










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Articulo
 texto en
texto en  Español (pdf)
Español (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkRevista de Ciencias Médicas de Pinar del Río
versión On-line ISSN 1561-3194
Rev Ciencias Médicas vol.27 no.3 Pinar del Río mayo.-jun. 2023 Epub 01-Mayo-2023
Articles
Efficacy of calendula in the treatment of chronic gingivitis
1University of Medical Sciences of Pinar del Río Stomatology Teaching Block. Faculty of Medical Sciences. Dr. Ernesto Guevara de la Serna. Pinar del Río, Cuba.
2University of Medical Sciences of Pinar del Río. Ormani Arenado Stomatology Teaching Clinic. Pinar del Río, Cuba.
3University of Medical Sciences of Pinar del Río. Turcios Lima Community Polyclinic. Pinar del Río, Cuba.
ABSTRACT Introduction: gingivitis is the most frequent periodontal disease affecting both adolescents and adult patients. Objective: to determine the efficacy of calendula in the treatment of chronic gingivitis. Methods: longitudinal study of therapeutic intervention in patients from 11 to 15 years old of the "Antonio Maceo" Mixed Center, of the "Hermanos Saíz" Teaching Stomatological Clinic, San Juan y Martínez municipality, in the period January 2020 - October 2021. 150 patients diagnosed with chronic fibroedematous gingivitis. By means of intentional sampling by expert criteria, the sample consisted of 40 patients who were divided into two groups (study and control) of 20 members each, treated with calendula mouthwashes and 0,2 % Chlorhexidine mouthwashes, respectively. The patients were evaluated 7,14 and 21 days after starting treatment. Percentage was used as a summary measure. Results: at seven days of treatment, all patients in the study group were cured while 65 % of the controls remained with mild gingivitis. At 14 and 21 days after starting treatment, all patients in both groups improved. Conclusions: the efficacy of 20 % diluted calendula tincture, used as mouthwash, was proved, since after seven days of treatment the patients were cured, without adverse reactions or recurrence of the disease, all attributable to the benefits provided by this product, including its
Key words: ADOLESCENT; GINGIVITIS; TRADITIONAL MEDICINE; PHYTOTHERAPY/treatmen.
INTRODUCTION
Periodontal diseases are among the most common affections of the human species; they occupy the second place among the health problems in stomatology, due to their prevalence and their effects, they are reported in world statistics, between 70 and 95 % of the adult population.1
They are defined as a chronic immunoinflammatory reaction of the protective periodontium (gingivitis) or attachment periodontium (periodontitis). Thus, chronic gingivitis is the most common form of periodontal disease occurring in childhood and its prevalence is considerable, increasing with age.1
The rates of gingivitis in men are 10 % higher than in women, regardless of age. Although ethnic differences are small, gingival inflammation is more prevalent in Caucasian subjects.2
Approximately 73 % of children between six and 11 years of age in developed countries suffer from gingivitis. Several studies have shown that the risk of suffering from gingivitis increases during puberty, between 50 and 90 %.3
In Cuba there is a high prevalence of gingivitis; it is almost always present in all its forms, it begins early in life from the age of five, continues until puberty, then gradually decreases until approximately 35 years of age, which is when there is an increase in the prevalence of destructive periodontal disease, becoming the leading cause of tooth loss.4
Chronic gingivitis affects approximately 80 % of school-age children, more than 70 % of the adult population has had either gingivitis or periodontitis or both.5
Treatment of patients with chronic gingivitis is aimed at controlling and/or eliminating the risk factors most responsible for the disease. Drug therapy includes caustic products, astringents, alkalinizers, epidermicides and the use of bactericidal substances such as 0,2 % aqueous chlorhexidine, in the form of mouthwashes, among others.6
Chlorhexidine has an anti-inflammatory action due to its detergent and antioxidant power. Its side effects are mild and transitory, including dental and tongue dorsum staining, taste alteration, mucosal erosion, lingual burning sensation, supragingival stimulation of calculus and very rarely parotid swelling; which limits its use in preventive dentistry.3
In the trends of contemporary medicine, the incorporation of Natural and Traditional Medicine to the professional practice in specialists of General Comprehensive Stomatology (EGI) stands out as a true scientific discipline that is necessary to study, improve and develop permanently due to its proven ethical and scientific advantages.7
In Cuba, a rescue work of natural therapies began in 1978 and organizational actions have been concentrated that allowed the development of other styles in the philosophy of medical thought, and they were inserted within the Cuban National Health System (SNS).7
Within traditional medicine, there is a group of plants that are used to combat periodontal disorders. The properties that make herbs beneficial for the treatment of the human body include anti-inflammatory, antimicrobial, astringent, stimulant, tonic, among others.8
Calendula officinalis L. is considered to originate from Egypt and has been cultivated in Europe since the 12th century; it has a high healing effect, anti-inflammatory, antimicrobial and immunomodulatory action. These remedies act to stimulate the body's natural healing response. Its toxicity and production costs are low.9
In Pinar de Río, in the year 2020, chronic gingivitis occupied an important place in the population due to the large number of people affected. The knowledge of phytotherapy as an attribute that can combat this oral disease is a goal to be achieved in the new model of stomatological care, which responds to the concept of General Comprehensive Stomatology, where the individual is considered as a biopsychosocial being influenced by different agents.
The high frequency of patients diagnosed with gingivitis, and the need to have alternative treatments of low toxicity and low cost, motivated the realization of this study, with the objective of determining the efficacy of calendula in the treatment of chronic gingivitis in patients from 11 to 15 years old of the Teaching Stomatological Clinic "Ormani Arenado", Pinar del Río municipality.
METHODS
A therapeutic intervention study was carried out on patients from 11 to 15 years old from the "Antonio Maceo" Mixed Center of the "Hermanos Saíz" Teaching Dental Clinic, San Juan y Martínez municipality, from January 2020 to October 2021.
The study universe consisted of 150 patients from 11 to 15 years old who were diagnosed with chronic fibroedematous gingivitis, i.e. gums increased in volume, hard-soft consistency, which may or may not present bleeding to stimulus, normal color, slightly hypercolored or bright red, in the study period.
By means of purposive sampling by expert judgment, the sample consisted of 40 patients. Patients from 11 to 15 years old, of both sexes, who started stomatological treatment at the "Hermanos Saíz" Teaching Stomatological Clinic of the San Juan y Martínez municipality with clinical diagnosis of chronic fibroedematous gingivitis and whose tutors accepted to collaborate with the research were included.
Patients affected psychically and emotionally, immunodepressed, with bronchial asthma or severe allergy that could present hypersensitivity to the medicine, patients with orthodontic treatment or severe dental crowding were excluded.
For a better study, two groups were formed, a study group (A) and another control (B) with 20 patients each, treated with calendula mouthwashes and 0,2 chlorhexidine mouthwashes, respectively.
The following variables were taken into account for this study: age, sex, risk factors, gingival index, treatment, days of treatment, clinical evolution according to gingival index and response to treatment.
Empirical scientific research methods were used, including observation, interview and documentary analysis.
Each patient was questioned and a thorough clinical examination was carried out in a dental chair with direct light by means of observation, palpation and exploration, using gloves, a flat oral mirror, tweezers, an explorer and a periodontal probe to identify the disease, its type and location.
The data of interest for the development of the research (general data, interrogation, physical examination and evolution) were collected from two fundamental sources:
The diagnosis of chronic gingivitis was based on the clinical characteristics and signs that describe the presence of chronic gingivitis, considering the presence of inflammation, bleeding, color, consistency and stippling, size, texture and contour, in addition to any other clinical findings of interest.
The degree of severity was determined by means of the Löe and Silness gingival index.10 using Williams millimeter probes, which allowed the evaluation of the evolution of gingival inflammation, using the following scales:
0. Normal gingiva (absence of inflammation).
1. Mild inflammation: slight color change, slight edema, no bleeding on probing.
2. Moderate inflammation: red, shiny, edematous gingiva, bleeding on probing.
3. Severe inflammation: red gingiva, edema, ulcerations, spontaneous bleeding.
To obtain the Gingival Index, the results for each tooth were added up, the sum was divided by four and the score for each tooth was obtained.
To determine the degree of severity of the disease, the numerical values of the gingival index were related to the different degrees of gingivitis as follows:10
To determine the effectiveness of the phytotherapy, to the study group (A), after polishing the dental surfaces, mouthwashes of Calendula officinalis L. (for one minute, three times a week and every other day) were applied: one teaspoon of 20% calendula tincture diluted in 120 ml of water, (it should only be used during the first 24 hours after its preparation).
The control group (B) was given 0,2 % aqueous chlorhexidine mouthwash, with the same conditions as the previous group.
After the application of the treatment, it was explained to the patients that they could not drink water for half an hour, not ingest food for two hours and not rinse their mouth immediately. Patients were trained to perform the treatment in case they could not attend the consultation.
Evaluation of the response
The clinical evolution of gingivitis was evaluated according to the gingival index after seven days of treatment, and to measure the response to treatment, the final evaluation was made according to the behavior of the gingival index at 7, 14 and 21 days, taking into account the following criteria:
1. cured: when at the days of evolution the Final Gingival Index was equal to 0 (IGF=0).
2. Improved: when the Final Gingival Index was lower than the Initial Gingival Index (IGF<IGI), but corresponding to a value greater than 0.
3. Equal: when after days of evolution, the Final Gingival Index value was equal to the Initial Gingival Index (IGF>IGI) or remained within the range shown by the IGI.
The patients in both groups were treated in a comprehensive manner, so they underwent all the treatments required in Primary Health Care, guaranteeing an initial preparation consisting of:
- Physical examination.
- Health education and motivation.
- Dentobacterial plaque control.
- Tartrectomy.
- Treatment of caries and defective fillings.
- Essential extractions.
Information processing
The information necessary for the study of each patient was recorded in a database structured by variables in Microsoft Excel spreadsheets.
Descriptive methods were used to determine relationships between the data, order, present and summarize the information in tables and graphs using absolute and relative frequencies.
Ethical aspects
All patients and guardians were provided with information about the study and its details. Autonomy, justice, beneficence, and nonmaleficence were guaranteed. Once this explanation was given, they were given the informed consent form (Annex 1) to sign if they agreed to participate in the research.
The study was conducted according to good clinical practice and the results obtained were used for strictly scientific, educational and social benefit purposes, and will only be disclosed in scientific events and published in prestigious journals.
RESULTS
Table 1. Distribution of the population according to age, sex and treatment groups.Teaching Stomatological Clinic "Hermanos Saíz", San Juan y Martínez, Pinar del Río. 2020 - 2021.
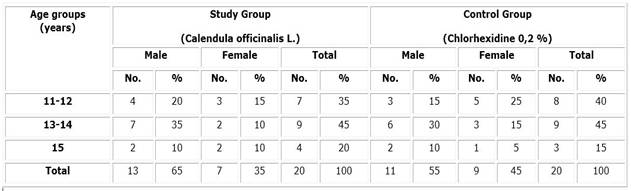
Table 1 shows the distribution of the selected sample in both study groups according to age and sex. Male patients predominated in both groups, 65 % in the study group and 55 % in the control group, and the 13-14 year-old group, which represented 45 % in both study groups.
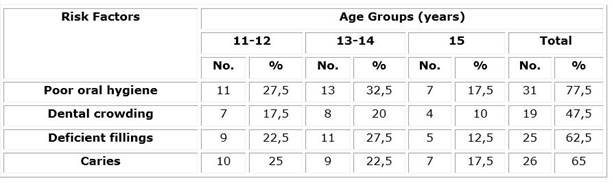
Table 2 shows the main risk factors for gingivitis in the sample studied, where it is evident that poor oral hygiene was the risk factor with the highest incidence and is directly related to the appearance of chronic gingivitis with 77,5 %, followed by dental caries with 65 %.
Table 3 Distribution of gingival index according to treatment groups.
| Gingival index | Study group (Caléndula officinalis L.) | Control Group (Chlorhexidine 0,2 %) | Total | |||
| No. | % | No. | % | No. | % | |
| Mild | 5 | 12,5 | 7 | 17,5 | 12 | 30 |
| Moderate | 9 | 22,5 | 8 | 20 | 17 | 42,5 |
| Severe | 6 | 15 | 5 | 12,5 | 11 | 27,5 |
| Total | 20 | 50 | 20 | 50 | 40 | 100 |
Table 3 shows the distribution of the sample according to study groups and gingival index after the initial preparation. Moderate gingivitis was the most represented in both groups, affecting 22,5 % of the patients in the study group and 20 % in the control group, followed by mild gingivitis with 12,5 % and 17,5 % respectively.
Table 4 Clinical evolution at seven days according to gingival index and treatment groups.
| Clinical evolution according to gingival index | Study Group (Calendula) | Control Group (Chlorhexidine) | Total | |||
| No. | % | No. | % | No. | % | |
| Healthy | 20 | 100 | 7 | 35 | 27 | 67,5 |
| Mild | 0 | 0 | 13 | 65 | 13 | 32,5 |
| Moderate | 0 | 0 | 0 | 0 | 0 | 0 |
| Severe | 0 | 0 | 0 | 0 | 0 | 0 |
| Total | 20 | 100 | 20 | 100 | 40 | 100 |
As can be seen in Table 4, seven days after starting treatment, all the patients in the study group were cured, while 65 % of the controls remained with mild gingivitis and only 35 % were cured.
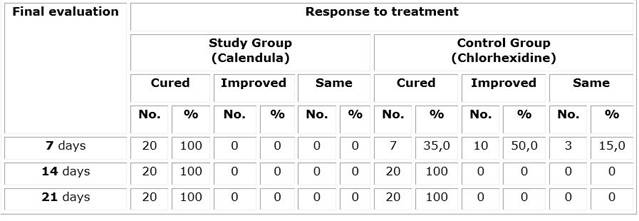
Table 5 shows that, 14 and 21 days after starting treatment, patients in both groups were cured. The effectiveness of the Calendula officinalis L. mouthwashes was also demonstrated in relation to the 0,2 % aqueous chlorhexidine mouthwashes, since at seven days, 100 % of those affected in the study group were cured, without the appearance of recurrence at 14 and 21 days, unlike the controls, with only 35,0 % cure at seven days, but with results similar to those of the first group at 14 and 21 days.
DISCUSSION
In line with our results (Table 1), Castro Yero et al.11) obtained a predominance of the male sex with 55,7 % in a study in which a population of adolescents with chronic gingivitis was characterized. These results also agree with research on the subject such as that of Rodríguez Moreno et al.3 where the most representative age range coincides with that of this study, as well as the male sex.
Different results were obtained by Pérez Ayala,6 and Pérez Barrero,12 who found a predominance of the female sex and patients aged 15 years and older. These authors consider that this predominance is influenced by the period of puberty, since hormonal changes may have repercussions on the clinical changes that occur in patients with chronic edematous and fibroedematous gingivitis.
The current prevalence of chronic gingivitis in Cuba is seven per hundred thousand in the male population and 2,8 in the female population. The incidence is 10 % higher in men than in women. It is suggested that this may be due to inadequate oral hygiene habits and infrequent brushing at an early age, which are considered risk factors for this disease and increase the severity of the pathology with increasing age.(2, 13)
The study of risk factors makes it possible to identify which adolescents are at high or low risk of becoming ill, and by acting on them, gingivitis can be prevented or controlled. Most of the adolescents have poor oral hygiene (Table 2), which is similar to that obtained (85,6 %) by Pérez Barrero,12 in his research.
Similarly, a predominance of deficient oral hygiene is obtained in studies carried out in Matanzas by Castro Yero, 11) in Sancti Spíritus with 78,7 %, followed by dental caries (47,5 %) and Villegas Rojas, 13) with 70,3 %.
The results differ from those published by Navarro Nápoles,1) where the predominant risk factor was dental crowding with 57,3 %, followed by defective fillings in 49,3 % and 30,7 % presented caries.
According to Sanchez Escalona et al.,9) dental plaque is eliminated by efficient brushing, which depends on adolescents, since oral hygiene care is not always a priority at this age through adequate forms and frequency of dentogingival brushing.
In the research of Pérez Ayala,6) the group of 15 years and older was the most representative, influenced by the period of puberty, since hormonal changes may have repercussions on the clinical changes present, both in patients with chronic edematous and fibroedematous gingivitis; results that coincide with those of Pérez Barrero et al.12
Despite the educational efforts that are made, periodontal diseases increase during adolescence as a consequence of the lack of motivation in the practice of oral hygiene. The predominance of the most severe forms in the study can be explained by the above.
According to the study by de Castro Yero,11) moderate gingival status prevailed in the adolescents studied (50,8 %) followed by mild (31,1 %), which is consistent with the results of this study (Table 3).
In the research by Rodríguez Moreno et al.,3 phytotherapy (Chamomile) vs. Chlorhexidine was used in the treatment of chronic gingivitis, coinciding with our study in terms of the gingival index at the beginning of treatment, with a predominance of the moderate degree in 50 % for the experimental group and 56,4 % for the control group.
This differs from that published by Sánchez Escalona et al.,9 in which the highest values were observed in the most severe form of the disease with 63,7 %, and mild gingivitis was not observed in any of the young people studied.
According to the literature consulted, mild chronic gingivitis is the most common classification, and studies carried out in Cuba, such as that of Martínez Barreiro,2 and Llerena Noda,4 report higher numbers of adolescents with mild gingivitis.
Likewise, Navarro Nápoles,1 and Pérez Ayala,6 in Santiago de Cuba, obtained a predominance of mild gingivitis, with 66,7 % and 77 % respectively. These results do not coincide with ours and may be due to the degree of health education that the Cuban population has at all levels of health, both to prevent the disease and to detect it early from the first level of care.
The favorable evolution of gingivitis to its less severe forms, since the beginning of the application of phytotherapy, can be justified by the proven anti-inflammatory action of calendula, for which the tripertenes and flavonoids present in it are responsible, as well as the antibacterial properties against staphylococci and streptococci, which makes the healing time shorter than in patients treated with conventional medicine.8,9
A similar investigation (table 4), was that of Pérez Ayala et al.:6 seven days after starting treatment with phytotherapy (Mangifera indica L.) in the form of mouthwashes, all patients were cured; while 62,0 % of the controls (Chlorhexidine 0,2 %), remained with mild gingivitis, and only 16,0 % were cured.
These results are also similar to those obtained by Serrano Corrales,14 in his study on the treatment of chronic gingivitis with ozone therapy where it was observed that after seven days, in the study group 24 % of the patients presented gums with normal characteristics, however in the control group, only 16 %.
In contrast to the present study, the study by Sánchez Escalona et al. 9 showed that seven days after starting treatment in the study group, changes in the disease were observed with a decrease in the severe form in 42,9 % and an increase in the moderate form with 57,0 %.
Regarding the clinical evolution of the lesion, in the study of Rodriguez Moreno et al. 3), the highest percentage of healing was evidenced between 12 and 14 days of treatment in both groups, with 30,6 % in those treated with 0,2 % chlorhexidine and 33,9 % in those who received phytotherapy, which does not coincide with our results.
The effects of Calendula officinalis and the use of phytotherapy in stomatology, in addition to its low price and no side effects, have been referred to in the specialized literature on several occasions with successful results; although there are no studies similar to the one presented here on the use of calendula in mouthwashes to make comparisons (Table 5).7,8,9
In the study of Rodríguez Moreno,3 after 6-7 applications, 33,8 % of the patients treated with phytotherapy (Chamomile), evolved towards cure while only 30,65 %, cured with Chlorhexidine 0,2 % in the same number of applications.
Pérez Ayala et al.,6 applied with good results phytotherapy in the form of mouthwashes in patients with chronic edematous and fibroedematous gingivitis using phytotherapy (Mangifera indica L.) in the study group, vs. 0,2 % Chlorhexidine in the control group, because after six days the lesions had disappeared in 80 % of those affected in the study group without presenting adverse reactions, demonstrating the efficacy of the treatment.
Sánchez Escalona et al.,9 observed changes in the disease with a decrease in the severe form in 42,96 % and an increase in the moderate form in 57,04 % seven days after starting the treatment of chronic fibroedematous gingivitis with homeopathic calendula, which proved to be more effective than with the conventional treatment.
The authors add.9 that:
"the evident improvement of adolescents treated with Calendula officinalis evolving towards healing of the lesion, confirms that, the higher the dilutions are made, the faster and more penetrating seems to occur the medicinal action that the preparation exerts on the state of the individual, cured without leaving noticeable damage".
According to the time of response to the treatment, in the study of Serrano Corrales et al.14 they observed that 21 days after the treatment, in the study group 92 % of the patients in which signs of gingivitis persisted were cured; while in the control group, it was effective only in 68 % of the patients.
These results are favorable, but, in the authors' opinion, they do not seem to be sufficiently effective in their response time to treatment, when compared with the results presented in the present investigation.
Therefore, it is concluded that the efficacy of 20 % diluted Calendula officinalis L. tincture, used as mouthwash, could be proved, since after seven days of treatment the patients were cured, without adverse reactions or relapses of the disease, all attributable to the benefits provided by this product, including its broad spectrum anti-inflammatory and antioxidant actions.
BIBLIOGRAPHIC REFERENCES
1. Navarro Nápoles J. Enfermedad periodontal en adolescentes. Rev Med Electrón. [Internet]. 2017 [citado 13/06/2022]; 39(1): 15-23. Disponible en: Disponible en: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S1684-18242017000100003&lng=es 1. [ Links ]
2. Martínez Barreiro LA, Gómez Nueva M, Labrada Estrada H, Dávila N, Martínez Pérez Y, Zamora León I. Prevalencia de la enfermedad gingival en adolescentes y su asociación con factores predisponentes. Manzanillo 2018. Multimed [Internet]. 2018 [citado 13/06/2022]; 22(6): 1200-1210. Disponible en: Disponible en: http://www.revmultimed.sld.cu/index.php/mtm/article/view/1046/1436 2. [ Links ]
3. Rodríguez Moreno A, ArciaCruz L, Moreno Diéguez O, Andrés Medina A, Rojas Pérez LM. Eficacia y seguridad de la tintura de manzanilla en el tratamiento de la gingivitis crónica edematosa. Multimed [Internet]. 2017 [citado 13/06/2022]; 20(5): 95-109. Disponible en: Disponible en: https://www.medigraphic.com/cgi-bin/new/resumen.cgi?IDARTICULO=70838 3. [ Links ]
4. Llerena Noda VY, Toledo Pimentel BF, VeitiaCabarrocas F, Barreto Fiu EE, Gutiérrez Álvarez I, Sasigaing Barreras A. La enfermedad periodontal inflamatoria crónica en jóvenes de la provincia de Villa Clara. Acta Médica del Centro [Internet]. 2016 [citado 13/06/2022]; 10(3): 19-26. Disponible en: Disponible en: http://www.revactamedicacentro.sld.cu/index.php/amc/article/view/681 4. [ Links ]
5. Zerón A. La nueva clasificación de enfermedades periodontales. Reva ADM [Internet]. 2018 [citado 13/06/2022]; 75(3): 122-4. Disponible en: Disponible en: https://www.medigraphic.com/pdfs/adm/od-2018/od183a.pdf 5. [ Links ]
6. Pérez Ayala O, Vigo Pérez Y, Vizcay Herrezuelo NL, Gutiérrez Torres D, Duarte Lisimón J. Eficacia del extracto de Mangifera indica L. en pacientes con gingivitis crónica edematosa y fibroedematosa. MediSan [Internet]. 2019 [citado 13/06/2022]; 23(06): 1023-34. Disponible en: Disponible en: https://www.medigraphic.com/pdfs/medisan/mds-2019/mds196d.pdf 6. [ Links ]
7. Bueno Rodríguez J, Álvarez de la Cruz M, García Vitar L, Suris Varona H. Eficacia de preparados de fitofármacos y apifármacos en las odontalgias. La Habana: Sociedad Cubana de Enfermería. Medicina Natural y Tradicional. Convención Tecnosalud Camagüey 2017 [Internet]. 2017 [citado 13/06/2022]: [aprox. 15 p.]. Disponible en: Disponible en: http://tecnosaludcmw2017.sld.cu/index.php/socoenf/tecnosalud2017/paper/view/98 7. [ Links ]
8. Rodríguez Cuellar Y, González Cardona Y, Camaño Carballo L, García Rodríguez B. Utilización de la fitoterapia por los estomatólogos. Clínica Estomatológica" Juan Manuel Márquez", municipio Playa, La Habana. Dilemas Contemporáneos: Educación, Política y Valores [Internet]. 2019 [citado 13/06/2022]; 6(s/n): [aprox. 12 p.]. https://www.dilemascontemporaneoseducacionpoliticayvalores.com/index.php/dilemas/article/view/1475 8. [ Links ]
9. Sánchez Escalona C, Pedroso Ramos L, Aneiro Díaz YR, Capdevila Gort SE. Efectividad de la caléndula homeopática como coadyuvante en el tratamiento de la gingivitis crónica fibroedematosa. Medimay [Internet]. 2022 [citado 13/06/2022]; 29(1): 85-94. Disponible en: Disponible en: http://revcmhabana.sld.cu/index.php/rcmh/article/view/2035 9. [ Links ]
10. González Díaz ME, Toledo Pimentel B, Corrales Álvarez M, Veitia Cabarrocas F. Diagnóstico, pronóstico y tratamiento de la enfermedad inmunoiinflamatoria crónica. Cap. 4. En: Colectivo de Autores. Compendio de Periodoncia. 2da ed. La Habana: Editorial Ciencias Médicas; 2017. p. 185-6, 190-2. [ Links ]
11. Castro Yero JL, Torrecilla Venegas R, Yero Mier IM, et al. Caracterización de la gingivitis crónica en la población adolescente. Universidad Médica Pinareña [Internet]. 2021 [citado 13/06/2022]; 17(1): e606. Disponible en: Disponible en: https://www.medigraphic.com/pdfs/revunimedpin/ump-2021/ump211l.pdf 11. [ Links ]
12. Pérez Barrero BR, Duharte Garbey C, Perdomo Estrada C, Ferrer Mustelier A, Gan Caldero B. Higiene bucal deficiente, hábito de fumar y gingivitis crónica en adolescentes venezolanos de 15-18 años. MEDISAN [Internet]. 2018 [citado 13/06/2022]; 15(9): 1-7. Disponible en: Disponible en: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S1029-30192018000900001 12. [ Links ]
13. Villegas Rojas IM, Díaz Rivero A, Domínguez Fernández Y, Solís Cabrera BA, Tabares Alonso Y. Prevalencia y gravedad de la enfermedad periodontal en pacientes diabéticos. Rev. Med. Electrón [Internet]. 2018 [citado 13/06/2022]; 40(6): 1911-30. Disponible en: Disponible en: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S1684-18242018000601911&lng=es 13. [ Links ]
14. Serrano Corrales A, Serrano Fernández D, Corrales León AL, Serrano Corrales A, Serrano Corrales A. Efectividad de ozonoterapia en tratamiento de gingivitis en adolescentes, Pinar del Río 2019. Rev. Ciencias Médicas [Internet]. 2021 [citado 13/06/2022]; 25(3): e4982. Disponible en: Disponible en: http://revcmpinar.sld.cu/index.php/publicaciones/article/view/4982 14. [ Links ]
Received: June 13, 2022; Accepted: February 06, 2023

