










 Servicios personalizados
Servicios personalizados Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Malaria is a disease that is closely related to the poverty level of a community and decreases economic growth.1,2 Population from rural areas in Colombia have worrying health indicator levels, and low coverage of basic sanitation services.3,4 This problem is mainly attributed to the geography, great distances to urban areas and complex topography, all of which obstruct access to certain areas and cause an extremely scarce presence of health care service providers.5 These socioeconomic factors, along with human activities as migration and wars, play an important role in malaria transmission, leading to the spread of both parasites and vectors.6
Malaria control and prevention programmes sometimes are designed without the participation of the communities and ignore local knowledge and cultural dynamics regarding their main health issues, which can lead to the enforcement of decontextualized control measures that diminish the coverage and impact of such interventions.7 Some of the control measures used to avoid mosquito bites are the elimination of water deposits, sleeping under insecticide-treated bed nets, using repellent, and wearing protective clothes.8
Communities build knowledge about health and disease that are reflected in their own attitudes and actions and that can contribute to the success or failure of a programme. Community participation in health programmes requires measurable behaviour changes so that individuals can actively participate in the decision-making processes. This cultural construction on the disease-health process in relation to malaria is reflected in its own interpretations, in behaviours and expectations that are specific to each population and that explain its interrelationship with the health system and with the community and self-care. Therefore, when developing institutional programmes, it is necessary to include the community’s perspective.9
Although the incidence of this disease in the municipality of Vista Hermosa, in the Meta department, is not as high as in other departments of Colombia, the number of reported cases has remained constant over time.10) Also, Anopheles darlingi is the main vector of malaria in this region, and it´s anthropophilic behavior causes constant infection rates.11 In addition, as of 2019, four municipalities belonging to this department were on alert because of the increasing number of malaria cases, making it an event of interest for public health.12 The importance to study malaria in Meta department is because of its geopolitical location, and social and political formation because Vista Hermosa have been decisive in the Colombian conflict. At the end of 2016, a small village, was installed there as the starting axis of the implementation of the peace agreements.13) The purpose of this study was to determine the knowledge, attitude and practice regarding malaria in Piñalito, a town located in the municipality of Vista Hermosa in the Meta department (Colombia), during 2016-2017.
Methods
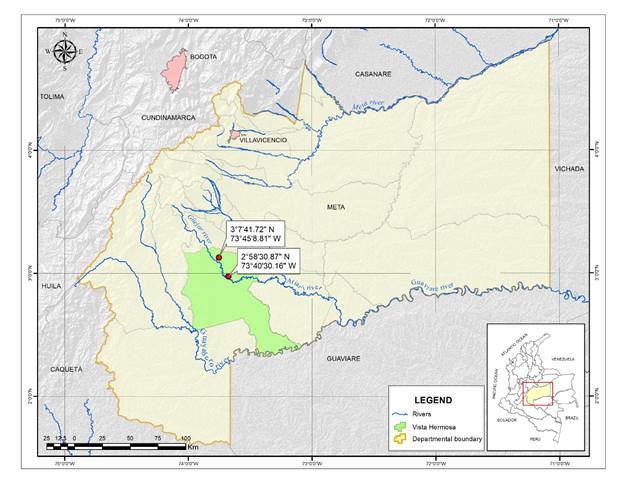
A mixed-methods study was carried out between 2016-2017 in Piñalito, located at 2° 58’ 30.87’’ N and 73° 40’ 30.16’’ W and, 20 km away from Vista Hermosa (Meta) (3° 7’41. 42’’ N and 73° 45’ 8. 81’’ W). Its population is close to 1400 inhabitants14 (Fig.).
For this purpose, a semi-structured survey, validated to address malaria in indigenous communities13, of knowledge, attitudes and practices (KAP) was conducted. It focuses on the determinants of health in settings of developing countries with rural areas. Questions within the variables of basic data, general data and KAP regarding the disease and insight into health care systems were considered. The community was asked a total of 45 questions.
We used a convenience sampling to administer the survey. Because the town has been affected by violence for many years, it is not easy to speak with people, as they have fears for their safety. We established the areas to be surveyed, and if the family didn´t want to participate, the interviewer continued to the next house until the required sample size was reached. Finally, inclusion criteria consisted of being of legal age (18 years old), living in the town for at least 2 years and providing signed informed consent.
The sample size was calculated with a 95% confidence level, a percentage error of 5% and an expected proportion of 0.05 for malaria based on the data reported for Vista Hermosa in 2013. Using these parameters, we estimated a sample size of 73 surveys.
Z = |
the confidence level |
p= |
the probability of success or expected proportion |
e = |
the margin of error |
In addition, semi-structured interviews were conducted based on two questionnaires, one for the community and another for employees of town hall working on health care development programmes and health personnel from the hospital of Vista Hermosa. In total, nine interviews were conducted with three health care personnel at the hospital and the town hall facilities, and six residents of Piñalito. Interviews lasted for 10 to 15 minutes and there was no relationship between the interviewer and respondents. People were allowed to express themselves freely.15 All interviews were recorded and, at the end of each session, the individuals could ask for additional information about the disease.
For data analysis, the variables included in KAP surveys were first described with frequencies and central tendency measures, according to the nature of each variable. For cross tables, nonparametric statistics based on the χ2 and Kruskal-Wallis tests was used. Epi Info 7.0 and SPSS v. 23.0 were used for the analysis.
In addition, we carried out a bivariate analysis focused on social determinants of health. Sociodemographic variables were considered as analysis factors (risk/protective factors) and whether the respondent had malaria in their lifetime was considered an effect. Data were analysed in 2 x 2 contingency tables, and the odds ratio (OR) was calculated from the social determinants seeking to determine the variables that were most likely to be associated with having had the disease. A p value of < 0.05 was considered to be significant according to the χ2 tests and values other than one according to the 95% confidence interval.
Interview findings were analysed by thematic coding based on predefined codes. We used Atlas.ti v. 8.0 to perform the coding. Three groups of codes were created: prevention and control, clinical management and social determinants.
Among the ethical considerations, this study had the approval of the Bioethics Subcommittee of the Universidad Cooperativa de Colombia. We consider the willingness of individuals to participate in the survey and provide informed consent.
Results
KAP surveys
The number of people estimated to participate in this study was 73, but only 46 agreed to complete the survey. This was because the number of inhabitants in Piñalito were less than the expected; and because of the political, social and security conditions, some people refused to participate. The average respondent age was 42.55 years, and the average time that the respondents had been living in the municipality was 21.93 years. A total of 84.78% of this population depended on the government to receive health attention; 6.5% reported not having access to any health system (Table 1).
Survey questions regarding living conditions and basic needs revealed that the population lived in houses with zinc or sheet roofs (82.61%), wooden walls (36.96%) and a cement floor (63.04%). In addition, more than 80% of the respondents stated that they had basic electricity services, garbage disposal, and running water; and 78.26% had a sewage system (Table 1). None of these factors appeared to be risk factors for malaria in Piñalito (p > 0.05; Table 2).
Table 1 - Demographic characteristics about malaria among participants in Piñalito, Vista Hermosa
| Sex | |||
| Female | 27 | 58.69 | 44.33-74.3 |
| Male | 19 | 41.3 | 25.7-55.67 |
| Marital status | |||
| Domestic partnership | 22 | 47.83 | 32.89-63.05 |
| Single | 14 | 30.43 | 17.74-45.75 |
| Married | 7 | 15.22 | 6.34-28.87 |
| Widower | 3 | 6.52 | 1.37-17.9 |
| Health affiliation | |||
| Subsidised | 39 | 84.78 | 71.13-93.66 |
| Contributory | 3 | 6.52 | 01.37-17.9 |
| None | 3 | 6.52 | 01.37-17.9 |
| Special | 1 | 2.17 | 0.06-11.53 |
| Education level | |||
| Primary | 25 | 54.35 | 39.01-69.1 |
| Secondary | 15 | 32.61 | 19.53-48.02 |
| Illiterate | 3 | 6.52 | 01.37-17.9 |
| Technical | 2 | 4.35 | 0.53-14.84 |
| University | 1 | 2.17 | 0.06-11.53 |
| Home Living Condition | |||
| Roof type | |||
| Zinc or laminate | 38 | 82.61 | 68.58-92.18 |
| Cement | 4 | 8.7 | 2.42-20.79 |
| Vegetation or plants | 2 | 4.35 | 0.53-14.84 |
| Clay tile | 2 | 4.35 | 0.53-14.84 |
| Wall type | |||
| Wood | 17 | 36.96 | 23.21-52.45 |
| Spackled or painted | 14 | 30.43 | 17.74-45.75 |
| Only cement | 14 | 30.43 | 17.74-45.75 |
| Other | 1 | 2.17 | 0.06-11.53 |
| Floor type | |||
| Cement | 29 | 63.04 | 47.55-76.79 |
| Soil | 10 | 21.74 | 10.95-36.36 |
| Tile | 7 | 15.22 | 6.34-28.87 |
| Electricity | 41 | 89.13 | 76.43-96.38 |
| Running water | 40 | 86.96 | 73.74-95.06 |
| Garbage disposal | 39 | 84.78 | 71.13-93.66 |
| Sewage system | 36 | 78.26 | 63.64-89.05 |
| Septic tank | 4 | 8.7 | 2.42-20.79 |
| Water well | 3 | 6.52 | 1.37-17.9 |
| River/ravine | 2 | 4.35 | 0.53-14.84 |
Table 2 - Factors associated with malaria in Piñalito, Vista Hermosa
|
|
|||||
|---|---|---|---|---|---|
| Social class | Sex | 1 | 0.3-3.32 | 0 | 0.49 |
| Health affiliation: subsidized | 2.8 | 0.27-29.84 | 0.8 | 0.21 | |
| Education level: illiterate | 0.63 | 0.05-7.5 | 0.13 | 0.38 | |
| Environmental circumstances | Running water | 0.61 | 0.1-3.72 | 0.28 | 0.31 |
| Sewage system | 0.83 | 0.2-3.47 | 0.06 | 0.41 | |
| Garbage disposal | 0.97 | 0.19-4.93 | 0.0013 | 0.49 | |
| Septic tank | 0.75 | 0.096-5.84 | 0.07 | 0.4 | |
| Electricity | 2.11 | 0.31-14.07 | 0.62 | 0.24 | |
| River/ravine | 0.76 | 0.04-12.94 | 0.03 | 0.43 | |
| Marital status: single/widower | 2.7 | 0.79-9.3 | 2.5 | 0.06 | |
| Behaviors and Biological factors | Agrees with fumigation at home for vector control | 1.2 | 0.07-21.86 | 0.03 | 0.44 |
| Filling the trenches with earth | 1.03 | 0.2-5.23 | 0.0013 | 0.49 | |
| Organising cleaning days with the community | 0.95 | 0.21-4.12 | 0.0043 | 0.47 | |
| Draining stains | 1.23 | 0.35-4.3 | 0.11 | 0.37 | |
| Drilling objects that may contain water | 1.17 | 0.18-7.79 | 0.03 | 0.44 | |
| Using mosquito nets | 0.33 | 0.08-1.44 | 2.25 | 0.08 | |
| Using repellents | 0.47 | 0.07-3.13 | 0.6 | 0.24 | |
| Personal protection (clothing impregnated) * | 7.0 | 0.78-62.52 | 3.78 | 0.03 | |
| Fumigation | 2.48 | 0.23-25.81 | 0.61 | 0.25 | |
| Does nothing | 1.31 | 0.07-22.41 | 0.03 | 0.43 | |
| Health System | How do we get malaria: incorrect answers | 0.76 | 0.04-12.94 | 0.036 | 0.43 |
| Do you take all the formulated medicine | 1.92 | 0.37-9.75 | 0.62 | 0.23 | |
| Receives good health care in the medical consultation | 2.25 | 0.57-8.93 | 1.36 | 0.13 | |
| The health secretary carries out community work against malaria* | 8.31 | 0.92-74.89 | 4.5 | 0.02 | |
| The health secretary carries out education days against malaria | 1.2 | 0.3-5.27 | 0.1 | 0.38 | |
| Which health service do you go to when you get sick | 0.7 | 0.06-8.44 | 0.08 | 0.41 |
*Significative risk factors (p < 0,05).
Knowledge
Overall, 43.5% of individuals reported having had malaria at some point in their lives, and 89% still considered this disease to be a problem for themselves and their families. With regard to their knowledge about the disease, 63% of respondents knew that a mosquito is the vector of malaria, although they could not specifically identify the type of mosquito. In terms of their knowledge about the symptoms of malaria: high fever, headache, chills, muscle and bone pain, were the most frequent symptoms reported by the participants. Regarding the question about how malaria is cured, the answer with the highest percentage was take the treatment formulated by the doctor, followed by the consumption of other medicines and then the use traditional medicine. Significant differences were found between the responses (p < 0.05). When asked what test was performed to diagnose malaria, only 32.6% of people could remember a blood test as a diagnostic test and 6.5% answered that the test that had been carried out was called a ‘thick drop’ (Table 3).
Table 3 - Knowledge about malaria, among participants in Piñalito, Vista Hermosa
| Variable | |||
|---|---|---|---|
| Have you had malaria | |||
| No | 26 | 56.52 | 41.11-71.07 |
| Yes | 20 | 43.48 | 28.93-58.89 |
| Malaria is a health problem for you | |||
| Yes | 41 | 89.13 | 76.43-96.38 |
| No | 4 | 8.7 | 2.42-20.79 |
| Doesn´t know | 1 | 2.17 | 0.06-11.53 |
| How do we get malaria | |||
| Bite of any mosquito | 29 | 63.04 | 47.55-76.79 |
| Water | 6 | 13.04 | 4.94-26.26 |
| Other | 5 | 10.87 | 3.62-23.57 |
| Doesn’t know | 3 | 6.52 | 1.37-17.9 |
| Bite of |
2 | 4.35 | 0.53-14.84 |
| Air | 1 | 2.17 | 0.06-11.53 |
| What are the symptoms of malaria | |||
| High fever | 36 | 78.26 | 63.64-89.05 |
| Headache | 28 | 60.87 | 45.37-74.91 |
| Chill | 28 | 60.87 | 45.37-74.91 |
| Muscle and bone pain | 24 | 52.17 | 36.95-67.11 |
| Vomiting and diarrhea | 23 | 50 | 34.9-65.1 |
| Weakness and tiredness | 20 | 43.48 | 28.93-58.89 |
| Doesn’t know | 2 | 4.35 | 0.53-14.84 |
| Other | 2 | 4.35 | 0.53-14.84 |
| How malaria is cured | |||
| Taking the treatment formulated by the doctor | 16 | 34.78 | 21.35-50.25 |
| Taking other medicine | 13 | 28.26 | 15.99-43.46 |
| Traditional medicine | 9 | 19.57 | 9.36-33.91 |
| Other | 5 | 10.87 | 3.62-23.57 |
| Going to the health center | 3 | 6.52 | 1.37-17.9 |
| How many known people have died from malaria | |||
| 0 | 35 | 89.74 | 75.78-97.13 |
| 10 | 3 | 7.69 | 1.62-20.87 |
| 50 | 1 | 2.56 | 0.06-13.48 |
| What test to diagnose malaria has been done | |||
| None | 27 | 58.7 | 43.23-73 |
| Blood sample | 15 | 32.61 | 19.53-48.02 |
| Thick blood | 3 | 6.52 | 1.37-17.9 |
| Doesn’t know the name | 1 | 2.17 | 0.06-11.53 |
Attitudes and practices
To avoid contracting malaria, respondents said that the population of Piñalito takes care of itself mostly using mosquito nets (74%) or by draining water tanks (32.6%). In the same way, survey respondents mentioned having organised cleaning sessions within their community (19.6%) and maintaining personal protection (17.4%). Not using personal protection such as impregnated clothing appeared to be a risk factor for malaria (OR = 7; p = 0.03), but because of the sample size, the 95% CI showed no significant difference (0.78-62.52; Table 2). Most of the respondents agreed with the application of insecticides in the home to prevent malaria and other vector-borne diseases (84.78%; Table 4).
Table 4 - Attitudes and practices about malaria, among participants in Piñalito, Vista Hermosa
| How do you take care not to get sick from malaria | |||
| Using mosquito nets | 34 | 73.91 | 58.87-85.73 |
| Draining stains | 15 | 32.61 | 19.53-48.02 |
| Organizing cleaning days with the community | 9 | 19.57 | 9.36-33.91 |
| Personal protection (clothing impregnated) | 8 | 17.39 | 7.82-31.42 |
| Filling the trenches with earth | 7 | 15.22 | 6.34-28.87 |
| Using repellents | 5 | 10.87 | 3.62-23.57 |
| Drilling objects that may contain water | 5 | 10.87 | 3.62-23.57 |
| Fumigation | 4 | 8.7 | 2.42-20.79 |
| Does nothing | 2 | 4.35 | 0.53-14.84 |
| Using wire mesh on windows | 1 | 2.17 | 0.06-11.53 |
| Do you take all the formulated medicine | |||
| Yes | 41 | 93.18 | 81.34-98.57 |
| No | 2 | 4.55 | 0.56-15.47 |
| Doesn’t know | 1 | 2.27 | 0.06-12.02 |
| Agrees with fumigation at home for vector control | |||
| Yes | 39 | 84.78 | 71.13-93.66 |
| No | 7 | 15.22 | 6.34-28.87 |
| If you have had malaria, some health personnel have visited you | |||
| No | 25 | 54.35 | 39.01-69.1 |
| Have never had malaria | 17 | 36.96 | 23.21-52.45 |
| Yes | 2 | 4.35 | 0.53-14.84 |
| Doesn’t know | 2 | 4.35 | 0.53-14.84 |
| Know someone who cures malaria and is not a doctor | |||
| No | 32 | 69.57 | 54.25-82.26 |
| Yes | 12 | 26.09 | 14.27-41.13 |
| Doesn’t know | 2 | 4.35 | 0.53-14.84 |
| Perception of the health service | |||
| Receives good health care in the medical consultation | |||
| No | 30 | 65.22 | 49.75-78.65 |
| Yes | 13 | 28.26 | 15.99-43.46 |
| Doesn’t know | 3 | 6.52 | 1.37-17.9 |
| The health secretary carries out community work against malaria | |||
| No | 35 | 76.09 | 61.23-87.41 |
| Yes | 8 | 17.39 | 7.82-31.42 |
| Doesn’t know | 3 | 6.52 | 1.37-17.9 |
| The health secretary carries out education days against malaria | |||
| No | 35 | 76.09 | 61.23-87.41 |
| Yes | 10 | 21.74 | 10.95-36.36 |
| Doesn’t know | 1 | 2.17 | 0.06-11.53 |
| Which health service do you go to when you get sick | |||
| Hospital | 19 | 41.3 | 27.00-56.77 |
| Health center | 17 | 36.96 | 23.21-52.45 |
| Other | 6 | 13.04 | 4.94-26.26 |
| None | 3 | 6.52 | 1.37-17.9 |
| Traditional doctor | 1 | 2.17 | 0.06-11.53 |
Members of the population believed that malaria prevention should primarily be the responsibility of each individual (54.3%); and 21.7% believed that it is exclusively the responsibility of the health secretary. Furthermore, 6.5% and 8.7% individuals believed that malaria prevention was the responsibility of the community or family, respectively. These percentages showed significant statistical differences (p < 0.05).
With regard to the perception of health services, 65.13% of individuals surveyed believed that the quality is poor and that they do not feel well cared for. As can be seen in Table 4, 6.09% of respondents also considered malaria control to be the responsibility of the Ministry of Health and that the education they received about malaria from them was poor. When they felt sick, more than 70% of respondents reported attending public health services, and 1.17% of the respondents said they prefer traditional medicine.
Semistructured interviews
Six residents who met inclusion criteria agreed to participate in interviews. Knowledge and perception of the problems associated with malaria among the residents of Piñalito varied among the study participants. Some residents confused malaria with infections caused by arboviruses that have caused major outbreaks in recent years.
Years ago, malaria was traditionally identified with the mosquito, and over the years, there is still the same kind of mosquito, but some other similar diseases have developed... right now, the term malaria is no longer used because there are other terms such as chikungunya and dengue, but they are ultimately the consequence of the bite of the same insect. (Inhabitant of Piñalito 01)
People who had malaria in the past, had more knowledge about its mechanisms of transmission, symptoms, treatment and prevention; but there was no consensus on the treatments.
... the most severe symptoms (for malaria) were fever, chills, malaise, and sweating, and people learned to recognize these symptoms. (Inhabitant of Piñalito 03)
A reduction in the number of malaria cases within the area has led to a decrease in the perception of risk by the population. The reasons for this reduction remain unclear; however, after the peace agreements and the designation of Local Transition Zones for Normalization in Vista Hermosa, malaria began to be reported more frequently. Another element is the deforestation that approaches the habitat of the mosquito to people. However, these assumptions are still under study.
This was a wooded area, there were a lot of mosquitoes and other insects, and with the malaria vector control program, today we are in a slightly better state of health. It still exists, but not in such quantity. (Inhabitant of Piñalito 06)
The health service in Piñalito is poor; despite having facilities, the service does not have permanent staff. Occasionally there is a nurse, but most of the time, villagers must go to Vista Hermosa for medical care. Inhabitants generally feel unprotected and vulnerable. Malaria prevention campaigns have not been carried out recently.
Sometimes you can get health care, but sometimes not... here there is no stability, … in case of serious illness, you need to rent a car… (Inhabitant of Piñalito 05)
There is a nurse, but she is almost the whole time in Vista Hermosa; here there is no nurse, no doctor or anything, here we are abandoned... here there are people who have died on the road because they couldn't receive health care here. (Inhabitant of Piñalito 04)
Here, in Piñalito, there is no prevention or health care. The nurse is part-time, nothing more... and she can't handle everything because she has to go to the rural area. (Inhabitant of Piñalito 03)
The government and health authorities are aware of the deficiencies of the health system in this area, due to the lack of personnel and the precarious access roads. It is the result of a process of centralization of health services. This makes people miss their medical appointments or prefer not to attend due to lack of money.
The operating capacity of the hospital may not cover all services; Occasionally we have only two doctors... the municipality has a fairly large territory, and a lot of people in the community do not come to the hospital because the roads are not in good conditions, and it is difficult to travel them. (Health/public health worker 02)
Health care in the rural area is limited; people must go first to Vista Hermosa; then, they must ask for an appointment, and there are always a lot of patients. (Health/public health worker 01)
Despite the government's efforts, these are still ineffective and do not always consider the opinion of the communities.
We work together, and we have developed joint actions that have allowed us to carry out educational actions and ensure diagnosis... we always have the help of technicians who support us in the interventions we carry out. (Health/public health worker 03)
There is a collective intervention plan within the 2018 health action plan, with activities for urban and rural areas, focused on vector control. This strategy is not oriented toward fumigation but toward community work in each home. (Health/public health worker 02)
There is a progressive deterioration of health promotion and disease prevention activities, and a low impact of the integrated vector control strategy.
Discussion
The increase of malaria cases in Vista Hermosa could be forced relocation, that allows the disease to migrate to other regions without malaria.16,17 Piñalito has been affected by violence, and most of its population have been victims of armed conflict and forced to relocate. Other problems such as unemployment, deterioration of the roads, an absent state and lack of public policies that meet the needs of the population became evident. According to the Education Ministry, the education coverage of Vista Hermosa in 2018, to which Piñalito belongs, is 62.63%; this is below the national education coverage percentage (84.88%). This increases inequality in the population.18) All these problems, are part of social determinants that could help to increase health problems.
A report published in 201619 emphasised the problems with the aqueduct and sewage systems in Piñalito, which lack total coverage and require maintenance. Three years later, the situation has not improved, putting the community at risk of contracting diseases. The municipality of Vista Hermosa generally experiences these problems because of a deficit in the coverage of basic sanitation services provided by the municipality, which was detected in 2009.17 In the urban area of the municipality, the aqueduct provided service to 86.5% of the population, sewage system services were provided to 62.8% and sanitation services were provided to 85% of the population. These data are similar to those found in this study on Piñalito, where the aqueduct reaches 85% of the population, the sewage system reaches 78% and sanitation reaches 85% of the population. These data provide evidence that the population considerably lags behind other populations.
Older people have a better knowledge of malaria, its mechanism of transmission and its symptoms, primarily because most of them have had this disease at least once. Because of recent outbreaks of dengue, chikungunya and Zika infection, many individuals were unable to distinguish malaria from these infections caused by arboviruses, which are transmitted by a different mosquito species. Currently, these populations have been more in contact with arboviruses than with malaria; therefore, they associated any disease transmitted by mosquitoes to those caused by arboviruses, such as dengue; the same had already been identified in Vista Hermosa in 2016.20
The sociodemographic characteristics showed that in terms of house structure, zinc roofs followed by wood walls were the most prevalent materials used in houses. Similar results were observed in Quibdo (Colombia)21 and Chiapas (México),22 which showed some environmental characteristics similar to other endemic areas.
Field observations showed that the use of mosquito nets was the most important control measure in this community, which was also reported by Fernández et al. (2014)7 and de Oliveira et al. (2019),23 and in the northern coast of Ecuador by Sáenz et al. (2017),24 in Iquitos (Perú) by Newell et al. (2018)25 and Chiapas (México) by Mora-Ruiz et al. (2014).22 The application of insecticides for vector control was widely accepted among the surveyed inhabitants (84.78%); a similar result was found in other studies, in which individuals accepted insecticide application for malaria vector control, despite their disgust regarding the smell.26,27
About the behaviours and biological factors (Table 2), the use of personal protection elements to avoid getting sick with malaria, was statistically significant (p ( 0.05), a result that coincides with what was found in the Romay-Barja study in New Guinea, in which the participants of this study answered that among the prevention or personal care measures, mosquito nets were the best preventive measure (OR = 0.43; p = 0.001). However, for the prevention strategy to remain fully clothed the association was not statistically significant (OR = 3.54; p = 0.054).28
The municipality, along with the Departmental Health secretary, conducts intersectoral health actions with the community on a monthly basis and has established the community epidemiological surveillance committee in the neighbourhoods of Vista Hermosa where the community receives guidance and empowerment about events of public health, including vector-borne diseases. According to information recorded in the municipality of Vista Hermosa in 2011,29 Piñalito had a level 1 health care centre, with two beds, some emergency care equipment and staff including a nursing assistant who provides basic care and conducts promotional and preventive programmes. The health facility in the town was found to be almost abandoned, with no equipment or staff in charge. Therefore, to receive medical attention, individuals must travel to Vista Hermosa. However, the access roads are affected by rains, which consequently greatly increases travel times, further limiting access. This is reflected in the results, in relation to the population’s perception about health services and the medical care they receive. Survey respondents reported a distant relationship with little sense of belonging and low identification with the health system; 65% of the individuals surveyed expressed disagreement with the institutional offer of health services.
According to the health personnel of Vista Hermosa, febrile episodes treated in the health centre are not compatible with malaria, because they do not present the triad of fever, sweating and chills. However, toward the rural area, more cases of malaria were detected, which are referred for diagnosis via a thick blood smear. However, doctors report that patients from these areas are lost to follow-up and never return for treatment, because they affirm that they take other medications. The residents of Piñalito reported using mata-ratón (Gliricidia sepium) and Cabo de Hacha tree (Aspidosperma macrocarpon) for fever. However, these treatments are not 100% effective and act on only some symptoms, such as fever, without fully killing the parasite. This behaviour might affect the reporting of malaria cases; this underreporting has an effect on the incidence rate of the disease in the population of this municipality. The use of alternative methods is common in populations with high incidence rates of malaria. In Ghana and Nigeria, people use herbs and other alternative treatments to cure malaria, and there is also a large percentage of the population who opt for self-medication. The reasons for this decision are quite similar to those found in this study, which included economic difficulties and poor health care, making individuals seek alternatives for the treatment of these diseases, increasing morbimortality.30,31,32
Although an improvement has been observed in recent years, waiting times for physician care are still long. The relationship between public health providers and health insurers has deteriorated because of delays in the payment of services provided, which impairs the finances of health care providers and the improvement in the supply and quality of care. This establishes a barrier to accessing health services and represents a risk for vulnerable populations such as Piñalito.
Limitations
This study has some limitations. First, because the number of inhabitants estimated in the last census does not reflect the reality of this population, fewer inhabitants were found than those registered at the census. Second, because of the political and social conditions in the region, some people refused to participate in the survey; therefore, the potential number of respondents was decreased. Only those surveys and interviews in which people were willing to respond clearly and truthfully were considered for the study. This limited sample size could affect the reliability of the study, because of higher variability and likely bias. Furthermore, a type II error was possible, which decreased the power of this study. However, despite these limitations, our results are meaningful for this community and other areas with similar socio-political and economic issues.
Conclusion
Our results provide evidence that the population’s experiences with malaria are strongly influenced by social determinants of health. Dispersed rural population conditions and factors originating from social and political violence, drug trafficking and a low state presence have generated a significant estrangement between community knowledge and promotion and prevention activities carried out by the health system. These factors in turn create greater risk in the transmission of the disease and greater obstacles to its prevention, diagnosis, and treatment. Piñalito is almost abandoned by the government, which presents many shortcomings, especially in health care service. Its community is apathetic and fearful; and this is reflected in the low community participation in vector control programs. In addition, there is a poor perception of health services by its population; supply difficulties; a lack of quality, humanisation, and basic resources; and an absence of community participation. These aspects could compromise disease and vector control programmes, and there is evidence for the need to redesign strategies and emphasise community collaboration.

