










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Articulo
 texto en
texto en  Español (pdf)
Español (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkRevista de Ciencias Médicas de Pinar del Río
versión On-line ISSN 1561-3194
Rev Ciencias Médicas vol.27 no.3 Pinar del Río mayo.-jun. 2023 Epub 01-Mayo-2023
Articles
Clinico-imaging-histopathological characterization of patients with astrocytic brain tumors
1University of Medical Sciences of Guantánamo. Dr. Agostinho Neto General Teaching Hospital Guantánamo, Cuba
2University of Medical Sciences of Santiago de Cuba. Saturnino Lora Clinical and Surgical Hospital. Santiago de Cuba, Cuba.
Introduction:
the term "brain tumor" refers to an unusual growth of tissue in the brain; all the structures that are part of the brain and its environment have cells that can grow in an uncontrolled way and produce tumor lesions.
Objective:
to characterize adult patients, with brain tumors of glial origin, attended at the General Teaching Hospital "Agostinho Neto", in the period 2017-2021.
Methods:
an observational, descriptive, cross-sectional study was conducted in patients diagnosed with astrocytic tumor. From a population of 80 patients, a probabilistic, simple random sample of 40 patients was taken. The variables included in the study were: age, sex, debut symptom, syndrome, Karnoftsky scale value, histological diagnosis, Kernohan classification, topographic localization, tomographic density, edema association, displacement of midline structures.
Results:
it is observed that in terms of age, patients older than 40 years old stand out (n=34 85 %), female (n=22 55 %). The most observed syndrome was endocranial hypertension (n=22 55 %). The most common histological diagnosis was glioblastoma multiforme (n=18 45 %). The tomographically predominant lesions in patients were larger than 50 mm (n=30 75 %). In the case of survival, most patients were deceased (n=30 75 %).
Conclusions:
It is concluded that brain tumors are an entity that, in the research presented, shows a higher incidence in women, with a tendency to have a large size, behaving as tomographically heterogeneous lesions.
Key words: GLIOMA; SURVIVORSHIP; BRAIN NEOPLASMS; ASTROCYTOMA
INTRODUCTION
The term "brain tumor" refers to an unusual growth of tissue in the brain, regardless of the nature and cause of the growth. Primary tumors of the brain may be benign and may be discovered by chance or because they cause symptoms, while others are cancerous (malignant).1
All the structures that form part of the brain and its environment have cells that can grow uncontrollably and produce tumor lesions. Depending on the speed of growth and the cells that originate it, the tumor will be more or less aggressive, which is why it is important the therapeutic design with radiotherapy or even chemotherapy. On the other hand, it must be taken into account that a very large tumor does not imply that its complete removal is impossible, depending on the nature and location of the tumor, as well as the clinical situation of the patient.1,2
The same rules apply to all cases: firstly, early diagnosis is essential for the treatment to be more effective and, secondly, the design of a correct treatment can achieve cure or significantly prolong life.3
The symptoms of brain tumors depend on the speed of growth of the tumor and its location. In general they can produce: alterations in the level of consciousness, with a tendency to sleep, which are more frequent in the most aggressive and rapidly expanding tumors, such as primary malignant brain tumors of rapid evolution. Personality alterations, such as apathy and lack of interest in relationships. They can also simulate depression.3,4
In the case of hemiplegia, the abrupt onset of a motor deficit may raise suspicion of stroke and is more characteristic of more aggressive tumors and metastases. Alterations of balance, loss of vision and headache which is usually more intense in the morning and does not respond adequately to analgesics. Epileptic seizures are more frequent in tumors of slow evolution, such as malignant tumors of low aggressiveness, although they can also appear in aggressive tumors. They may not produce any symptoms and may be a casual finding when performing a CT (Computed Axial Tomography) or MRI (Magnetic Resonance Imaging) for any other reason.5,6
In Spain, according to data from the population cancer registries that cover approximately 25 % of the Spanish population, primary CNS tumors represent 2 % of the total cancer in adults and up to almost 15 % in children under 15 years of age; which indicates that it is, at least in adults, an infrequent tumor with a higher incidence in men.7
In 2021, it is estimated that 83,570 people will be diagnosed with brain tumors and other CNS tumors in the United States (24,530 malignant tumors and 59,040 non-malignant tumors), and 18,000 people will die from the disease.8
In Mexico, brain tumors occupy the 19th place among all neoplasms, and the tenth among the most lethal. Worldwide, about 300,000 new cases are diagnosed each year, corresponding to 2,5 percent of cancer mortality, according to the globocan2018 statistical site, said Aliesha González Arenas, from the Institute for Biomedical Research (IIBm).9
In Cuba, mortality due to brain tumors in 2016 was 5,8 and 5,2 per 100,000 inhabitants for men and women respectively, with a higher mortality rate in the group aged 80 years or older for both sexes.10
The review of the studies developed in the localities where the hospital institutions are located are essential to know the development of diseases, in this case brain cancer. With regard to this statement, the results of this research on brain tumors of glial origin are proposed, since in Guantánamo there are few studies on the subject. The objective of this research was: to characterize adult patients, with brain tumors of glial origin, attended at the General Teaching Hospital Agostinho Neto, in the period 2017-2021.
METHODS
A descriptive, cross-sectional study was conducted in patients with the diagnosis of astrocytic tumor, belonging to the General Teaching Hospital "Agostinho Neto" in the period of 2017 -2021. This study, approved by the scientific council of the institution in the agreement 20/2022. Aiming to characterize patients with such nosological entities.
From a population of 80 patients, a probabilistic, simple random sample of 40 patients was taken.
The variables included in the study were: age, sex, debut symptom, syndrome, Karnoftsky scale value,6 histological diagnosis, Kernohan classification,7 topographic location, tomographic density, edema association, displacement of midline structures, treatment modality (surgical, chemotherapy, radiotherapy), time of evolution and status at discharge.
The data obtained were processed in a MicrosotfExcel database, then passed to the SPSS 23,0 statistical program for analysis and the results were entered in a Microsoft Word document for publication of the results.
The numerical variables (age, tomographic density, displacement of midline structures, time of evolution) were summarized as absolute frequency with its corresponding percentage, standard deviation (SD) and arithmetic mean (X). The rest of the categorical variables were only summarized as absolute frequency.
RESULTS
The mean age was 56,5 years, which deviates as average ±14,5 years in general, with a minimum value of 19 years and a maximum of 83 years. Particularly for each sex, in the female sex the mean age was 59,7 years which deviated as average ±13,1 years, in the case of the male sex the mean was 51,6 years which deviated as average 15,2 years.
Table 1 Patients according to age range and sex. General Teaching Hospital "Agostinho Neto" in the period of 2017 -2021.
| Age Range | Sex | Total | X | DT | ||||
|---|---|---|---|---|---|---|---|---|
| Female | Male | |||||||
| n | % | n | % | n | % | |||
| Less than 40 years old | 2 | 5,0 | 4 | 10,0 | 6 | 15,0 | 33,5 | 7,3 |
| Older than 40 years | 20 | 50,0 | 14 | 35,0 | 34 | 85,0 | 60,0 | 11,5 |
| Total | 22 | 55,0 | 18 | 45,0 | 40 | 100,0 | 0 | 0 |
In terms of age, patients over 40 years of age stand out (n=34 85 %), mainly those belonging to the female sex (n=22 55 %).(Table 1).
Table 2 Patients according to predominant symptom, syndrome and Karnoftky scale value.
| Predominant symptom | n= 40 | % |
|---|---|---|
| Headache | 16 | 40,0 |
| Seizure | 8 | 20,0 |
| Disorientation | 3 | 7,5 |
| Cognitive disturbances | 1 | 2,5 |
| Hemiplegia | 7 | 17,5 |
| Facial paralysis | 1 | 2,5 |
| Visual disorders | 2 | 5,0 |
| Vertigo | 1 | 2,5 |
| Vomiting | 1 | 2,5 |
| Syndrome | ||
| Cephalalgic syndrome | 7 | 17,5 |
| Confusional | 4 | 10,0 |
| Convulsive | 2 | 5,0 |
| Hemiplegic | 4 | 10,0 |
| Endocranial hypertension | 22 | 55,0 |
| Vertiginous | 1 | 2,5 |
| Value of the Karnoftsky scale | ||
| Greater than 70 points | 15 | 37,5 |
| Less than 70 points | 25 | 62,5 |
Headache (n=16 40 %) was the predominant symptom after seizure (n=8 20 %). The above approach also highlights that the most observed syndrome in patients was endocranial hypertension syndrome (n=22 55 %). The values of the Karnoftsky scale ranged from less than 70 points (n=25 62,5 %). (Table 2).
Table 3 Patients according to histological diagnosis, Kernoham classification value.
| Histological diagnosis | n=40 | % |
| Anaplastic astrocytoma | 4 | 10,0 |
| Fibrillary astrocytoma | 17 | 42,5 |
| Glioblastoma multiforme | 18 | 45,0 |
| Oligoastrocytoma | 1 | 2,5 |
| Kernoham classification value | ||
| Grade II | 18 | 45,0 |
| Grade III | 4 | 10,0 |
| Grade IV | 18 | 45,0 |
The most common histological diagnosis was Glioblastoma multiforme (n=18 45 %), with a Kernoham grade IV classification with an equal number of patients (n=18 45 %). (Table 3).
Regarding the size of the lesion the minimum value was 7,5 mm and the maximum was 109,8 mm, with a mean of 65,5 mm, which deviates as average ± 22,5 mm. In the case of midline deviation, the maximum value was 15 mm, with a mean of 6,1 mm, which deviates as average ± 4,3 mm.
Table 4 Patients according to tomographic characteristics
| Lesion size | n | % |
| Less than 50 mm | 10 | 25,0 |
| Larger than 50 mm | 30 | 75,0 |
| Tumor location | ||
| Cerebellum | 1 | 2,5 |
| Right frontal | 8 | 20,0 |
| Left frontal | 1 | 2,5 |
| Right hemispheric | 2 | 5,0 |
| Right occipital | 4 | 10,0 |
| Right parietal | 3 | 7,5 |
| Left parietal | 6 | 15,0 |
| Brain stem | 4 | 10,0 |
| Right temporal | 8 | 20,0 |
| Left temporal | 3 | 7,5 |
| Tomographic density | ||
| Hypodense | 2 | 5,0 |
| Hyperdense | 8 | 20,0 |
| Heterogeneous | 30 | 75,0 |
| Edema association | ||
| Associated edema | 10 | 25,0 |
| No associated edema | 30 | 75,0 |
| Deviation of structures from midline | ||
| No deviation + de 5 mm | 17 | 42,5 |
| If deviation +5 mm | 23 | 57,5 |
Table 4 shows that the predominant tomographic lesions in the patients were classified as larger than 50 mm (n=30 75 %), located mainly in the frontal and right temporal regions, with an equal number of patients in each location (n=8 20 %).
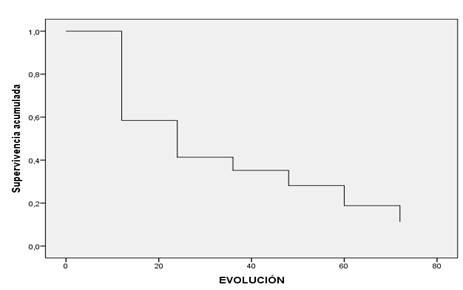
In the case of survival, most of the patients included in the study were deceased (n=30 75 %), with a mean survival time of 17,9 months, which deviates as mean ± 20,6 months, with a Confidence Interval (CI 8,5-23,8).
The survival function shows that 85 % of the patients die within the first 24 months of the disease (Fig. 1).
DISCUSSION
Cancer is an aggressive disease that bursts into the patient's life causing great havoc in all spheres, both personal and family, because from the very existence of this diagnosis, unpleasant expectations arise about the evolution of the life of the human being in question. These expectations change according to the age of the patient and the way of facing these adversities according to the degree of maturity experienced by the patient.
This study shows that, in the case of brain cancer, mainly in the stages of middle and older adulthood, the highest number of cases occur, Magdiely cols,1 in his article on the trend of cancer mortality in Mexico show similar results as they state that mortality rates begin to rise from 45 years in the case of brain tumors. Sierra,2 also agrees with this criterion in their study on the risk factors for the development of some types of cancer. The researchers agree with the results of the research reviewed, as they coincide with the classic literature on this condition.
In general, the male sex is the one with the highest number of patients with these conditions, since, secondary to different factors, such as oxidative stress, toxic habits, as well as the development of tasks that promote the development of brain tumors in patients, damage is produced at different levels that promote the appearance of brain tumor diseases. This fact takes its basis and is supported by research by Rodriguez et al,4 where they state that, for decades, men have been more likely than women to suffer from an aggressive form of brain cancer called glioblastoma.
There is also evidence that women tend to respond better than men to conventional therapy for this disease. The present study arose from the clinical observation that there is a large difference in the incidence of Glioblastoma between men and women and between boys and girls, Dr. Rubin said. Males are 60 % more likely overall to have Glioblastoma than females.
The findings of this research could be explained by the proportion of women in relation to men studied in this case, since it is perfectly understandable that a greater number of women in a research study increases the probability that they will suffer from the disease studied, which is brain cancer.
The symptoms related to the presence of intracranial expansive lesions, in this case brain tumors, have a wide compass, since they can present themselves in a varied range. Headache is a symptom common to a group of diseases, so much so that as a syndrome it groups together several nosological entities.
In this case, headache is the main symptom observed in most of the patients, a fact supported by different investigations, such as those shown by Ogawa,5 where he reveals that 52,5 % of the patients presented headaches as the initial symptom of the disease. Martínez Suarez,6 in his study about primary tumors of the central nervous system, also shows similar results, since in 84 % of the patients this was the most common symptom, authors like Oliva,7 are in partial agreement with the exposed in the investigation, since this symptom can be pathoneumonic of other diseases of the central nervous system, such as cerebrovascular diseases and sometimes heredodegenerative diseases, an attitude with which the researchers agree, since the present work is focused on the observation of the evolution of patients with brain tumors; it is not the objective of the same to abound with regard to other diseases.
The syndrome of endocranial hypertension is a common entity for multiple diseases, since the cranial cavity is, due to its closed configuration; the Monro-Kellie doctrine,8 refers that the various components found in the intracranial cavity give rise to an intracranial pressure (ICP), which may vary according to various life situations. Abnormal variations in ICP are mostly due to mass effects caused by alteration of one of the three intracranial components. It has been observed that the timely recognition of these alterations will be determinant for the prognosis.
In the case of brain tumors the increase is at the expense of the encephalic mass and causes different disorders in the cerebral economy. This is evidenced by the symptomatological compass described above that patients present, studies such as those of Gutiérrez Crespo,9 and Rojas Carvajal,10 show similar results in each of their investigations, as they describe brain tumors as the first cause in their study of endocranial hypertension syndrome, this was presented in these investigations in more than 80 % of patients. The researchers agree with these findings, since this criterion is reinforced by the international literature and is evidenced in the research in question.
The Karnoftsky scale measures the patient's condition according to the patient's functionability; the lower the patient's score, the better the prognosis. Especially in patients who undergo high-risk surgeries such as tumor surgeries, and even more so in the case of neurosurgical surgeries. Patients with brain tumors tend to have a low score, because due to the characteristics of the lesion in this case, highly infiltrative, in the brain, there is a gradual or abrupt loss of the patient's vital functions, especially the cognitive ones, which give way to the progressive deterioration suffered by patients with brain tumors. This research supports the aforementioned, due to the low values of the patients when examining the measurements of said functional scale.
In research developed by Solomon Cardona,11 after a review of the literature carried out by the author, it shows that with the evolution of the intracranial glial expansive lesion there is a decrease in the Karnofsky scale of the patient. De Hollanda,12 shows similar results to the previous research, Ruidiaz,13 in his study about tractography for the intervention of patients with glial tumors also shows that patients had low values of functionability in the Karnofsky scale. The researchers concur with the findings of these investigations, there is a tendency for patients with glial brain tumors to have low values on the Karnofsky scale.
Among the glial tumors, the most common is glioblastoma multiforme, the tumor with the highest degree of malignancy of the central nervous system, there is a uniformity according to the international community on the subject. Hernández Cortés,14 in his characterization of patients with brain tumors, shows results similar to those described in this research, since he states that when developing his study, glioblastoma multiforme occurred more frequently in both sexes and in all age groups. Urbańska 15 coincide with the opinion of Hernández Cortés,14 since in their studies, after reviewing several articles they observed that more than 50 % of the patients diagnosed with brain tumors were diagnosed with Glioblastoma multiforme. The researchers agree with the previous studies, which is in agreement with the reference literature on the subject.
The diagnostic means, although they serve in essence as a way of contrasting the hypothesis raised by the health personnel, when providing care to a patient, constitute an effective weapon for the early and timely diagnosis of brain tumors, with these can be issued the necessary data for the approach of brain tumor diseases, the size of the lesion is an important data when the neurosurgeon considers a therapeutic strategy. This research describes that most lesions were larger than 50 mm. Studies carried out by Suchorska,16) show that preoperatively the patients had an average tumor volume of more than 5 cm, an observation with which the researchers agree, since these tumors present a high aggressiveness.
The localization of brain tumors opens a gap for the medical personnel who provide care to these patients, because according to this, an arsenal of therapeutic procedures is deployed that can help at the moment of approaching the lesion. In the case of the research presented, it is observed that they occur mostly in the frontal and temporal lobes. Studies carried out by Estupiñán 17) coincide with what is presented in this research, since in their results they show concordance with the results of this research, since most of the patients reported had lesions in the temporal lobe. Esquivel Tamayo,18) in his study about brain tumors in Las Tunas shows similar results to those exposed also but in this case the tumors were located mostly in the temporal lobe with 14 patients that represented 33,44 % of the sample, as well as Días,19) where he shows that in 44 % of the patients the lesion was presented in the frontal lobe.
Imaging studies are important for the diagnosis of brain tumor lesions, in this study, there is a tendency for most of the lesions to be heterogeneous, a fact with which Salek,20) agrees, as this is given by the degree of malignancy and hypercellularity of these tumors, This is also associated with the mass effect that these tumors produce inside the cranial cavity, which in this case is aggravated, causing deviations of the midline and the presence of edema that aggravates the symptomatological picture.
Siero Almonte,21) in his study of the imaging characteristics of intracranial space-occupying lesions, shows that all high-grade malignant astrocytomas have associated edema and therefore deviation of the midline structures. Researchers agree with the above, since it is a characteristic of these entities to cause the picture described above.
In general, most patients with astrocytic brain tumors have a survival of less than 24 months, a fact that is shown in this study, Gómez Vega,22) agrees with the above described, in his study about the survival of primary brain tumors in Colombia, shows that according to the histological subgroup, the most frequent in ascending order were glial lesions, embryonal tumors and ependymal tumors, of which the predominant histological subtypes were astrocytoma, medulloblastoma and ependymoma. The overall survival at six months, one year, two years and three years was 49 %, 35 %, 21 % and 15 %, respectively.
It is concluded that brain tumors are an entity that, in the research presented, shows a higher incidence in women, with a tendency to have a large size, behaving as tomographically heterogeneous lesions. They cause higher mortality in the first 24 months after diagnosis.
BIBLIOGRAPHIC REFERENCES
1. Magdiel L, Rodríguez V, Rojas I, Cáceres Lavernia H, González González J, Cruz Pérez P, et al. Characterization of central nervous system tumors in patients cared for in HermanosAmeijeiras Clinical-Surgical Hospital. Actamedica [Internet]. 2021 [citado 03/06/2022]; 20(2): e07. Disponible en:Disponible en:https://www.medigraphic.com/pdfs/actamedica/acm-2019/acm192g.pdf 1. [ Links ]
2. Sierra Benítez EM, León Pérez MQ, Molina Estévez ML, Guerra Sánchez R, Hernández Román G. Meningiomas intracraneales. Experiencia de dos años en el servicio Neurocirugía de Matanzas. Rev.Med.Electrón. [Internet]. 2019 Dic [citado 28/06/2022]; 41(6): 1367-1381. Disponible en: Disponible en: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S1684-18242019000601367&lng=es 2. [ Links ]
3. NCI. Estudio revela diferencias de sexo en el glioblastoma [Internet]. Instituto Nacional del Cáncer; 2019. [citado 06/06/2022]. Disponible en: Disponible en: https://www.cancer.gov/espanol/noticias/temas-y-relatos-blog/2019/glioblastoma-tratamiento-respuesta-diferencia-por-sexo 3. [ Links ]
4. Rodríguez MPT, Garcia KAM, Cruz A del PI, Baquero CAC. Inmunopatología del Glioblastoma Multiforme y su importancia en el ámbito clínico. Revista Ciencias Biomédicas [Internet]. 2022 Apr 15 [citado 28/06/2022]; 11(2):163-78. Disponible en: Disponible en: https://revistas.unicartagena.edu.co/index.php/cbiomedicas/article/view/3738 4. [ Links ]
5. Ogawa J, Pao GM, Shokhirev MN, Verma IM. Glioblastoma Model Using Human Cerebral Organoids. Cell Reports [Internet]. 2018 Apr [citado 28/06/2022]; 23(4): 1220-9. Disponible en: Disponible en: https://www.sciencedirect.com/science/article/pii/S2211124718304819 5. [ Links ]
6. Martínez-Suárez C. Diagnóstico de tumores cerebrales primarios en el Hospital Universitario: “Gustavo Aldereguía Lima”, Cienfuegos. Gaceta Médica Estudiantil [Internet]. 2022 [citado 11/06/2022]; 3(2): e217. Disponible en: Disponible en: http://www.revgacetaestudiantil.sld.cu/index.php/gme/article/view/217 6. [ Links ]
7. Oliva J, Betancourt M, Cárdenas R, Bell L, Ferrán S, Gutiérrez S, et al. Estudio de los tumores broncopulmonares con Ga- 67-citrato. Informe preliminar. Revista Cubana de Medicina [Internet]. 2020 [citado 28/06/2022]; 18(3). Disponible en: Disponible en: http://revmedicina.sld.cu/index.php/med/article/view/1288 7. [ Links ]
8. Galofre-Martínez MC, Puello-Martínez D, Arévalo-Sarmiento A, Ramos-Villegas Y, Quintana-Pájaro L, Moscote-Salazar LR. Doctrina Monro-Kellie: fisiología y fisiopatología aplicada para el manejo neurocritico. Revista Chilena de Neurocirugía [Internet]. 2019 Oct 4 [citado 08/06/2022]; 45(2): 169-74. Disponible en : Disponible en : https://revistachilenadeneurocirugia.com/index.php/revchilneurocirugia/article/view/131/118 8. [ Links ]
9. Gutierrez-Crespo P, López-Arbolay O, Cruz-Pérez P, Ortiz-Machín M. Lesiones de la región pineal. Resultados del tratamiento multimodal. Anales de la Academia de Ciencias de Cuba [Internet]. 2022 [citado 11/06/2022]; 12(2): e1142. Disponible en: Disponible en: http://revistaccuba.sld.cu/index.php/revacc/article/view/1142 9. [ Links ]
10. Rojas Carvajal CM, Meneses Gil MX. Hipertensión intracraneal en Colombia en 2010-2018: carga de enfermedad [Tesis]. Universidad El Bosque; 2020 [citado 11/06/2022]. Disponible en: Disponible en: http://hdl.handle.net/20.500.12495/4232 10. [ Links ]
11. Solomón-Cardona M, Estupiñán-Díaz B, Hernández-Díaz Z, de-la-Paz-Bermúdez T, Quintanal-Cordero N, Gómez-Suárez H. Glioblastoma de células granulares supratentorial hemisférico. Presentación de caso y revisión de la literatura. Anales de la Academia de Ciencias de Cuba [Internet]. 2022 [citado 11/06/2022]; 12(2): e1184. Disponible en: Disponible en: http://revistaccuba.sld.cu/index.php/revacc/article/view/1184 11. [ Links ]
12. De Hollanda BC. Funcionalidade de idososcom diagnóstico de cânceratravés da Escala de Desempenho de Karnofsky / Functionality of elderlypeoplediagnosedwithcancerusingtheKarnofsky Performance Scale. Brazilian Journal of Health Review [Internet]. 2021 Jun 28 [citado 11/06/2022]; 4(3): 14098-106. Disponible en: Disponible en: https://scholar.archive.org/work/dae23qnubzh4rfatyakpuzyh2q/access/wayback/https://www.brazilianjournals.com/index.php/BJHR/article/download/32006/pdf 12. [ Links ]
13. Ruidiaz AA, López LBL, Sufuentes SV, Cid PA, Pellejero JC, Herbera JM. Aplicación de la tractografía en la resección de tumores gliales. Atalaya Médica Turolense [Internet]. 2021 [citado 11/06/2022]; (22): 37-46. Disponible en: Disponible en: https://dialnet.unirioja.es/servlet/articulo?codigo=8235074 13. [ Links ]
14. Hernández Cortés N, Hernández Cortés K, Pérez Hernández H. Caracterización clínica, epidemiológica y anatomopatológica de los tumores cerebrales supratentoriales y su morbilidad posanestésica. Rev Cubana Med Gen Integr [Internet]. 2021 Jun [citado 11/06/2022]; 37(2): e1366. Disponible en: Disponible en: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S0864-21252021000200009&lng=es 14. . [ Links ]
15. Urbańska K, Sokołowska J, Szmidt M, Sysa P. Review Glioblastomamultiforme - an overview. WspółczesnaOnkologia [Internet]. 2014 [citado 11/06/2022]; 18(5): 307-12. Disponible en: Disponible en: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4248049/ 15. [ Links ]
16. Suchorska B, Jansen NL, Linn J, Kretzschmar H, Janssen H, Eigenbrod S, et al. Biological tumor volume in 18FET-PET before radiochemotherapy correlates with survival in GBM. Neurology [Internet]. 2015 Jan 21 [citado 11/06/2022]; 84(7): 710-9. Disponible en: Disponible en: https://pubmed.ncbi.nlm.nih.gov/25609769/ 16. [ Links ]
17. Estupiñán DBO, García MI, Morales CLM, et al. Tumores cerebrales en el programa de cirugía de la epilepsia del Centro Internacional de Restauración Neurológica (La Habana). Rev Cubana NeurolNeurocir [Internet]. 2017 [citado 13/06/2022]; 7(1): 25-33. Disponible en: Disponible en: https://www.medigraphic.com/cgi-bin/new/resumen.cgi?IDARTICULO=76767 17. [ Links ]
18. Esquivel-Tamayo J, Ponce-de-León-Norniella L. Caracterización clínico-epidemiológica de los pacientes diagnosticados de cáncer cerebral en la provincia de Las Tunas. EsTuSalud [Internet]. 2021 [citado 13/06/2022]; 3(1): e61. Disponible en: Disponible en: http://www.revestusalud.sld.cu/index.php/estusalud/article/view/61 18. [ Links ]
19. Dias A. Aplicación de puntos craneométricos y neuroimágenes en la cirugía cerebral tumoral [Internet]. Auditorio Ramón Carrillo del Hospital de Alta Complejidad en Red El Cruce; 2018 [citado 13/06/2022]: 24-33. Disponible en: Disponible en: http://repositorio.hospitalelcruce.org/xmlui/handle/123456789/788 19. [ Links ]
20. Salek DMB, Velasco DMR, González DRS, Velasco DPS, Miguel DEN, Jimenez DJR. “Abordaje del reto de realizar un correcto diagnóstico diferencial de LOES cerebrales con patrón de realce en anillo.” Seram [Internet]. 2021 May 18 [citado 14/06/2022]; 1(1). Disponible en: Disponible en: https://piper.espacio-seram.com/index.php/seram/article/view/4414/2880 20. [ Links ]
21. Almonte SS, González TP, Llane MR, Carbonel CLA, Musa M. Diagnóstico de masas intracraneales primarias por medio imagenológicos. Revista de Ciencias Médicas de Pinar del Río [Internet]. 2012 Mar 1 [citado 17/06/2022]; 16(1): 44-53. Disponible en: Disponible en: http://www.revcmpinar.sld.cu/index.php/publicaciones/article/view/868/1588 21. [ Links ]
22. Gómez Vega JC, Ocampo Navia MI, de Vries E, Feo Lee OH. Sobrevida de los tumores cerebrales primarios en Colombia. Univ. Med. [Internet]. 2020 Sep [citado 16/06/2022]; 61(3): 80-90. Disponible en: Disponible en: http://www.scielo.org.co/scielo.php?script=sci_arttext&pid=S2011-08392020000300080&lng=en 22. [ Links ]
Received: June 28, 2022; Accepted: March 14, 2023

