










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Articulo
 texto en
texto en  Español (pdf)
Español (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkRevista de Ciencias Médicas de Pinar del Río
versión On-line ISSN 1561-3194
Rev Ciencias Médicas vol.27 no.1 Pinar del Río ene.-feb. 2023 Epub 01-Ene-2023
Articles
Most frequent oral communication disorders in pediatric age
1University of Medical Sciences of Pinar del Río "Pepe Portilla" Pediatric Provincial Hospital. Pinar del Río, Cuba.
2University of Medical Sciences of Pinar del Río. Faculty of Medical Sciences "Dr. Ernesto Che Guevara de la Serna". Pinar del Río, Cuba.
3University of Medical Sciences of Pinar del Río Luis Augusto Turcios Lima Polyclinic. Pinar del Río, Cuba
Introduction:
the learning of the mother tongue constitutes for many the greatest intellectual feat that man can accomplish. Men express themselves, exchange ideas and are understood in most cases through oral communication. It is necessary that the individual possesses the minimum skills and knowledge to understand and also generate a normal language, through the harmonious work of the three levels of oral communication: language, speech and voice.
Objective:
to characterize the behavior of oral communication alterations in pediatric age patients in the province of Pinar del Río, attended at the Pepe Portilla Pediatric Hospital, in the period 2017-2021.
Methods:
an observational, descriptive, longitudinal and retrospective study was carried out, taking data from the logophoniatric clinical history that were processed by means of the statistical system InfStat 1.0. The universe and the sample consisted of 539 patients who met the inclusion criteria.
Results:
67,7 % of the sample was male; 52,9 % of the patients were evaluated for the first time between 3 and 5 years of age; secondary delay in language development was the most frequent disorder, followed by dyslalia. Attendance for evaluation at the provincial center varied depending on the municipality of origin.
Conclusions:
early diagnosis of oral communication disorders, timely treatment and the united work of parents and rehabilitators are fundamental in the success of the development of the child's language skills.
Key words: COMMUNICATION; LANGUAGE; SPEECH; VOICE; CHILD
INTRODUCTION
The learning of the mother tongue constitutes for many the greatest intellectual feat that man accomplishes. Men express themselves, exchange ideas and are understood in most cases through oral communication. It is necessary that the individual possesses the minimum skills and knowledge to understand and also generate a normal language, through the principle of functional unity of the three levels of oral communication: language, speech and voice.1,2
Before the child acquires language as such, he or she must go through the learning of sounds, the formation of words, their combination into sentences, the construction of meanings and the acquisition of knowledge about his or her language, until reaching the desired goal: the mastery of language itself.3,4,5,6
Language refers to the whole system of expressing and receiving information in a meaningful way; it consists of understanding and being understood through verbal, non-verbal and written communication.
A child is considered to have delayed language development when the quantitative or qualitative use of language is below the average figure for children of the same age. The factors that cause these difficulties are varied and may be associated with diseases, perinatal sequelae or poor management of the socio-communicative area at early ages.(1
Speech is the verbal expression of language and includes articulation and verbal fluency. speech disorders refer to difficulties in the production of the sounds required for speech or verbal fluency. They may be characterized by a disruption in the flow or rhythm of speech, or constitute problems with sound formation due to articulation or phonological disorders.(7
The voice is any sound emission produced by the laryngeal organ that serves to communicate a being with the surrounding world, whose basic function within communication is to be the emotional affective channel. It is affected when acoustic-clinical alterations of vocal qualities appear; fundamentally of the tone, timbre, intensity, resonance and intonation.(8
There may be a combination of several problems and it would be difficult to understand what a person with an oral communication disorder is saying.
Both the lack of language and the difficulties in its realization and comprehension limit the individual's ability to receive and understand what he/she is saying.
Both the lack of language and the difficulties in its realization and comprehension limit in the individual the possibilities of receiving and transmitting information and, consequently, hinder the normal development of all cognitive processes and especially thinking.
There are defects in oral communication such as simple dyslalia, which do not have such a serious impact on the intellectual development of the individual, but as they constitute "violations" from the aesthetic point of view and are not received naturally in many cases by those around the sufferer, they cause in the affected person a negative reaction to their defect that is reflected in social and work life in an obvious way. (7
Withdrawal, distrust, negativism, maladjustment, phobia to oral communication, are, among others, the characteristics of the behavior of individuals with oral communication disorders, in most cases, and if we add to this the school failures and difficulties in learning that these phenomena can bring with them, we are forced to recognize that these characteristics of the individual who suffers them and the surrounding environment, depending on their severity, may have a greater or lesser psychological and social repercussion, ranging from small limitations to express themselves before the group, to serious alterations of the personality, major failures and limitations in the learning process or in working life, depending on the case.
In the clinical practice of the Speech Therapy and Phoniatrics specialty, which is developed in the pediatric age, we frequently find cases of children in which the harmonic work of the three levels of oral communication does not occur, or occurs with certain irregularities.
The manifestation of this health problem corresponds to the world statistics which indicate that, in school children, the prevalence of language disorders is 2-3 %; the prevalence of speech disorders is 3-6 %; and in some children there are both problems. The prevalence in preschool children is much higher, 15 %.4
The authors of this work consider children to be the sector of the population most qualitatively affected by any oral communication disorder, which has repercussions on the integral development of the child, considering the psychological, pedagogical and social alterations they cause in the medium and long term.
In order to evidence these results, the following objective has been proposed: to characterize the behavior of oral communication disorders in pediatric age patients in the province of Pinar del Río, attended at the Pepe Portilla Pediatric Hospital, in the period 2017-2021.
METHODS
An observational, descriptive, longitudinal, retrospective, descriptive research was carried out during the period from January 2017 to December 2021 in the Speech Therapy and Phoniatrics consultation of the Pediatric Hospital "Pepe Portilla", Pinar del Río.
The study universe was integrated by the 539 patients of the province of Pinar del Río with the diagnosis of oral communication alterations who were attended at the Pediatric Hospital "Pepe Portilla", between January 2017 and December 2021. The 539 patients who met the following criteria were taken as a sample to conform the study:
Patients with a diagnosis of oral communication disorders.
That their parents wished to cooperate in the research with prior informed consent.
They were evaluated in the area of oral communication in the period selected for the study.
The following variables were collected: gender, race, municipality of origin, age of speech-language evaluation, speech-language diagnosis.
Statgraphics Plus version 5.1 for Windows was used as the main software for the statistical processing of the data. The analysis included descriptive procedures, graphic options and relative frequency data. Independence analysis was performed on the basis of contingency tables and the Chi-square test was used as a criterion. Summary measures were used for qualitative data (percentage) and summary measures for quantitative data.
Ethics
The research was conducted following the ethical principles of respect for persons, beneficence, nonmaleficence, justice and autonomy. A consent document was prepared and signed by the parents, for their agreement to participate in the research, based on its objectives, characteristics, the meaning of the results and its scientific purposes with respect for their identities.
RESULTS
By applying the proposed methodology, a characterization of the studied sample was obtained according to sex, of the 539 patients attended with oral communication alterations, in the Province of Pinar del Río from January 2017 to December 2021.
As shown in Graph 1, of the total sample, 365 were male and 174 were female, corresponding to 67,7 % and 32,3 %, respectively.
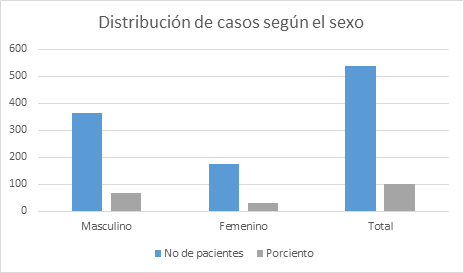
Graph 1. Distribution of cases according to sex. "Pepe Portilla" Pediatric Provincial Hospital.2021
In relation to race, 396 patients (73,5 %) were white and 143 (26,5 %) were black.
Table 1 shows the distribution of cases according to the age of the first speech-language evaluation. Of the total, in 191 (35,4 %) the first speech-language evaluation was performed between 3 and 5 years of age, in 157 (29,1 %) between 5 and 7 years of age, in 97 (18 %) after 8 years of age, in 70 (13 %) between 2 and 3 years of age and in 24 (4,5 %) between 1 and 2 years of age. There was no evaluation during the prelanguage stage between birth and the first year of age.
Table 1 Distribution of cases according to the age of the first speech-language evaluation.
| Age of speech-language evaluation | Number of cases | % | Accumulated frequency |
|---|---|---|---|
| From 0 a 1 years old | 0 | 0 | 0 |
| From 1 a 2 years old | 24 | 4,5 | 4,5 |
| From 2 a 3 years old | 70 | 13 | 17,5 |
| From 3 a 5 years old | 191 | 35,4 | 52,9 |
| From 5 a 7 years old | 157 | 29,1 | 82 |
| More than de 8 years old | 97 | 18 | 100 |
| Total | 539 | 100 | 100 |
Source: clinical history data
Patients evaluated between 3 and 5 years of age predominated, followed by those aged 5 to 7 years and more than 8 years.
The distribution of cases according to the presence of Logofoniatric Syndromes is shown in Table 2. Of the total number of patients evaluated, 252 presented a Disintegrative Syndrome (46,.8 %), 140 (25,9 %) a Disarticulatory Syndrome, 60 (11,2 %) a Dysfluency Syndrome, 5 (0,9 a Dysresonance Syndrome, 58 (10,8 %) a Dysphonia Syndrome. In 16 patients (2,9 %) concomitant Dysarticulatory and Dysfluency Syndrome and in 8 patients (1,5 %) Dysarticulatory and Dysphonia Syndrome were present.
Table 2 Distribution of cases according to the presence of Logophoniatric Syndromes.
| Syndromes | Number of cases | Percentage |
|---|---|---|
| Disintegrative | 252 | 46,8 |
| Dysarticulatory | 140 | 25,9 |
| Dysfluency | 60 | 11,2 |
| Disarticulatory + Disfluence | 16 | 2,9 |
| Dysarticulatory + Dysphonia | 8 | 1,5 |
| Dysresonancial | 5 | 0,9 |
| Dysphonia | 58 | 10,8 |
| Total | 539 | 100 |
Source: clinical history data
During the presumptive logofoniatric diagnosis, the cases studied were classified as shown in Table 3, where there was a higher incidence in 252 cases that represent 46.8% of the total cases whose diagnosis was Language Development Delay, coinciding with the 252 cases whose Syndrome is Disintegrative, there were no patients with Disintegrative Syndrome.
There were 134 cases diagnosed with Dyslalia (24,9 %) and 6 with Dysarthria (1,11 %), corresponding to Dysarticulatory Syndrome.
In relation to the Dysfluency Syndrome, there were 43 patients (7,9 %) with physiological stuttering, 9 (1,7 %) with definite stuttering and 8 (1,5 %) with definite stuttering.
In relation to voice alterations, 58 patients (10,8 %) presented chronic functional dysphonia and 5 (0,9 %) were diagnosed with hyperrinolalia secondary to operated cleft palate.
There were 8 patients with concomitant functional dyslalia and dysphonia (1,5 %) and 16 patients with dyslalia and physiological tartarism (2,8 %).
Table 3 Distribution of cases according to presumptive speech-language diagnosis
| Speech-language diagnosis | Number of cases | Percentage |
|---|---|---|
| Delay in language development | 252 | 46,8 |
| Dyslalia | 134 | 24,9 |
| Dysarthria | 6 | 1,11 |
| Physiological stuttering | 43 | 7,9 |
| Definite stuttering | 9 | 1,7 |
| Definite stuttering | 8 | 1,5 |
| Functional dysphonia | 58 | 10,8 |
| Hyperrinolalia | 5 | 0,9 |
| Dyslalia + Dysphonia | 8 | 1,5 |
| Dyslalia + Physiological stuttering | 16 | 2,8 |
| Total | 539 | 100 |
Source: medical history data
Figure 2 shows how the percentage distribution of the sample studied behaved according to the etiological classification of the total number of cases with language development delay. Primary delay was diagnosed in 23 patients (9,1 %) and secondary delay in 229 (90,9 %).
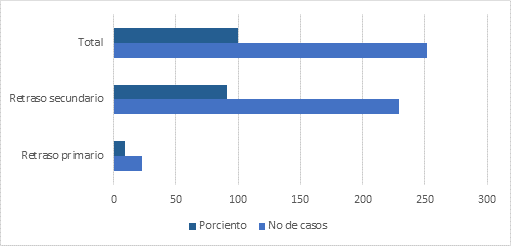
Graph 2 Distribution of cases according to etiological classification of language development delays.
The etiological classification of secondary language development delay is shown in Table 4. Poor verbal stimulation predominated as a secondary cause in 96 patients (41,9 %), family overprotection in 54 (23,6 %), autism in 29 (12,7 %), hypoacusis in 25 (10,9 %), intellectual disability in 11 (4,8 %), bilingualism in 8 (3,5 %) and Static lesion of the central nervous system (SIDS) in 6 (2,6 %).
Table 4 Distribution of cases according to etiological classification of secondary language developmental delay
| Aetiological classification | Number of cases | Percentage |
|---|---|---|
| Intellectual disability | 11 | 4,8 |
| Autism | 29 | 12,7 |
| Hearing impairment | 25 | 10,9 |
| LESNC | 6 | 2,6 |
| Poor verbal stimulation | 96 | 41,9 |
| Family overprotection | 54 | 23,6 |
| Bilingualism | 8 | 3,5 |
| Total | 229 | 100 |
Source: clinical history data
The analysis of the distribution of patients according to the municipalities of origin behaves as follows as shown, the largest number of patients evaluated corresponds to the municipality of Pinar del Río with 441 for 81,8 %, from Consolación del Sur 21 patients were evaluated for 3,9 %, from Guane 14 (2,6 %), from La Palma 2 (0,4 %), from Viñales 10 (1,6 %), Minas de Matahambre 13 (2,5 %), Los Palacios 6 (1,2 %), Sandino 8 (1,5 %), Mantua 2 (0,4 %), San Luis 13 (2,4 %), San Juan y Martínez 9 (1,9 %).
DISCUSSION
When reviewing the bibliography, studies on oral communication disorders predominate in isolation, in relation to the concept of diseases and forms of prevention. These do not allow us to have an exact reference of the percentage behavior in relation to the characterization of patients with oral communication disorders in population groups, as they differ from the method used in this work.3,5,6,8
The results coincide with the national and global trend regarding the high prevalence of language and speech disorders both at school age and preschool age.1,2,3,4)
In this regard Moreno,4) points out that, in school children, the prevalence of language disorders is 2-3 %; the prevalence of speech disorders is 3-6 %; and in some children there are both problems. It refers to the fact that the prevalence of these disorders in preschool children is much higher and can reach 15 %. This study addresses the issue in a general sense, specifically pointing out the causes of language and speech disorders, without statistical studies that favor comparison with the results obtained.
In several studies, the authors coincide in the predominance of oral communication disorders in the male sex.1,2,3,5
The analysis of the age of the first speech-language evaluation of pediatric patients shows that it was late. This makes it impossible to diagnose the alterations during the pre-language and first language stages, losing the greater period of brain plasticity of the first postnatal stages with a worse prognosis in rehabilitation.
It coincides with a study carried out in a national consultation of neurodevelopmental evaluation in patients with perinatal risk factors, which showed that the ages of the first specialized consultation to children with oral communication disorders were between 2,07 and 5 years for 43,2 %, followed by those between 1 and 2,06 years (39,2 %); this is considered late, which makes early diagnosis impossible and delays timely treatment.(5
For the early detection of language development disorders, it is necessary to know that the ontogenesis of language begins with the initial cry of the newborn and continues in an ascending process of development according to the physical and mental development of the child, until the use, fixation and communicative automation of a phonetic-lexico-syntactic means of oral expression, which constitutes a true code of signals.
Its evaluation allows an evolutionary follow-up of the language development where linguistic skills become increasingly complex and allows us to detect if the child's communication is behind its peers in the acquisition of language skills.
Early detection of these alterations allows us to take advantage of the brain's "vulnerability" to environmental influence, which is greater in the early stages of postnatal development than in later stages.
In Cuba, a program is designed to monitor the growth and development of children through childcare consultations by specialists in General Comprehensive Medicine and Pediatrics, in addition to follow-up in neurodevelopmental consultations if they have biological and/or social risk factors, where the following areas are evaluated: motor, cognitive, autonomy habits, and sociocommunicative.
As soon as the alteration in the socio-communicative area is detected, the patient should be referred for a specialized evaluation, where a speech-language diagnosis is made and speech therapy is initiated to establish or restore undeveloped, altered or interrupted linguistic communication in the child, based on vocalizations, fun strategies and games according to their age, which will stimulate them to use their language.
Speech and language therapy is the area of Speech therapy is the area of rehabilitation that works with children who present speech, language and/or communication difficulties, problems with the production of sounds, or difficulties with language learning, that is, failures in combining words to express ideas.9,10
The speech therapist specialized in therapy for oral communication disorders knows that the afferent information that arrives through the different sense organs should not be isolated from the communication process, everything that is done and happens is susceptible to be verbalized. It will work in a global way skills: preverbal, auditory, articulatory, linguistic, speech and cognitive.1
Taking into account the results of this study, the Disintegrative Syndrome and the Disarticulatory Syndrome predominated.
The Disintegrative Syndrome is characterized by interference in the formation of afferences that give rise to the origin, development and consolidation of the functional scaffolding of dynamic language stereotypes. It is a frustrating physiology. The basic common symptom is the partial or total difficulty in the development of language both qualitatively and quantitatively. Both primary and secondary language delays belong to this syndrome.
On the other hand, the disarticulatory syndrome occurs when there are difficulties in the pronunciation of phonemes and may or may not be a consequence of a neurological disorder.
Several authors report language developmental delays and dyslalia as the most frequent causes of consultation at preschool age, being the language disorder an impairment in the development of the ability to understand or use words in union, verbally and nonverbally. Some characteristics of language disorders include improper use of words and their meanings, inability to express ideas, inadequate grammatical patterns, reduced vocabulary, and inability to follow instructions.1,2,4,10,13
Regarding the etiological classification of secondary delays in language development, we agree with studies that show that poor verbal stimulation and family overprotection with poor use of technology associated with changes in the lifestyles of the population are among the most frequent causes that can lead to a delay in language development.1,2,3,4
In relation to what was described in the previous paragraph, the LESNC, hypoacusis, intellectual deficit and global developmental disorders are described as the most serious causes of language delay.4,6,10,14
It is agreed with Centeno (2019) in addressing that voice overuse (overuse) and high intensity voice with effort (misuse), common in children, contribute to the pathophysiology of dysphonias in the pediatric age.8
The analysis of the distribution of the patients according to the municipality of origin, reveals a greater evaluation of patients from the provincial head municipality, but not from the remaining municipalities.
The factors that make it difficult for patients to attend the provincial center are the lack of proximity to the center, transportation difficulties and the presence in the different rehabilitation rooms of the municipalities of Speech-Language Pathologists capable of evaluating, diagnosing, indicating therapy and following up on the indicated treatment in the less severe cases with oral communication disorders.
According to the results of other researches, there is agreement that rehabilitation can last for years, and its levels progress depending on several factors, such as the age of diagnosis, the cause, the participation of the rehabilitator and the family in the rehabilitation.6,9,14,15
In this regard Ayala,10 agrees that the motivation and dedication of the family is essential for the prognosis in the rehabilitation of the patient. This improves the results of the therapy, the child's incorporation into general education is achieved, as well as his social reintegration, thus increasing his quality of life.
It must be taken into account that, if the child's dispositions for language acquisition are important, the language directed to the child by the members of his immediate environment is no less important. None of the components is sufficient in itself to ensure normal language development: all the systems involved in language, speech and voice without the linguistic environment are inoperative.
Knowledge of the problem in oral communication allows the specialist to catch children early in the preschool stage and ensure that appropriate services are provided. Early treatment can significantly modify language learning and thus avoid the complications that affect its development 4).
It can be concluded that the early diagnosis of oral communication disorders, timely treatment and the united work of parents and caregivers can significantly modify language learning and, thus, avoid the It can be concluded that early diagnosis of oral communication disorders, timely treatment and the joint work of parents and rehabilitators are essential for the successful development of the child's language skills.
BIBLIOGRAPHIC REFERENCES
1. Castillo Valdés L, Olivera Hernández MM, Díaz García D, Rivas Brito A, Martínez Rojas RM. Rehabilitación logofoniátrica en pacientes con implante coclear. Hospital Pediátrico Provincial Pepe Portilla. Rev Ciencias Médicas[Internet]. 2021 [citado 29/03/2022]; 25(6): e5231. Disponibleen: http://revcmpinar.sld.cu/index.php/publicaciones/article/view/5231 [ Links ]
2. Castillo Valdés L, Echevarría Cruz A, García Peña EA, Pérez Matos AR. Implante coclear y terapia auditivo verbal en el Hospital Pediátrico Provincial Pepe Portilla. Rev Ciencias Médicas [Internet]. 2021 [citado 29/03/2022]; 25(4): e5063. Disponible en: Disponible en: http://scielo.sld.cu/scielo.php?script=sci_abstract&pid=S1561-31942021000400016&lng=es&nrm=iso 2. [ Links ]
3. Achury Delgado S, Cifuentes Cuartas I M, Lasso Sanceno C, Páez Londoño S. Fonoaudiología en la estrategia de atención integral a la primera infancia de cero a siempre. Universidad del Valle. Facultad de Falud Fscuela de Fehabilitación Fumana. Fantiago de Fali [Internet]. 2015 [citado 29/03/2022]. Disponible en: Disponible en: https://bibliotecadigital.univalle.edu.co/bitstream/handle/10893/10868/CB-0565909.pdf?sequence=1&isAllowed=y 3. [ Links ]
4. Moreno Flagge N. Trastornos del lenguaje. Diagnóstico y tratamiento. RevNeurol[Internet]. 2013 [citado 26/01/2022]; 57(Supl 1): S85-S94 Disponible en: Disponible en: https://pavlov.psyciencia.com/2013/11/Trastornos-del-lenguaje-diagnostico-y-tratamiento.pdf 4. [ Links ]
5. Castillo Valdés L, López Betancourt M, Fernández Peña CL, Olivera Hernández MM, Sotrés León Y. Evaluación del prelenguaje tras aplicación de programa de estimulación en niños con factores de riesgo perinatales. Rev Ciencias Médicas[Internet]. 2014 [citado 20/03/2022]; 18(2). Disponible en: Disponible en: https://www.medigraphic.com/cgi-bin/new/resumen.cgi?IDARTICULO=48578 5. [ Links ]
6. Méndez Hurtado DE. Importancia de la evaluación del lenguaje oral en niños de 4 a 5 años. Ciencia Latina Revista Multidisciplinar [Internet] 2022 [citado 13/04/2022]; 6(1). Disponible en: Disponible en: https://ciencialatina.org/index.php/cienciala/article/view/1875/2668 6. [ Links ]
7. Wollfsdorf J. Que son los trastornos del habla. [Internet]; 2020 [citado 20/03/2022]. Disponible en: Disponible en: http://www.nicklauschildrens.org/condiciones/trastornos-del-habla 7. [ Links ]
8. Diana Centeno A, Maximiliano Penna R. Caracterización de los pacientes con disfonía evaluados en laUnidad de Voz Pediátrica del Hospital Dr. Luis Calvo Mackenna. Rev. Otorrinolaringol. Cir. Cabeza Cuello [Internet]. 2019 [citado 20/03/2022]; 79: 18-24 Disponible en: Disponible en: https://www.scielo.cl/pdf/orl/v79n1/0718-4816-orl-79-01-0018.pdf 8. [ Links ]
9. Ribalta L G, et al. Resultados del programa de implantes cocleares de Clínica Las Condes a 20 años de su inicio: Serie clínica 1994-2015. Rev. Otorrinolaringol. Cir. Cabeza Cuello [Internet]. 2018 [citado 17/03/2021]; 78(3): 275-280. Disponible en: Disponible en: https://www.scielo.cl/scielo.php?pid=S0718-48162018000300275&script=sci_abstract 9. [ Links ]
10. Ayala Paredes MA, Pluas-Arias NZ, Pacherress SF. La terapia del lenguaje, fonoaudiología o logopedia. Pol. Con [Internet]. 2017 [citado 04/04/2021]; 2(5): 1230-1339. Disponible en Disponible en https://polodelconocimiento.com/ojs/index.php/es/article/view/216 10. [ Links ]
11. Guzmán OC, Fuentes López E, Cardemil MF. Resultado del programa nacional de implantes cocleares y garantías explicitas en salud en beneficiarios pertenecientes al servicio de salud Aconcagua. Rev. Otorrinolaringol. Cir. Cabeza cuello. [Internet]. 2020 [citado 17/03/2021]; 80(3): 273-279. Disponible en: Disponible en: https://www.scielo.cl/scielo.php?script=sci_arttext&pid=S0718-48162020000300273 11. [ Links ]
12. Márquez Ibañes N, Santana Hernández E. Comportamiento de la hipoacusia no sindrómica en una familia del municipio de Urbano Noris. Holguín. GacMédEspirit [Internet]. 2017 [citado 23/01/2021]; 19(1): 51-61. Disponible en: Disponible en: http://scielo.sld.cu/scielo.php?script=sci_abstract&pid=S1608-89212017000100008 12. [ Links ]
13. Rodríguez Veloz Y, Veloz Cruz l, Reyes Estrada R. Las ayudas técnicas. Recurso para garantizar la inclusión educativa de personas con discapacidad auditiva. Conrado [Internet]. 2018 [citado 17/03/2022]; 14(63): 229-234. Disponible en: Disponible en: http://scielo.sld.cu/scielo.php?script=sci_abstract&pid=S1990-86442018000300229 13. [ Links ]
14. Rojas Céspedes L. La importancia de la evaluación del lenguaje. [Internet]; 2021 [citado 20/03/2022]. Disponible en: Disponible en: www.fundacionquerer.org/la-importancia-de-la-evaluacion-del-lenguaje 14. [ Links ]
15. Peñafiel Puerto M. Indicadores tempranos de los trastornos del lenguaje. Centro de Invervención del Lenguaje. Colegio Legamar. Leganés. Madrid. [Internet]; 2016 [citado 13/04/2022]. Disponible en: Disponible en: https://www.aepap.org/sites/default/files/4t2.4_indicadores_precoces_de_los_trastornos_del_lenguaje.pdf 15. [ Links ]
Received: July 25, 2022; Accepted: November 21, 2022

