










 Servicios personalizados
Servicios personalizados Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
A skeletal injury involving fracture of the pelvis or acetabulum and ipsilateral femur is called a floating hip. These injuries are rare and the incidence is about 1 in 10,000 fractures.1,2 Floating hip injury is associated with high energy trauma, such as fall from height and motor vehicle accidents and occurs mostly in the younger population.
Prior to the year 1990, very few published literatures describing this injury was available. The terminology ‘floating hip’ was introduced by Liebergall. He classified the injury into two types: Type A and B. Type A is a posterior type injury: a posterior type acetabular fracture with ipsilateral diaphyseal femur fracture. The Type B is the central type wherein there was a central type acetabular fracture and an ipsilateral proximal femur fracture.1
Another study by Muller et al in 1999 described the fracture pattern, classification and complications associated with this injury. He divided it into 3 types. Type A injuries represent a fracture of the acetabulum and the ipsilateral femur, type B lesions consist of a fracture of the pelvic ring and the ipsilateral femur, while type C lesions involve a fracture of the pelvic ring associated with an ipsilateral fracture of the acetabulum and the femur.2
Till date, there exists a dilemma regarding the sequence of fixation of fracture (whether femur or acetabulum should be fixed first), whether a single or double staged fixation is preferable and how to minimize and manage the vast complications that may arise due to this injury. Single stage surgery is favoured in patients with no other comorbidities, as early fixation and reduction permits early mobilization and improves clinical outcome. The management should be individualized according to the injury pattern and expertise of treating surgeon, as this injury can have a severe impact on the patient’s quality of life.3 Lack of standardized protocol for management of such fractures makes it a surgical challenge.
The major complications associated with floating hip include: hetero-tropic ossification, deep vein thrombosis , traumatic sciatic nerve palsy and avascular necrosis of head of femur. The severe traums leads to extensive soft tissue damage which can affect rehabilitation and quality of life post surgery.4) In this report, we have described the management and complications of one such case (Liebergall type B) which presented to our hospital following a road traffic accident.
The objective of this case report is to highlight the usefulness of single stage surgery using a common incision, the order of fracture fixation, in lateral decubitus position for type B floating hip injuries.
Case report
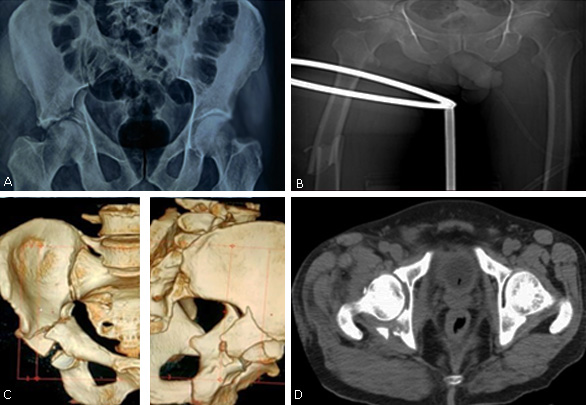
A 58-year-old male, presented to our emergency department with pain, swelling, deformity of right lower limb following a road traffic accident. On primary examination, patient was in hypovolemic shock. The right lower limb was externally rotated, with apparent shortening and gross swelling in the thigh. There were no open wounds over the lower limb. Abnormal mobility was present in the right thigh. Distal neurovascular examination was uneventful. He was evaluated using ATLS protocol and was stabilized hemodynamically with fluid resuscitation including blood transfusion. The right lower limb was temporarily stabilized using fixed skin traction on a Thomas splint. Radiographs revealed fracture of the right posterior column and posterior wall of acetabulum with ipsilateral diaphyseal femur fracture. CT scan revealed trans-tectal transverse fracture with posterior wall fracture. A secondary survey revealed no other injuries (fig 1).
After explaining the nature of the injury and the prognosis, the patient was taken up for surgery after 4 days. We decided to operate in a single stage in lateral decubitus position. The incision site was marked (Kocher Langenbeck approach). After skin marking, we first made the incision along the distal 1/3rd of the marking to expose the entry point for femur nailing. Intramedullary interlocking titanium nail was inserted under guidance of image intensifier. Subsequently the incision was extended proximally to expose the posterior acetabular fracture site. The sciatic nerve was intact. The posterior column and wall fractures were reduced and fixed with two separate contoured titanium reconstruction plates. Separate fixation of anterior column was not done as adequate stability was achieved (figs. 2, 3 y 4).


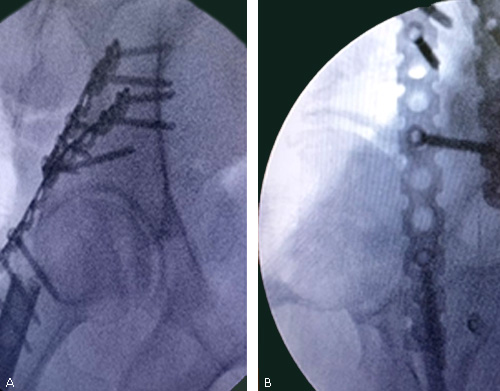
The operative time was about 3 hours. There were no intra-operative complications. Post-operatively, patient was started on chemoprophylaxis for deep vein thrombosis. In bed mobilization started from first post- operative day and non- weight bearing mobilization was started from second week onward. The patient was evaluated with periodic radiographs to check the maintenance of reduction of fractures. At 10 weeks, there were no progressive signs of healing of the diaphyseal femur fracture. Hence teriparatide therapy (20mcg daily subcutaneous injections) was initiated for six months and assisted weight bearing mobilization was started (figs. 5, 6, 7 y 8).




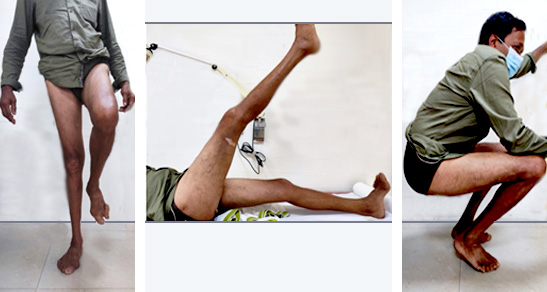
At seventh month, radiographs revealed signs of adequate union in both the fracture sites and patient was able to mobilize independently. There was no evidence of heterotrophic ossification or avascular necrosis of the femoral head in serial follow-up radiographs (fig 4). Nine months post injury, patient was able to return to his pre injury status. He had painless good range of movements in his right hip and was also able to squat and perfrom activities of daily living (fig 9).
Discussion
Before the year 1990, there was no official terminology to address this type of fracture pattern. Liebergall et al were the first to introduce the term floating hip for a fracture pattern that involved the pelvis/acetabulum and ipsilateral femur.1) The management of individual fractures of pelvis and femur have been extensively discussed in literature. Attempts to shed light on the grievous nature of the injury, the initial management and also to associate the complications arising from this injury have been going ever since. Rajashekaran et al5 used the term ‘complex floating hip’ to denote ipsilateral acetabular fracture associated with a displaced femoral head fracture and a femoral shaft fracture.
Avascular necrosis of head of femur (AVN), deep vein thrombosis(DVT), heterotrophic ossification (HO) and neurological deficits (either pre injury or iatrogenic) are the commonly associated complications. HO has been documented in patients with concomitant head injury and the role of indomethacin has also been documented in the prevention of HO. DVT is more common in elderly individuals due to prolonged post-operative immobilization and be prevented by initiating anti coagulation therapy.
The lack of a standardized protocol brings forth the following questions: which fracture must be fixed first, whether it advisable to fix both fractures in a single stage procedure or one after the other and how to avoid complications which may arise. Majority of the authors feel that fixation of femur should be done first as it provides stable platform for manipulation and reconstruction of the joint. Also, the femur shaft fracture can mask the hip dislocation as it acts as corrective osteotomy.1,6,7,8 Depending on the femur fracture(proximal, midshaft, distal), anterograde or retrograde nailing is preferred, followed by acetabulum fixation. The preferred patient positioning(supine, prone or lateral) during surgery is up to the treating surgeon. In cases associated with hip dislocation in floating hip, preference is given to reduction of hip first.9
Kregor suggested prioritising fixing the acetabular fracture first.10) Suzuki and Wu et al11 have documented that in case of Muller Type B, the pelvis has been fixed first as internal injuries that arise due to pelvic ring fracture are grave and should be addressed. However in case of Muller Type A, they prefer the femur first approach. Babak also believed in fixing acetabulum/pelvic injury first.12 Most patients present with associated grievous injuries to head, spine and abdomen which can lead to delay in definitive operative management. This necessitates the need for multiple staged surgeries which can lead to increase in morbidity and delay in recovery. Umesh et al mentioned the average time between injury and the first Orthopaedic surgery in his study series was 4.41 days.13) The decision of single or double staged procedure is based on the patient’s condition and expertise of treating surgeon.
We have treated this floating hip injury in a single stage. Single stage surgery can potentially reduce the morbidity and also reduce the rate of post-operative complications and accelerate the rehabilitation. In our case, both the fractures were fixed in lateral decubitus position without any requirement for intraoperative change of position of the patient. Even though femoral nailing in lateral decubitus position is technically more demanding, it is very useful technique to reduce operative time. The problem of delayed union was solved with the administration of teriparatide. At the end of one year of follow-up, our patient was pain free and was able to walk, squat and perform activities of daily living quite comfortably.
On the acetabular side, even though a transverse fracture was presented, these type B injuries essentially act as posterior injuries which can be adequately stabilised by fixation of posterior column and wall without requirement of additional anterior fixation. Our inference, it that each case is unique and the operative management, sequence of fracture fixation and choice of implant should be according to the treating surgeon. A report by Abdellatif et al mentioned about use of external fixator initially as part of damage control orthopaedics for treatment of ipsilateral floating hip and knee.14
Conclusion
Floating hip is a rare complex injury associated with high rates of complications. It is a life changing injury that has a major impact on the patient’s quality of life. as, residual pain and limitation of function are invariably present which may prevent the patient from regaining his pre-injury quality of life. From the surgeon’s point of view, there is still a lot of uncertainty regarding the sequence of fixation of fracture due to the complexity of the trauma and associated injuries. Single stage fixation in lateral decubitus position after adequate resuscitation and evaluation can offer a good outcome by reducing the operative time and post- operative complications.

