del Rio province and then to determine the main causes of the appearance of metabolic syndrome in older adults belonging to the nursing home ¨Carlos Castellano Blanco¨ of Pinar Del Rio province.
METHODS
An observational, descriptive, cross-sectional study was carried out in the universe of 160 older adults of the Carlos Castellano Blanco Home for the Elderly in Pinar del Rio, in the period from January to September 2020, of which 54 have a diagnosis of Metabolic Syndrome in their clinical history, leaving a sample of 40 older adults who met the inclusion criteria established in the study, having a diagnosis of MS, age equal or older than 60 years and expressing informed consent and 14 patients with psychiatric diseases or mental disability and those who did not agree to participate were excluded.
The data were obtained by reviewing the medical records and the diagnosis of MS was made by the authors, according to the NCEP-ATP III,7) by the presence of at least three of the following criteria: Diabetes Mellitus, Arterial Hypertension, abdominal obesity, high triglycerides, low HDL. The diagnostic parameters were established according to the following criteria.
Diabetes Mellitus: It was diagnosed according to the criteria of the American Diabetes Association (ADA),8) which are those applied in our health services.
Arterial hypertension: Yes: BP≥130/85 mmHg for both sexes, or receiving antihypertensive treatment.
Abdominal obesity: If waist circumference in men >102 cm and in women >88 cm.
Elevated triglycerides: If: fasting blood values ≥1.70 mmol/L, or receiving pharmacological treatment for hypertriglyceridemia.
Low HDL-cholesterol: If: blood values <1.04 mmol/L in men and <1.29 mmol/L in women, or receiving drug treatment for hypercholesterolemia.
The laboratory techniques used for the determinations of the biochemical variables studied were carried out in the clinical laboratory of the Hospital Abel Santamaría, complying with quality control, the samples were processed by a certified laboratory technique in a Hitachi 192, after a 12-hour fasting period, the serum was obtained and the reagents used were produced by the Biologicals Production Company ¨Carlos J. Finlay. The kits and methods used for glycemia were the Rapigluco-Test kit, using the enzymatic colorimetric method of glucose oxidase; for cholesterol, the Colestestest kit was used, using the enzymatic method; triglycerides were determined with the Triglitest kit, using the enzymatic method, HDL-cholesterol was determined using the HDL-C Kit by colorimetric enzymatic method, end point and the determination of microalbuminuria was performed by the UMELISA MICROALBUMINA method, a heterogeneous sandwich enzyme-linked immunosorbent assay that uses ultramicroELISA strips as a solid phase.
Abdominal circumference was measured by the anthropometric method, using a 200 cm non-elastic tape measure. It was performed with the subject standing, at the midpoint between the lower costal ridge and the iliac crest, without compressing the skin with the tape, the feet were kept separated by a distance of 25 to 30 cm, in such a way that the weight was distributed over both lower limbs and the reading was taken at the end of a normal exhalation. To measure blood pressure, a KANGJU sphygmomanometer was used, with a previous rest of five minutes before measuring blood pressure.
The variable fatty liver was included in the study, using the abdominal ultrasound reports in the medical records of all patients, which confirmed its presence.
The patients were organized into three age groups: 60-69, 70-79 and 80-89 years.
The information was processed in Microsoft Excel, using descriptive statistics with absolute and relative frequencies and the Chi-square test (X2) to determine the relationship between variables. The principles of medical ethics were respected at all stages of the study.
RESULTS
that MS affected 34 % of the older adults belonging to the Carlos Castellanos Blanco Home for the Elderly.
The distribution of older adults with MS according to age and sex is shown in Table 1, with a higher proportion in the male sex (60 %) and in the 60-69 age group (62,5 %).
Table 1 Patients with MS according to age and sex.
| Age group | Sex | |||||
|---|---|---|---|---|---|---|
| Male | Female | Total n=40 | ||||
| No | % | No | % | No | % | |
| 60-69 | 16 | 40 | 9 | 22,50 | 25 | 62,50 |
| 70- 79 | 7 | 17,50 | 7 | 17,50 | 14 | 35 |
| 80-89 | 1 | 2,50 | 0 | 0 | 1 | 2,50 |
| Total | 24 | 60 | 16 | 40 | 40 | 100 |
Table 2 shows that AHT and elevated triglycerides were the most frequent components of MS, present in 62 and 60 % of the patients, respectively.
Table 2 Frequency of metabolic syndrome components.
| Components | Sex | Total n=40 | ||||
|---|---|---|---|---|---|---|
| Female | Male | |||||
| No. | % | No. | % | No. | % | |
| Abdominal obesity | 2 | 5 | 6 | 15 | 8 | 20,00 |
| Elevated triglycerides | 6 | 15 | 18 | 45 | 24 | 60,00 |
| Low HDL cholesterol | 1 | 2,50 | 0 | 0 | 1 | 2,50 |
| High blood pressure | 9 | 22,50 | 16 | 40 | 25 | 62,50 |
| DM TIPE 2 | 4 | 10,00 | 10 | 25 | 14 | 35 |
Source: medical records.
Table 3 shows the combinations of the components of MS in the older adults studied, the most frequent being the association of DM, HT and high TAG, present in 35 % of the cases. It is significant that the diagnosis of MS was made in 75 % of the patients with at least three of the criteria required by ATP III; nine patients had four criteria and only one of the elderly presented all five diagnostic criteria. DM and AHT were present in all the patients and in the most frequent combinations of MS components in the study we found obesity and DM and in the sample studied in particular all the obese patients studied had DM, but not all the diabetics were obese.
Table 3 Combination of Metabolic Syndrome components.
| Combination | Total n=40 | |
|---|---|---|
| No. | % | |
| DM + HT + Obesity | 8 | 20,00 |
| DM + HTA + elevated TAG | 14 | 35,00 |
| DM + Obesity + elevated TAG | 8 | 20,00 |
| DM + HTA + Obesity + elevated TAG | 8 | 20,00 |
| DM + HTA + Obesity + HDL bajo | 1 | 2,50 |
| DM + HTA + Obesity + elevated TAG + low HDL | 1 | 2,50 |
| TOTAL | 40 | 100 |
Source: Medical records.
The finding, from the abdominal ultrasound report, allowed establishing the presence of non-alcoholic fatty liver disease in 52 % of the elderly, as shown in graph 1.
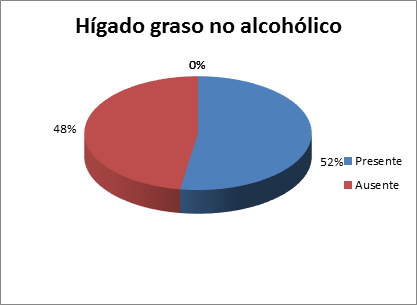
Table 4 shows that there was a predominance of older adults with MS without alterations in glycemic control and of male sex, and that there was no statistical significance in the relationship between both variables when applying the Chi-square test (X2).
Table 4 Glycemic control in older adults with MS according to sex.
| Age group | Sex n=40 | |||
|---|---|---|---|---|
| Male | Female | |||
| No | % | No | % | |
| With alterations in glycemic control | 10 | 25,00 | 4 | 10,00 |
| Without alterations of glycemic control | 14 | 35,00 | 12 | 30,00 |
Source: medical records. Significance: P > 0.05
Table 5 shows that 20 % of the male older adults had microalbuminuria, a variable that showed no relationship with the sex of the older adults.
DISCUSSION
The increase in the prevalence of metabolic syndrome (MS) worldwide is alarming, especially in older adults, in correspondence with the physiological changes typical of aging, the metabolism is much slower, free radicals increase, the functions of their organs decrease, such as the function of the pancreas, the arterial walls harden, factors that, together with inadequate lifestyles, increase the vulnerability to suffer from MS,7 Many studies in different countries, in Cuba and in the province of Pinar del Rio coincide with this statement.6
The prevalence by sex varies in the different stages of life, with many authors coinciding in the predominance of the female sex in post-climacteric ages; 9 which does not correspond with the result obtained in the research, in which the male sex predominated, a result that may be due to the fact that most of the adults in this institution belong to this sex and perhaps related to the fact that there are risk factors that occur more frequently in men than in women, such as sedentary lifestyle, smoking, which contribute to the appearance of diseases such as arterial hypertension and hyperlipidemia, which are diagnostic criteria of this entity.9
although other research carried out in Cuba has found a predominance of the male sex over the female, at a ratio of 1.8: 1 men for each woman, results attributed to male hypogonadism or androgen deficiency and visceral obesity, which have a complex and bidirectional relationship, the decrease in testosterone levels, due to a decrease in gonadotropin-releasing hormone and luteinizing hormone, secondary to fat aromatization, causes an increase in visceral obesity, which in the context of insulin resistance leads to the diagnosis of MS. (10,11)
It coincides with the study carried out in the province of Pinar del Rio by Perez Gonzalez and colls.,6 that the most significant component of MS found was HT, followed by hypertriglyceridemia, which was found in 60 % of the elderly with MS studied, These components of MS are interrelated in its pathogenesis, in which lipid deposition in the arteries, hypertrophy of the intimal layer of the vascular endothelium, vasoconstriction that appears as a consequence of the activation of the sympathetic nervous system, and renal sodium retention are involved.
Triglycerides transported by low density lipoproteins constitute the most useful lipid parameter when assessing coronary risk, they are transformed into LDL - oxidized, which is more immunogenic than native LDL, thus facilitating the deposition of cholesterol on arterial walls and the detection of immunocomplexes, which may be new diagnostic markers of coronary atherosclerosis and in turn of MS.12
Hypertriglyceridemia is an important alteration of lipid metabolism, with a wide range of clinical manifestations, which constitutes one of the most characteristic humoral alterations of MS and is an excellent marker of insulin resistance,3 which increases the synthesis of triglycerides and very low density lipoproteins (VLDL), which, together with deficient lipoprotein lipase activity, leads to hypertriglyceridemia This metabolic disorder impacts the lipoprotein pattern by favoring cholesteryl ester transfer protein activity, increasing the cholesterol ester content of VLDL and abnormally enriching HDL in triglycerides. HDL rich in triglycerides are more susceptible to degradation by hepatic lipase, which could explain the decrease in HDLc levels found in MS and small and dense LDL particles are formed, more atherogenic,4 alterations in plasma lipids that favor their deposition in the walls of the arteries, contributing to the development of atherosclerosis, which ends in a narrowing of the arteries, favoring the appearance of cardiovascular disease and arterial hypertension. Of the components of MS, low HDLc values were the least frequent in the sample studied, which coincides with Rivas et al.13
In the study only 20 % of the older adults with MS presented abdominal obesity, a result that could be related to the tendency to thinness of older adults and the lower presence in the combinations of low HDLc and abdominal obesity may be related to the reduction of adipose tissue that occurs with aging.
It is questioned whether the sum of the elements of MS increases the risk for the appearance of diseases, when compared with the effect of each one of them separately, in this respect it was considered that since the individual components of MS are clear risk factors, their simultaneous appearance increases the risk.
Insulin regulates a large part of the activities of adipose tissue and adipocytes constitute a cell type in which sensitivity to this hormone differs according to its levels, since the antilipolytic effect requires a notably lower concentration than that needed to stimulate glucose transport and even in states of IR in which glucose transport is altered, the antilipolytic effect is usually preserved, which maintains or even expands fat reserves.14
Insulin-stimulated glucose uptake is the key to the effectiveness of insulin in controlling blood glucose and therefore represents well what the level of insulin sensitivity is. Under physiological conditions there is a balance situation, which tends to be constant, between pancreatic insulin secretion and insulin sensitivity, and in healthy individuals there is great variability in both insulin effectiveness and insulin sensitivity and in the presence of insulin resistance the pancreatic beta cell, in an attempt to compensate for the product "insulin-stimulated glucose uptake" x "insulin secretion", will increase insulin secretion leading to hyperinsulinism, clinically ranging from normoglycemia through carbohydrate intolerance to non-insulin-dependent diabetes mellitus, when the islet beta cells do not respond with a sufficient increase in insulin secretion. 14
Chronic liver disease can be caused by simple steatosis or with inflammation and damage to the hepatocyte or steatohepatitis, its most severe manifestations are liver cirrhosis, hepatocarcinoma or hepatic insufficiency, Therefore, we attach special importance to the finding of more than 50 % of elderly patients with MS in the investigation with a diagnosis of non-alcoholic fatty liver disease, which requires a special follow-up of these patients, since age, steatohepatitis activity and fibrosis predispose to cirrhosis that in 10 years' time could lead to death in 12 to 25 % of the affected subjects. 15
In patients with steatosis, overproduction of VLDL represents a compensatory mechanism for hepatic lipid overload, which increases fasting dyslipidemia and the risk of atherosclerosis. This is accompanied by abnormal release of hormones and cytokines by adipose tissue, such as tumor necrosis factor alpha (tumour necrosis factor-α-TNF-α), IL-6, C-reactive protein, leptin, adiponectin and resistin, which is associated with dyslipidemia, oxidative stress, IR and hepatic inflammation.15
The lipotoxic hypothesis attempts to explain the mechanism by which fat infiltrates the liver through the unregulated influx of fatty acids.16 The massive, chronic, persistent and uncontrolled influx of free fatty acids into the hepatocyte overcomes the inhibitory effect of insulin on intracellular lipid oxidation and generates greater cellular resistance, fatty acids also interfere with insulin binding to its receptor and affect the intracellular propagation of the hormone signal by inducing serine phosphorylation of IRS-1.
Other mechanisms that favor IR facilitate the expression of proteins linked to the transcription and expression of genes related to the synthesis of triacylglycerides and to the production of an inflammatory response. New hypotheses state that in the context of IR, hepatic glucose production increases, because the ability of insulin to suppress gluconeogenetic enzymes is altered, an anomaly that coexists with an increase in triglyceride synthesis and reduced fatty acid oxidation. 16
Microalbuminuria is one such marker of abnormal urinary albumin excretion that has gained importance in the early recognition of at-risk individuals such as patients with type 2 diabetes mellitus (DM2) or hypertension (HT).17 In non-diabetic patients with essential hypertension, microalbuminuria is associated with higher blood pressures, elevated serum total cholesterol and reduced serum HDL-cholesterol, alterations related to a generalized dysfunction of the vascular wall, so that this association has allowed us to consider that "the kidney is the sentinel of the vasculature".18
Insulin resistance is the hallmark of MS, and is the underlying cause of the association with metabolic disturbances: hyperglycemia, dyslipidemias, and arterial hypertension, which would be fundamental factors in the development of atherosclerosis, and could also contribute directly to renal damage, due to alterations in normal hemodynamics and due to glomerular damage by multiple factors present in MS, such as Arterial Hypertension, hyperinsulinemia, hyperglycemia, hyperlipidemia and systemic inflammation, which would lead to renal damage, 18 which justifies the need to provide follow-up to microalbuminuria and other parameters that allow a more precise evaluation of metabolic control, as well as the complications that may accompany MS and implement intervention strategies designed for the prevention and early detection of MS, in older adults attended at the Carlos Castellano Blanco home for the elderly and in all communities.
CONCLUSIONS
The degenerative changes in older adults justify the high frequency and particularities of Metabolic Syndrome in them and the high risk of complications and mortality as could be observed in this study. Among the main components, there is an increase in triacylglycerides, arterial hypertension, diabetes mellitus, obesity and cholesterol, which imposes the need to create a group of actions for its adequate control.
BIBLIOGRAPHIC REFERENCES
1. Bolado García VE, Rivera Barragán MR, Soto Olivares MCV, Blasco López G, Romero Valdés LC. Componentes clínicos del Síndrome Metabólico. Rev. Méd Universidad Veracruzana [Internet]. 2015 [citado 14 Mar 2020]; 2(15): 67-89. Disponible en: Disponible en: https://www.medigraphic.com/pdfs/veracruzana/muv-2015/muv152e.pdf 1. [ Links ]
2. Reyes Sanamé FA, Pérez Álvarez ML, Céspedes Cuenca Y, Jiménez Rodríguez K, Fernández Mendoza A. Caracterización clínico epidemiológica de pacientes con síndrome metabólico. CCM [Internet]. 2019 [citado 5 mayo 2020]; 23(4): 2000-2020. Disponible en: Disponible en: http://www.revcocmed.sld.cu/index.php/cocmed/article/view/3365/1482 2. [ Links ]
3. Fundación del Caribe de la Investigación Biomédica (BIOS). Guía de Práctica Clínica "Síndrome Metabólico" [Internet]. Barranquilla: Fundación BIOS; 2015. [citado 14 Mar 2020]. Disponible en: Disponible en: http://www.fundacionbios.org/files/GPC%20SMET.PD 3. [ Links ]
4. Pereira-Rodríguez JE, Melo-Ascanio J, Caballero-Chavarro M, Rincón-Gonzales G, Jaimes-Martin T, Niño-Serrato R. Síndrome metabólico. Apuntes de interés. Rev Cu. Cardiol CirCardiov [Internet]. 2016 [citado 14 Mar 2020]; 22(2): 109-116. Disponible en: Disponible en: http://www.medigraphic.com/pdfs/cubcar/ccc-2016/ccc162i.pdf 4. [ Links ]
5. Herrera O. Síndrome metabólico en la infancia, un enfoque para la atención primaria. Rev cubana Pediatr [Internet]. 2015 Mar [citado 14 Mar 2020]; 87(1): 82-91. Disponible en: Disponible en: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S0034-75312015000100010 5. [ Links ]
6. Pérez González ME, Camejo Puentes M, Pérez Cardoso JJ, Díaz Llano PA. Síndrome metabólico en pacientes con diabetes mellitus tipo 2. RevCienc MédPinar del Río. 2016 [citado 14 Mar 2020]; 20(4): 414-420. Disponible en: Disponible en: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S1561-31942016000400005 6. [ Links ]
7. Castillo Castillo JL, Oscanoa Espinoza TJ. Dislipidemia como factor de riesgo para enfermedad cerebrovascular: estudio de casos y controles. Horiz. Med [Internet]. 2016 [citado 14 Mar 2020]; 16(4): 13-9. Disponible en: Disponible en: http://www.scielo.org.pe/scielo.php?script=sci_arttext&pid=S1727-558X2016000400003&lng=es 7. [ Links ]
8. Rivas Vázquez D, Miguel Soca PE, Llorente Columbié Y, Marrero Ramírez GM. Comportamiento clínico epidemiológico del síndrome metabólico en pacientes adultos. Rev CubMed Gen Integr [Internet]. 2015 [citado 14 Mar 2020]; 31(3). Disponible en: Disponible en: https://revmgi.sld.cu/index.php/mgi/article/view/57/http 8. ; [ Links ]
9. Vázquez Jiménez JG, Roura Guiberna A, Jiménez Mena LR, Olivares Reyes JA. El papel de los ácidos grasos libres en la resistencia a la insulina. Gac Med México [Internet]. 2017 [citado 6 sep 2020]; 153(7): 852-863. Disponible en: Disponible en: http://gacetamedicademexico.com/files/gmm_153_7_852-863.pdf 9. [ Links ]
10. Sapunar J, Aguilar Farías N, Navarro J, Araneda G, Chandía Poblete D, Manríquez V, et al. Alta prevalencia de dislipidemias y riesgo aterogénico en una población infanto-juvenil. Rev Med Chile [Internet]. 2018 [citado 14 Mar 2020]; 146: 1112-22. Disponible en: Disponible en: https://scielo.conicyt.cl/pdf/rmc/v146n10/0034-9887-rmc-146-10-01112.pdf 10. [ Links ]
11. Leiva AM, Martínez MA, Cristi-Montero C, Salas C, Ramírez-Campillo R, Díaz Martínez X. El sedenta rismo se asocia a un incremento de factores de riesgo cardiovascular y metabólicos independiente de los niveles de Actividad física. Rev Med Chile [Internet]. 2017 [citado: enero 2020]; 145(4): 458-467. Disponible en Disponible en http://dx.doi.org/10.4067/s0034-98872017000400006 11. [ Links ]
12. El Hadi H, Di Vincenzo A, Vettor R, Rossato M. Cardio-Metabolic Disorders in Non-Alcoholic Fatty Liver Disease. Int J Mol Sci [Internet]. 2019 [citado 14 Mar 2020]; 20(9). Disponible en: Disponible en: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6539803/pdf/ijms-20-2215.pdf 12. [ Links ]
13. Kim YM, Kim S, Kim SH, Won YJ. Clinical and Body Compositional Factors Associated with Metabolic Syndrome in Obese Koreans: A Cross-Sectional Study. Metabolic Syndrome and Related Disorders [Internet]. 2 de mayo de 2018 [citado 17 de octubre de 2020]; 16(6): 290-8. Disponible en: Disponible en: https://www.liebertpub.com/doi/10.1089/met.2017.0174 13. [ Links ]
14. Galiano Guerra G, Lastre Diéguez Y, Corrales García ME, Hernández Álvarez R, Japuz Cabrera D. Síndrome metabólico en pacientes hospitalizados en Servicio de Geriatría. Rev.Med.Electrón [Internet]. 2019 Jun [citado 2022 Abr 02]; 41(3): 628-640. Disponible en: Disponible en: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S1684-18242019000300628 14. [ Links ]
15. Peinado Martínez M, Dager Vergara I, Quintero Molano K, Mogollón Pérez M, Puello Ospina A. Síndrome Metabólico en Adultos: Revisión Narrativa de la Literatura. MedPub Journals [Internet]. 2021 [citado 2022 Abr 02]; 17(2): 4. Disponible en: Disponible en: https://www.archivosdemedicina.com/medicina-de-familia/siacutendrome-metaboacutelico-en-adultos-revisioacuten-narrativa-de-la-literatura.pdf 15. [ Links ]
16. Mendoza-Romo MÁ, Juárez-Antonio G, Fabela-Mendoza K, Medina-Tinoco A, Reyes Barbosa DL. Somatometria y características metabólicas del adulto mayor con y sin diabetes. Estudio comparativo. Rev Med UAS [Internet]. Octubre-Diciembre 2021 [citado 2022-04-02]; 11(4): 301-310. Disponible en: Disponible en: https://www.medigraphic.com/cgi-bin/new/resumen.cgi?IDARTICULO=106499 16. [ Links ]
17. Gonzalez Gonzalez LM, Cruzado Goicochea YS. Factores de riesgo que influyen en el Síndrome Metabólico en el adulto mayor del Centro de Salud Alto Trujillo, 2020. [Internet]. Trujillo Perú; 2020 [citado 2022 Abr 02]. Disponible en: Disponible en: https://repositorio.ucv.edu.pe/bitstream/handle/20.500.12692/67262/Gonzalez_GLM-Cruzado_GYS-SD.pdf?sequence=1&isAllowed=y 17. [ Links ]
18. Saquic Marta Julia Velásquez Velásquez, Deris Roselvy, Valdés de García Alba Marina. Frecuencia de síndrome metabólico en hombres y mujeres de 45-65 años que asisten al laboratorio clínico del Hospital Nacional de San Marcos. Rev. cient. cult [Internet]. 2021 [citado 2022 Abr 02]; 30(1). Disponible en: Disponible en: https://pesquisa.bvsalud.org/portal/resource/pt/biblio-1293332 18. [ Links ]
Received: August 26, 2022; Accepted: September 01, 2022

