










 Servicios personalizados
Servicios personalizados Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
The first clinical feature usually expected of transverse maxillary deficiency is the posterior cross bite and/or the dark spaces that appear during the smile among the upper dental arch and the lips commissures.1,2
This is a logical thought because in these cases, cause and consequence are on the same spatial axis. However, the extreme complexity of the human stomatognathic system does not allow simplifying problems to a single axis. The transverse deficiency, depending on its magnitude, will invariably be accompanied by vertical and anteroposterior alterations.
Many class II and class III malocclusions, as well as increased facial divergence, are related to maxillary constriction. From the dental point of view, it is common to find problems such as crowding and dento-alveolar protrusion, as a result of the discordance between the basal bone and the teeth size.3
The narrow upper arch resulting from maxillary deficiency causes a negative transverse discrepancy in relation to the lower arch. However, this type of problem is not exclusive to maxillary defects. It can be found in patients with transversely optimal and even increased measurements. Occasionally, a large and lowered tongue is capable of over-expanding the lower arch and causing a posterior crossbite.4
From the orthopedic point of view, the contraction of the lower arch is not feasible and the therapeutic action is enclosed to limited orthodontic movements. For this reason, when the transverse excess of the lower arch is the cause of the discrepancy, it can be assessed, depending on the wide range of aesthetically and functionally acceptable variations, whether the best therapeutic approach is to tolerate the posterior crossbite or to perform an over expansion of the upper arch.5)
Regarding the surgical solution, mandibular constriction by means of a midline osteotomy can be a useful tool to treat transverse discrepancies of the maxilla, as long as it is also performed a bilateral sagittal osteotomy. It has been described as a stable, relatively simple, and innocuous treatment for the temporomandibular joints and the periodontium adjacent to the osteotomy line.6,7 However, compared to surgically assisted maxillary expansion, it is a surgery that is not frequently used, possibly due to the limited experience and very few literature available.8
Given that the solution to the discrepancy is more feasible from dimensional changes of the upper arch, regardless of the therapeutic method (orthopedic or surgical) and the origin of the anomaly (maxilla or mandibular), it is productive to take the maxilla as a reference to describe disharmony. The term “negative maxillary transverse discrepancy” (NMTD) could be used to refer to any problem of skeletal origin that causes transverse incompatibilities between the arches; either upper default or lower excess.
Although the characteristics of maxillary deficiency are well described, this is not the case when the origin of the transverse problem is given by an excess in width of the mandible. In this way, the following question arises: what are the differences between NMTD with narrow jaws in relation to those with jaws whose width is adequate or increased? Taking into account the previous scientific problem and its potential clinical and investigative importance, the aim of this work was to describe the cephalometric differences between both types of NMTD.
Methods
An observational, comparative and cross-sectional study was carried out in the Maxillofacial Surgery Department of “Hermanos Ameijeiras” Clinical Surgical Hospital. The universe included clinical records of patients with NMTD whose treatments plan included surgically assisted maxillary expansion. Cases with loss of permanent teeth, presence of a craniofacial syndrome, or mental disability duly detected by the clinical psychologist of the multidisciplinary team were excluded. For the current study, 17 medical records were selected from patients assessed in consultation during the period of January 2016-January 2020.
The initial plaster models were measured to obtain the distance between the central fossae of the upper first molars in each patient and 47 mm was established as the correct measurement, according to the Mayoral9 method. Based on these values, the sample was divided into two groups:
Group A: Patients with decreased maxillary transverse dimension (distance between 16 and 26 <47 mm) for a total of 10 cases.
Group B: Patients with normal or increased maxillary transverse dimension (distance between 16 and 26 ≥ 47 mm) for a total of 7 cases.
From the initial lateral digital skull teleradiographs and using Facad version 3406 software, the cephalometric analysis of Ricketts, McNamara, Björk & Jarabak, Burstone and the soft profile of Burstone & Legan were performed.10 Continuous quantitative study variables were obtained, corresponding to the measurements of the respective cephalograms. In the age adjusted measurements of the Ricketts cephalogram, the value of the norm was calculated at 16 years. No standard was established for the mandibular length of the McNamara cephalogram, since it depends on the individual maxillary length.
To collect and process the information, a database was created in the statistical package IBM SPSS-PC version 20.0, through which the minimum, maximum, arithmetic mean and standard deviation of each variable were established in both groups.
The one-sample binominal test was applied to find out if the distribution of patients between both groups occurs with the same probability. To test the null hypothesis (H0) that there were no differences between group A and B regarding the distribution of cephalometric measurements, the non-parametric Mann Whitney U test of independent samples was applied. The variables where H0 was rejected with a significance level (p) lower than 0.05 were selected.
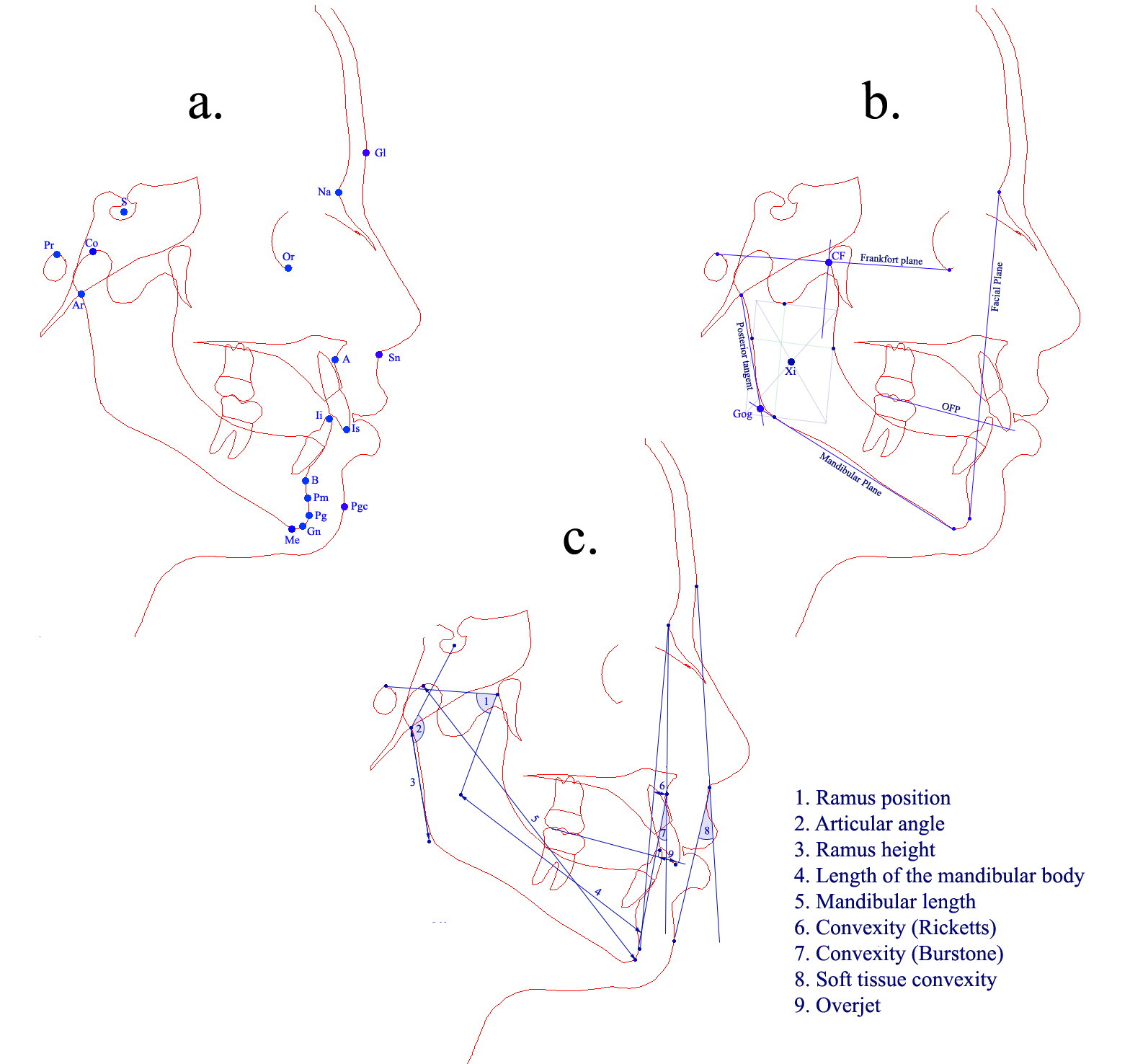
The landmarks and lines (skeletal and of the profile) used in the cephalometric analyses are represented in Figure 1, (sections a and b):
Landmarks:
Porion (Pr): the most superior point of the outline of the external auditory meatus.
Orbital (Or): the lowest point on the inferior orbital rim.
Facial center (CF): the geometric point located at the intersection of the Frankfort plane and the perpendicular to it that passes tangent to the posterior wall of the pterygo-maxillary fissure.
Mandibular centroid (Xi): the geometric point of the mandibular ramus located according to the procedure established in the Ricketts cephalogram.
Sella (S): the geometric center of the pituitary fossa (sella turcica).
Articulare (Ar): the point where the posterior border of the neck of the condyle intersects the inferior border of the sphenooccipital massif.
Geometric Gonion (Go): the intersection of the tangent to the posterior border of the ramus and the mandibular plane.
Condylion (Co): the most posterior superior point on the head of the mandibular condyle.
Point A maxilla (A): the deepest point of the curvature of the maxilla between the anterior nasal spine and the edge of the dental socket.
Mandibular point B (B): the deepest point of the anterior mandibular contour, between the dental alveolus and the symphysis.
Suprapogonion (Pm): the point where the curvature of the anterior edge of the symphysis changes from concave to convex.
Pogonion (Pg): the most anterior point of the contour of the mandibular symphysis in the midsagittal plane.
Gnathion (Gn): the most anteroinferior point of the anterior border of the mandibular symphysis.
Chin (Me): the lower point of the symphysis contour.
Glabella (Gl): the point of the most anterior cutaneous profile of the frontal region.
Subnasal (Sn): the point of the most posterior and superior cutaneous profile of the nasolabial curvature.
Cutaneous pogonion (Pgc): the point of the most anterior profile of the cutaneous chin.
Lines
Frankfort plane: Line drawn from points Pr and Or.
Tangent to the posterior border of the ramus: Line drawn from the articular point and passing tangent to the posterior border of the mandibular ramus.
Mandibular plane: Line drawn from point Me and passing tangent to the lower edge of the mandibular ramus.
Facial plane: Line drawn from points Na and Pg.
Occlusal functional plane (OFP): Line established between the most distal inter-occlusal contact point of the first molars and the midpoint of overbite of the canines.
The variables where Ho was rejected were classified by the authors into 4 categories and described as fallow (figure 1, section c):
Cranio-mandibular relationship:
Ramus position (Ricketts): Angle formed between the points Pr-CF-Xi.
Articular angle (Björk & Jarabak): Angle formed between the S-Ar-Go points.
S-Ar / Ar-Go ratio (Björk & Jarabak): Result of the division of the distances established by the points S-Ar and Ar-Go.
Mandibular anatomy:
Ramus height (Björk & Jarabak, Burstone): Distance between points Ar and Go.
Length of the mandibular body (Ricketts): Distance between Xi and Pm, prolonged up to the A-Pg line.
Mandibular length (McNamara): Distance between points Co and Gn.
Mandibular maxillary relationship:
Convexity (Ricketts): Distance between the facial plane line and point A.
Convexity (Burstone): Angle between the lines N-A and A-Pg.
Wits: Distance between points A and B, projected on the OFP. It takes negative values when B is ahead of A.
Mandibular-maxillary difference (McNamara): Is the result of the substraction between the value of the mandibular length and the value of the maxillary lenght (distance between points Co and A).
Soft tissue convexity (Burstone & Legan): Angle formed between the Gl-Sn and Sn-Poc lines.
Oclusal relationship
In the preparation of this study, the use of informed consent was not necessary, as it was a study of data collection from information sources. All kinds of personal identifiers were bypassed. Each case was assigned an unrelated consecutive number to facilitate statistical work. In this way, the privacy and integrity of individuals was guaranteed. The ethics committee of the institution has approved this study.
Results
Of a total of 17 patients studied with NMTD, 10 (58.82%) presented the transverse dimension of the maxillary arch decreased and 7 (41.18%) normal or increased, reason why both groups (A and B) were constituted without significant differences in terms of the number of individuals (p = 0.629).
Table 1 shows the behavior of the cephalometric variables concerning the cranio-mandibular relationship between groups A and B. In both groups, the average value of the position of the ramus was within established values as a norm, however, in A it was close to the lower limit and in B it was close to the upper limit. Regarding the value of the articular angle, the mean of group A was found above the upper limit of the norm. In the (S-Ar) / (Ar-Go) relationship, group B presented, on average, a greater vertical development of the ramus in relation to the length of the posterior cranial base.
Table 1 Craniomandibular relationship. Cephalometric comparison between the study groups
|
|
|||||
|---|---|---|---|---|---|
| Position of ramus (º) | A | 76 ± 3 | 73,64 ± 5 | 68,4 - 83,1 | 0,043 |
| B | 78,6 ± 3,5 | 72,4 - 83 | |||
| Articular angle (º) | A | 143 ± 6 | 150,31 ± 7,6 | 135,2 - 161,8 | 0,043 |
| B | 145,43 ± 2,6 | 142,5 - 149,4 | |||
| (S-Ar) / (Ar-Go) | A | 0,75 | 0,73 ± 0,12 | 0,6 - 1,0 | 0,033 |
| B | 0,62 ± 0,49 | 0,52 - 0,66 |
Table 2 describes the behavior between both groups of the cephalometric measurements related to the mandibular anatomy. It was observed that on average, the height of the ramus, the length of the mandibular body and the mandible, were higher in group B.
Table 2 Mandibular anatomy. Cephalometric comparison between the study groups
| |
|||||
|---|---|---|---|---|---|
| Ramus height (mm) | A | M: 52,0 ± 4,2 F: 46,8 ± 2,5 | 43,89 ± 4,1 | 39,6 - 52,2 | 0,033 |
| B | 50,44 ± 6,1 | 42,6 - 57,2 | |||
| Body lenght (R) (mm) | A | 77 ± 2,7 | 70,8 ± 6,7 | 64,5 - 85,8 | 0,010 |
| B | 80,17 ± 5,9 | 72,6 - 88,8 | |||
| Manibular lenght (mm) | A | - | 116,97 ± 8,5 | 107,4 - 136,3 | 0,025 |
| B | 129,33 ± 9,5 | 113,6 - 140,1 |
Table 3 allows us to compare the cephalometric differences in relation to the maxillo-mandibular relationship between both groups. Group B showed a greater tendency towards a class III skeletal pattern.
The mean values of convexity in the Ricketts, Burstone and soft profile cephalogram were below the norm in group B and were considerably lower in relation to those of group A, which, on the other hand, was more prone to Skeletal class II.
Group B presented a mean Wits measurement lower than that of group A and the established norm. Regarding the result of the difference between the mandibular and maxillary length, the average of group B exceeded that of group A and the norm.
Table 3 Maxillomandibular relationship. Cephalometric comparison between the study groups
| |
|||||
|---|---|---|---|---|---|
| Ricketts Convexity, (mm) | A | 0,5 ± 2 | 2,81 ± 4,8 | -5,4 - 8,8 | 0,033 |
| B | -2,7 ± 2,8 | -7,9 - (-3) | |||
| Burstone Convexity, (mm) | A | M: 3,9 ± 6,4 F: 2,6 ± 5,1 | 5,27 ± 9,4 | -10,5 - 16,4 | 0,033 |
| B | -5,39 ± 5,4 | -14,3 - (-5) | |||
| Wits (mm) | A | -1,2 ± 2 | -1,43 ± 4,5 | -8,7 - 5,5 | 0,014 |
| B | -9,8 ±6,3 | -19,3 - (-2,3) | |||
| Mand-Max Dif (mm) | A | 20-33 | 30,95 ± 6 | 22,9 - 43,9 | 0,003 |
| B | 43,3 ±7,6 | 33,5 - 57,3 | |||
| Soft profile convexity (º) | A | 12 ± 4 | 15,73 ± 9,1 | 2,8 - 28,9 | 0,043 |
| B | 4,67 ± 6,8 | -6,1 - 11,4 |
The significant difference between group A and B with regards to dental overjet is evident in Table 4. It was given by mean values higher than the norm in the first group and lower in the second. In group A, the minimum and maximum values of the dental overjet were higher than in group B.
Discussion
The literature states that NMTDs occur mainly due to a defect in the maxillary arch and to a lesser extent due to an excess of the mandibular arch.(2, 3) However, there are no studies that quantify the proportion between them. In the current research, it was observed that, although there was a higher frequency of patients with upper transverse deficiency (group A), no significant differences were found with respect to those with a normal or widened maxillary arch (group B).
This situation could be the result of the combination of several factors. The medical records of adult patients requiring orthognathic surgery were studied. The chief complaint could be influenced by other dento-skeletal problems with greater aesthetic involvement than the NMTD itself. On the other hand, many simple transverse deficiencies of maxillary origin are solved by orthodontists at an early age by orthopedic means, which is why their frequency decreases in adults.
Now, from the anteroposterior point of view, the cranio-mandibular relationship is important in the assessment of facial skeletal patterns. Class II can be caused or aggravated by a posterior insertion of the mandibular ramus and class III by a more advanced position. The anatomy of the cranial base can be decisive in this regard. In a meta-analysis carried out by Gong et al.11 it is suggested that the angle of the skull base and the lengths of the anterior and total cranial base are significantly lower in patients with class III skeletal patterns and greater in class II subjects.
The current study did not find significant differences in the measurements regarding the cranial base structure between both groups, but in the position of the ramus. On average, it was located more distally in group A. Statistical differences were also observed in relation to the value of the Articular angle, the mean value of which was higher in patients with a narrow maxillary arch.
In proportion to the posterior cranial base, the length of the ramus was significantly shorter in group A (S-Ar / Ar-Go). The ramus height variable (Ar-Go) was also significantly lower. These results are consistent with the variables previously described. The poor vertical development of the ramus forces the mandible, held by its joints, to rotate in a clockwise direction, which increases the value of the articular angle. In turn, the more the mandible rotates clockwise, the more posterior its centroid is placed, the ramus adopts a more vertical posterior position, and the smaller the anterior projection of the pogonion.10
Following the same criteria, Hasebe et al.12 state that the height of the condyle differs considerably between subjects with different anteroposterior and vertical skeletal patterns. Retrognathic and hyperdivergent patients have shorter condyles compared to patients with class I, class III skeletal patterns and normal or decreased facial divergence. Furthermore, Kajii et al.13 agree that patients with idiopathic condylar resorption of the temporomandibular joint present shorter mandibular ramus and greater clockwise rotation of the ramus.
Wang et al.14 in a tomographic study of dry Caucasian skulls, report that there is a significant negative correlation between the value of the angle of the mandibular plane and the height of the ramus. In the present study, there was no significant difference regarding the angle of the mandibular plane between both groups, despite the difference observed in the distribution of the articular angle values.
Other aspects of significant dimorphism found were the length of the mandibular body, according to the Ricketts cephalogram, and the mandibular length, according to McNamara. On average, their values were lower in group A. Furthermore, the mean body length was below the cephalometric norm in group A and above in group B.
All the above mentioned led to the fact that, on average, group B patients displayed lower mean values of skeletal convexity and cutaneous profile. Awad et al.15 advocate that there is a strong significant difference in the length of the mandible (Co-Gn) and the anteroposterior skeletal pattern. The lower values are cluster around skeletal class II, they increase in class I and are higher in class III. Farheen et al.16 report that the width of the maxillary arch in class III individuals is increased and the cause may be attributable to a compensation of mandibular growth to camouflage the true transverse skeletal discrepancy.
The difference between maxillary and mandibular length was statistically greater in group B, which confirms that, in general, the mandibular dimensions of the group are greater in relation to the maxillae. As in convexity, the lower values of the Wits measurements and the dental overjet are the logical result of finding dimensionally larger jaws in this group, with more advanced positions and less clockwise rotation.
In the studied patients, there is the same probability of having the maxillary arch with adequate transverse dimension, wide, or narrow. There are significant cephalometric differences between the two types in terms of mandibular anatomy and cranio-mandibular, maxillo-mandibular and occlusal relationships. Mandibles with increased body length, class III skeletal pattern and concave profile are more likely to be found in patients with wide upper arches, whereas in those with decreased transverse dimensions, the tendency is to present small mandibles with increased articular angle and tooth overjet.

