










 Servicios personalizados
Servicios personalizados Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkINTRODUCTION
Gouty arthritis (Gout) or “king´ disease” is known since ancient times. It is mentioned in texts of Ancient Egypt, as Ebers papyrus in the year 1500 b.c.(1, 2)
Gouty arthritis (Gout) is a persistent metabolic disease that produces an increase of the circulating uric acid, with the resulting deposit of monosodic urate crystals in the tissues, more frequently in the ones of the musculoskeletal system that can lead to either acute clinical manifestations or acute inflammatory episodes, as well as persistent or chronic clinical manifestations.3-5
The current tendency is to consider it as a disease of genetic, epigenetic and heterogenetic nature which polyvalent substrate rules several types of metabolic mistakes due to the evocation of enzyme deficiencies of familiar transmission but managed by different genes.6,7
The attacks of gout are due to the presence of monosodic urates in the interarticulate spaces that provoke the inflammation of some articulations and the surrounding tissue; this inflammation tends to attack the nervous ending of the articulations and produces a deep pain.6,8,9
The uric acid can increase in the blood due to a growth of its production or to the decrease of its excretion through the urine, however there are people that maintain persistent levels of acid uric in blood (hyperuricemia) for a long time and don´t develop a gout crisis, only a 20 % of them will develop the disease.5,8
There are situations and products that produce a growth of uric acid spontaneously favoring the appearance of crisis: stress situations such as surgical procedures, infections, local traumas; in general the use of radiologic iodine contrasts, certain products of the diet like caffeine, alcohol, shellfish, blue fish, viscera, red flesh, legume, asparagus, mushroom, tomatoes, spinach, cauliflower, broad beans, etc, can increase the levels of uric acid. There also exists some medications such as diuretics, thiazides (clortalidone, hydrochlorothiazide, indapamine, and xipamide), low doses of aspirin and theophylline.1,2,9,10
Gout is associated to diseases like diabetes mellitus, arterial hypertension, hyperlipidemias, obesity and others such as: myeloprolypherative diseases, polycythemia vera, myeloid metaplasia or chronic myeloid leukemia.9,10
Gouty arthritis in the female sex is rare, although it can present with more frequency after menopause. The rate of new cases in women increases with age, after 60 years of age, where the statistics show a percentage approximation to the figures established for the male sex. The relation male/female is 5-8 / 1.3-5,9
The world statistics about gout corroborate that three of every thousand persons are affected by this disease, with a higher incidence in men between the 3rd and 4th decade of life. Also, between a 10 and a 20% of the patients have previous family history of the disease. 5,9,11
There are differences according to ethnic origin, it is more common in people of the Pacific islands and in the Maori population of New Zeeland, but it rarely appears in the Australian aborigine.5,12
In the United States the gout is twice more frequent in Afro-American people than in Caucasians, being the most common type of arthritis among North American men. Updated statistics state that there are approximately 8, 3 millions of sick people in that country.12,13
In Spain it presents with a higher frequency in the male sex of black race, it is associated to obesity, alcohol intake and dietetic habits.5,12,13
Cuban statistics behave similarly to the developed countries, being more frequent this entity in the male sex with an incidence of 4-6 males per every woman that suffers from it and prevailing in black patients.
Epidemiological findings carried out suggest that in the next years new cases will increase, associated to dietetic habits and life styles harmful for health.14
The present study has been designed with the objective of characterizing clinically and epidemiologically patients with a diagnosis of gouty arthritis at Arnaldo Milián Castro University Teaching Hospital of Villa Clara province, Santa Clara, Cuba.
The frequency of the presentation of the disease according to sex, age, skin color, personal pathologic antecedents and toxic habits will be taken into account. Also the starting clinical manifestations and radiologic alterations found will be identified.
METHODS
An observational, descriptive, transversal and of development investigation was carried out at Arnaldo Milián Castro Clinical Surgical University Hospital of Villa Clara, Cuba during the period understood from January 2016 to December 2018.
The population of study was formed by all the patients with a diagnosis of gout arthritis older than 18 years of age that were assisted from January 2008 to December 2017 at the service of Rheumatology of the previously mentioned institution. The sample was selected of unprovable way by criteria and being formed by 72 patients that accomplished the following conditions:
Criteria of inclusion:
. To have a diagnosis of gouty arthritis.
Criteria of exclusion :
. Patients with diagnosis of this disease that were assisted due to other causes not related to the disease.
Techniques and procedures:
The documented analysis served as support of the investigation. Its object was the patient’s clinical chart and the clinical charts of the hospital. Its objective was the gathering of information related to socio-demographic and clinic variables associated to the diagnosis of the patients that formed the sample. All the data were collected in a guide of documented review made by the author. Variables such as age, sex, personal pathologic antecedents, toxic habits, more affected systems, applied treatments and more frequent causes of death were used.
For the statistical process of information, the obtained data were put in a card index, using the electronic tabulator Microsoft Excel 2016, where the data corresponding to the variables of study were put in a data base of SPSS version 19.0 which permitted to make tables and/or graphs; showing distributions of absolute and relative frequencies as well as average among ages and maximum and minimal values. From the inferential point of view Square Chi (X2) was applied to demonstrate significant differences among percent.
Pearson´s correlation coefficient was used as a measure of lineal association to see the relation among variables. Together with the value of Square Chi (X2) test its significance was shown (p).
According to the value p, its difference or association was classified in:
. Very significant: If (p) is ˂ 0.01
. Significant: If 0.01 ˂ (p) ˂0.05
. Not significant: If (p) ≥ 0.05
Bioethical considerations: During the development of the investigation, ethic and legal features were considered in the obtaining of information, according to Helsinki statement and the establishment for commission of international ethics (autonomy, beneficence, not evil talk and justice). The information related to the cases was only used by the authors; also, the results are only for scientific purposes, data that could serve to identify the studied sample were not included.
RESULTS
Table 1 shows the distribution of patients according to age groups and sex, where it was stated that the male sex prevailed with 65 patients, for a 90,3 % and the etharian group of 40 - 49 with 23 patients for a 31,9 %.
When comparing the rate of patients by sex very significant differences were found. When comparing the rate of patients by age group very significant differences were found.

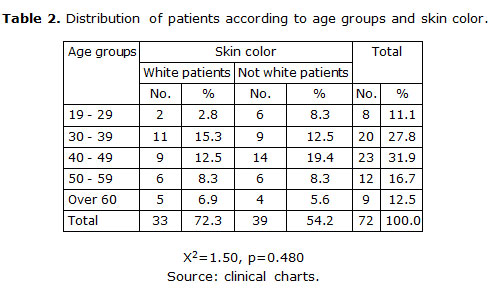
Table 2 represents the distribution of patients according to age groups and skin color, where it is observed the predominance of not white patients with 39 cases for a 54, 2 % and in reference to the etharian groups, the group of 40-49 with 23 patients for a 31.9 %.
There were not significant differences when comparing the rate of patients by skin color.
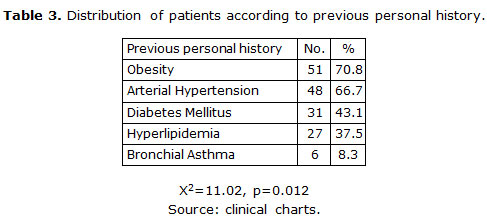
As is shown in table 3, the results of the study appear according to previous personal history, where it was observed that obesity and arterial blood pressure were the most represented with 51 and 48 patients that signified a 70.8 % and a 66.7 % respectively. When comparing the patients´ rate according to previous personal history very significant differences were found.
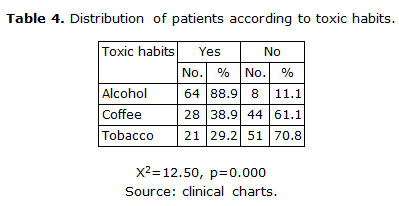
It is demonstrated in table 4 the distribution of patients according to toxic habits where it can be seen a predominance of patients consumers of alcohol with 64 patients for an 88.9 %.
When comparing the ratio of patients according to toxic habits very significant differences were found.
Alcohol X2=43.55, p=0.000
When comparing the ratio of patients by alcohol intake very significant differences were found, it didn’t occur the same in case of coffee and tobacco.
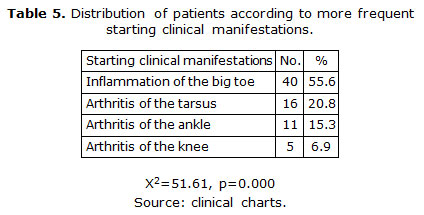
There are shown in table 5 the results obtained in the study according to the more frequent starting clinical manifestations where it is stated that inflammation of the big toe prevailed in 40 patients that represented the 55.6 % of the studied sample.
When comparing the rate of patients by starting clinical manifestations very significant differences were found.
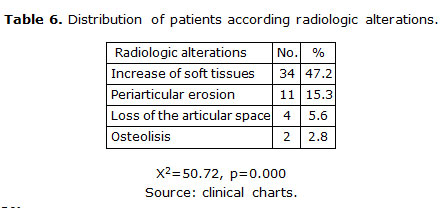
It is confirmed in table 6 the distribution of patients by radiologic alterations found in the studied sample where it can be observed the predominance of the increase of soft tissues in 34 patients for a 47.2 % from the total of the studied sample.
When comparing the ratio of patients according to radiologic alterations very significant differences were found.
DISCUSSION
In table 1, from the results it is shown the distribution of patients according to age groups and sex. It can be seen that the male sex prevailed with 65 patients and the etharian group of 40-49 years of age with 23 patients representing the 90.3 % and the 31.9 % respectively. In the female patients the incidence was less, only 7 patients were found in the study. These results coincide with the statements that appear in the literature, it is stated in consulted articles that it is more frequent in men predominating between the third and fifth decade of life. It is rare prior to adolescence in males and prior to menopause in females. The relation man woman is of 5-8:1.5,15,16
Gout affects mainly the male sex (90-97%) between the third and fifth decade of life, but it can appear at any age, even in puberty.5,9
Martinez JP et al. carried out a study where patients with gout were characterized, in which it could be stated that the sample of study was more representative between the 30 and 50 years of age and in the masculine sex, which coincides with the present study.14
In a study carried out information was obtained about two hospital centers of reference: Municipal Hospital of Badalona and University Hospital Germans Trias Pujol, in both results were obtained similar to the present study concerning the age and sex of the patients.15
A study of gout and comorbidity performed at the University of Alabama in Birmingham (UAB) between January 2016 and February 2017 confirmed a higher incidence of gout in male patients; nevertheless the age rank was more representative in the 6th decade of life.17
Gouty arthritis in the female sex is rare (3-10 %) although it can present with more frequency after menopause, probably because of uricaemia is higher at this time. The ratio of new cases of gout in women is increased with age, after 60 years of age, where statistics show a percentage approximation to established figures for the male sex.3-5,9,11
The authors consider that the high frequency of gout in males can be caused to the fact that they have less capacity to tolerate records of Hyperuricemia, associated to the point that due to sociocultural factors they have more toxic habits, as well as the presence of diseases related to insane diets.
Table 2 of the results shows the distribution of patients by age groups and skin color, where it is observed the majority in not white patients with 39 cases for a 54.2 % and in reference to the etharian groups the one of 40-49 with 23 patients for a 31.9 %.
In the United States the gout is twice more frequent in Afro-American persons than in Caucasians. A report in male medicine students showed the prevalence of gout, followed by a medium of 28 years after graduation, of 5.8 % in whites and 10.9 % in Afro-Americans.12,13
However, another study developed at Alabama University in Birmingham (UAB) between January 2016 and February 2017 demonstrated a higher incidence in white patients than in Afro-Americans although there were not significant differences.17
Sicras-Mainar developed a follow up study in Mexican patients with gout during 2 years, in which it could be identified that the 60 % of the patients were not white, with an average age between 35 and 45 years.18
In investigations done to patients with gout it has been stated that the incidence during 2 years was of 3.2 every 1000 men versus 0.5 every 1000 women, where the 97.5 % were black people. Another report showed the prevalence of gout in a medium of 28 years of age and a predominance in Afro-Americans.2,4,8
In quality of life studies in patients with gout, it is confirmed a worst prognosis in afro-descending patients.12,13
According to the authors´ criteria, the predominance of gout in patients with not white skin color, in the present investigation as well as consulted literature can be related to the current crossing of races in Cuba and the world, associated with genetic, epigenetic and cultural factors.
In table 3, from the results it is revealed the distribution of patients of the study according to previous personal history where it can be observed that obesity predominated in 51 patients, representing the 70.8 % and arterial hypertension with 48 cases for a 66.7 %.
A study carried out by the General Hospital of Vancouver (Canada) and by Harvard Medical School, from Boston (United States) made a follow up of 46000 males, all of them of 40 and more years of age and without medical history of the disease. The men were weighted at the beginning of the study and then every two years and were asked what medication they were taking and which medical condition they had. Throughout twelve years 755 new cases of gout were detected among them, also a direct relation between obesity and the risk of suffering from gout was found.19
Another follow up study for 52 years published by the Faculty of Boston states that obesity is one of the main risk factors of gout. Almost the 71 % of the people with gout have overweight and the 14 % of them are obese.19
The increase of gout in the last two decades (from 45 to 62.3 per 100,000) goes to an growth of obesity from 22.9 % during 1988-94 to 30,5% in 1999-2000. According to the study of the University of Boston people are consuming more flesh, more shellfish and more grease, drinking more beer and doing less exercise, habits that worsen obesity, arterial hypertension and diabetes mellitus, which increase the risk of developing gout.19
Gout has been associated epidemiologically to a higher frequency of hyperglycemia, hyperlipidemia, obesity and hypertension that is known as metabolic syndrome. The decrease of overweight, a diet without excess of protein of animal origin and a right caloric contribution can reduce the uricaemia, not of a limited manner, but with an important impact in the general patient´s health, mainly in the reduction of vascular risk.5,20
According to the study done by investigators of the University of Queensland, Australia, in the last decade the figures of the disease have double, which can be due to longevity, changes in the diet and the increase in cases of hypertension. The majority of cases were associated to cardiovascular diseases, mostly hypertension (39 %), followed by renal disorders (27 %) and diabetes (27). The study revealed that the people who suffered from gout together with another condition like cardiovascular disease had a less probability of survival than the ones who were admitted only because of gout.21
It is shown in table 4 the distribution of patients according to toxic habits, where it can be observed that 64 patients that represented the 88.9 % of the studied sample were alcohol consumers.
The consumption of alcoholic drinking has been associated as a risk factor of high incidence in patients who suffer from gout in relation to literature, representing a predisposing cause for the development of hyperuricemia and gout, and in people who suffer from it alcohol intake is a conditional factor for the appearance of tophi arthritis.22
It is stated in the consulted literature that different mechanisms of the same feeding can lead to hyperuricemia by means of several mechanisms that function of coinciding way, and among them alcoholic drinking has an outstanding place.
Alcohol increases the production of lactic acid and inhibits the renal excretion of uric acid in a competitive way. It also stimulates the synthesis of uric acid which is associated with a re-exchange, growing the nucleotides of adenine in these patients.23
In a multicenter study done in persons belonging to two hospital centers of reference: Municipal Hospital of Baladona and University Hospital Germans Trias Pujol alcohol consumption also had significant statistics in the patients belonging to the sample. In this study it was evidenced that more than the 80 % of the patients with gout were usual customers of alcoholic drinking.15
According to a North American study published in the British Journal of Medicine, the men who consume two or more alcoholic drinking have an 85 % more of probabilities to develop gout than people who drink less than once in a month.19
The authors consider according to their personal experience that alcohol is not only a risk factor of gout, but also an important risk factor for the appearance of new crises and the development of more severe forms of this disease.
Table 5 shows the distribution of patients according to more frequent starting clinical manifestations in patients that constituted the sample of the present study. It can be seen that the inflammation of the big toe predominated with 40 patients for a 55.6 %.
The literature states that the characteristic and more frequent clinical manifestation is pain in the first toe named inflammation of the big toe, but the pain and the inflammation can appear in any joint, mainly of the lower limbs (tarsus, ankles and knees).5 This coincides with the present study where, as described before, the inflammation of the big toe was the more frequent clinical manifestation.
In a multicenter study it was demonstrated that the first bout of gout affects the first metatarsophalangeal articulation (inflammation of the big toe) in the 50-80 % of the cases, that joint is compromised in a certain moment of the evolution of patients with gout. In the starting phases of the disease, the metatarsophalangeal arthritis is usually rude with a maximum of symptomatology in the first 24-48 hours.15
A study of gout and comorbidities affirms that the joint affectedness in patients with gout is such that can lead to irreversible damage.17
According to a North American study published in the British Journal of Medicine, more than the 50% of the patients presented inflammation of the big toe as starting manifestation, which coincides with the present study.19
The study mapping patients’ experiences from initial symptoms to gout diagnosis: a qualitative exploration accounts that the arthritis is the main clinical manifestation of gout, being the arthritis of the first metatarsophalangeal articulation the most frequent.20
It can be seen in table 6 the distribution of patients according to present radiologic alterations in the studied sample where the increase of soft tissue prevailed in 34 people that represent the 47.2 % of the sample.
In the consulted literature there is a reference to this radiologic finding in the majority of patients, which coincides with the results obtained in this study. Other authors state that it is the most common consequence caused by gouty arthritis in the osteomyoarticular system. Images techniques do not contribute to a sensible and specific diagnosis of gout, but can be useful in the validation of severity for a progressive follow up.
Simple radiology does not show findings at initial stages of gout, except an increase of soft tissue that coincide with episodes of acute inflammation. Periarticular erosions and periosteal reaction in “small roof” can be observed in patients initially, and later loss of the articular space that could end in a deformity due to a bad alignment and in very severe cases osteolisis.5,15
Recent studies suggest that the radiologic variations in gout are untied by an inflammatory answer where the nitric oxide, the prostaglandins and the factor of alpha tumor necrosis (TNF) intervene along with the IL-6, pro-inflammatory cytokines such as IL-1, mainly the IL-1, produced by macrophages, dendritic cells and monocytes, as well as the presence of the inflame some complex NLRP3 (intracellular proteolytic complex).6,24
In a study where patients with gout arthritis were categorized at 10 de Octubre Hospital in Havana city, Cuba, evidenced that the 55 % of the patients had an increase of soft tissue, the 10.8 % had periarticular erosions, the 4.5 % and the 0.8 % had decrease of the articular space and osteolisis respectively.14
A 10 years investigation accomplished by investigators of the University of Queensland, Australia, in the last decade, statistics demonstrated that the 50 % of the patients with gout admitted to hospitals in England and New Zeeland had radiologic alterations.25)
Another relevant study carried out at the general hospital of Vancouver, Canada and Harvard Medical School of Boston United States, obtained similar results, as the 53.4 % of the patients presented radiologic alterations. The increase of soft tissue was the most representative.19)
According to the authors´ criteria this could be done due to the severity or extent of the inflammatory process at the articular level or the presence of intra-articular monosodic urate crystals. The progression of the articular damage is related in the majority of patients with the time of evolution of the disease associated with a poor dietary and therapeutic control.

