










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Articulo
 texto en
texto en  Español (pdf)
Español (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkRevista de Ciencias Médicas de Pinar del Río
versión On-line ISSN 1561-3194
Rev Ciencias Médicas vol.27 supl.1 Pinar del Río 2023 Epub 01-Jul-2023
Articles
Dental erosion and hypersensitivity in adults, "Neodental" dental office
1Autonomous Regional University of the Andes. Santo Domingo, Ecuador.
ABSTRACT Introduction: enamel, dentin and dental cementum surfaces are subject to a variety of destructive processes. Exposure of dentin can lead to sensitivity, esthetic problems and pulp exposure. Objective: To analyze dental erosion and hypersensitivity in patients between 27 and 56 years of age who attended the "Neodental" dental office in Ecuador. Methods: An observational, descriptive, cross-sectional, descriptive study was carried out on adult patients between 20 and 56 years of age who were examined in the dental office "Neodental", Ecuador, during the period September-December 2022. The universe was composed of 42 patients, of whom a sample of 20 patients was obtained by simple random sampling, according to the inclusion and exclusion criteria. The data were obtained from the clinical history of the patients and a survey prepared for this purpose. The variables used were statistically described by means of relative percentage frequencies. Results: 40 % of the sample brushed once a day, showing a deficient oral hygiene, only 20 % brushed three times and only 15 % of the population brushed four times, which was recognized as an efficient oral hygiene and brushing. Sixty percent of the sample did not know about dental erosion, while 40 % of the remaining sample knew about the pathology. Seventy percent of the sample consumed medications containing vitamin C, and the remaining 30 % consumed them infrequently or not at all. Conclusions: Patients with hypersensitivity and dental erosion are generally diagnosed in time when the dental piece still has a good prognosis.
Key words: TOOTH EROSION; DENTAL ENAMEL; HYPERSENSITIVITY; RISK FACTORS
INTRODUCTION
Dental erosion was first described in 1933 and was named Mylolysis, which is defined as acid wear through chemical processes, while Erosive Dental Erosion (EDD) is the loss of dental tissue through dissolution by acids maintaining a worldwide prevalence, those clinically diagnosed lesions were correlated with the rate of intake of soft drinks, natural beverages or energy drinks, tooth sensitivity when consuming food.
Dental erosion consists of irreparable damage to the dental enamel with origins of non-carious chemical processes, that is, by means of acids that dissolve the dental enamel, in the ages that most affect erosion in children this being more likely to have children in private schools than public school children.(1
At present it has been demonstrated that it is not feasible to prophesy exactly the location of erosive wounds depending on their etiology, however, erosion will damage certain teeth more than others. From a clinical perspective certain common properties are described, where dental erosion wounds show up in both lingual and vestibular regions, especially in the gingival third, as small depressions or shallow wounds, wider than deep, disc-shaped, spoon-shaped or irregular.1
Once it shows up in occlusal regions it does so in the form of gutter or pits, the prevalence of erosive wounds in children and young people has been increasing considerably in the era. For such an impact, different indexes have been developed for the diagnosis of dental erosion to of a simple to use index that evaluates with a numerical scale the proportion of wear present and also evaluates, according to the score obtained, the need for the procedure of the piece.(2
It is evident that dental erosion is a very common pathology in infants. Dental erosion is directly related to risk factors such as: consumption of sweetened tea, intake of energy drinks and gastro-esophageal reflux (GER), among others. Children and adolescents are a vulnerable population, given that there is evidence of studies that confirm it, involving different factors where the citric acid present in the diet plays a fundamental role, acid candies, acid salivary pH, socioeconomic stratum and dental erosion in children.(2
Dental hypersensitivity is the most common cause of toothache and has been described as an intense, sharp, stabbing pain. It is associated with loss of enamel, exposure of dentin, cementum and gum tissue. It is also related to diet, bad habits, poor brushing techniques and tooth whitening. Various treatments, toothpastes or mouthwashes are used for relief. It may contain products such as calcium phosphate, potassium nitrate and 8 % arginine. The chemicals act by clogging the renal tubules or reducing nerve transmission to the pulp.
Enamel, dentin and cementum surfaces are subject to a variety of destructive processes. Dentin exposure can lead to dentin sensitivity, esthetic problems and pulp exposure. This is where oral prevention, diagnosis and timely treatment of various non-carious cervical lesions begins. With this we can appreciate the delicacy of the treatments when an adult patient has sensitivity problems.3
We were particularly interested in this subject in adults where these dental pathologies are more frequently manifested, which in the long term can be the gateway for dental emergencies to appear. For this reason we decided to analyze dental erosion and hypersensitivity in patients between 27 and 56 years of age.
METHODS
An observational, descriptive, cross-sectional, descriptive study was carried out in adult patients between 20 and 56 years of age examined in the dental office "Neodental", Ecuador, in the period September-December 2022. The universe was composed of 42 patients, of whom a sample of 20 patients was obtained by simple random sampling, according to the inclusion and exclusion criteria. The data were obtained from the patients' medical records and a survey prepared for this purpose.
Inclusion criteria
Adult patients between 27 and 59 years of age with possible signs of dental erosion.
Patients who agreed to help and collaborate with this investigation on a voluntary basis.
Exclusion criteria
Individuals whose primary interest was in the care and treatment of dental caries were excluded.
Patients who were not interested in participating in the research or answering the survey.
The variables used in the investigation were: number of times they brushed, knowledge of dental erosion, presence of dental sensitivity, frequency of consumption of medicines containing vitamin C.
To obtain the information the clinical histories of the patients were used, as well as the examination carried out during the consultations. The data obtained were stored in a database prepared for this purpose. Descriptive statistics were used for the study of the variables, by calculating absolute and relative percentage frequencies.
The principles of bioethics and the aspects established in the Declaration of Helsinki were complied with.
RESULTS
forty percent of the sample brushed once a day, showing a deficient oral hygiene, only 20 % brushed three times and only 15 % of the population brushed four times, which is recognized to determine efficient brushing and oral hygiene (Fig. 1).
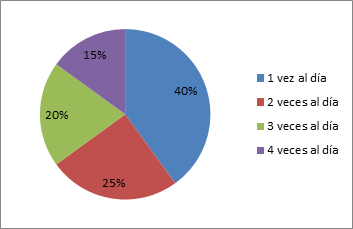
Fig. 1 Number of times a day they brushed.
60 % of the sample did not know about dental erosion, while 40 % of the remaining sample knew about the pathology because they were receiving or had received treatment for erosive problems in their teeth, these results indicate that more than half of the sample did not know about the pathology and more about the risk that it represents in the long term (Fig. 2).
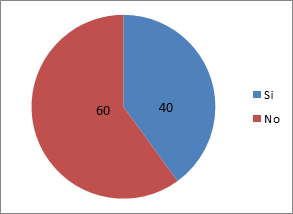
Fig. 2 Knowledge of dental erosion.
Forty percent of the sample, that is, eight persons presented low category discomfort or pain in the teeth when ingesting hot or cold foods, thus showing the existence in almost half of the sample of probabilities of suffering dental sensitivity not related to caries but to problems of dental erosion due to loss of enamel (Fig. 3).
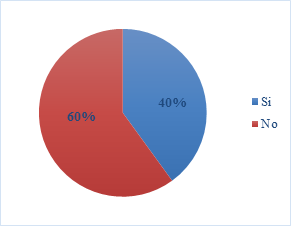
Fig. 3 Presence of dental sensitivity.
Seventy percent of the sample consumes medicines containing vitamin C, and the remaining 30 % consumes them infrequently or not at all, these results are subject to various reasons such as the season, depending on the season there is a higher rate of diseases such as flu, which causes an increase in the consumption of Vitamin C, which when consumed frequently either every day or at least four to five per week can represent irreparable damage to the enamel (Fig. 4).
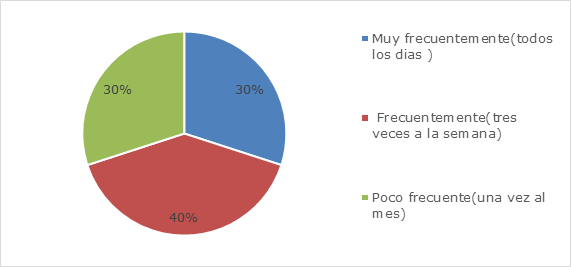
Fig. 4 Frequency of consumption of medications containing Vitamin C.
DISCUSSION
It is important that within the anamnesis that the dentist asks the patient, questions about his diet, the type of beverages he consumes and if he suffers from gastroesophageal reflux. The dentist should also ask if the patient clenches his teeth on a regular basis or when sleeping. If the patient reports that he/she does not suffer from gastroesophageal reflux or dental clenching, but if he/she habitually consumes carbonated beverages or fruit juices based on lemon, grape, orange, lime, among others; the diagnosis of dental erosion of extrinsic origin could be confirmed. In these cases, poor dietary habits play an important risk factor.4
As a treatment, dietary habits should be modified, reducing the consumption of acidic foods and avoiding carbonated beverages. Regarding hygiene habits, it is recommended to use toothpaste with more than 1450 ppm of fluoride and a soft bristle toothbrush to minimize any additional wear of the teeth. It is important to highlight that oral hygiene after consuming this type of beverages should be at least 30 minutes. This recommendation is given for oral hygiene in general, however, consumption of these beverages significantly increases acidity in the mouth which could cause abrasive lesions on the teeth.5
Larsen et al.6 in 2000 proposed an evaluation index that has different erosion locations and also includes a severity level based on the criteria of Smith and Knight reported in 1984.
Skogedal et al.7 in 1977 in a study of dental erosion in Norway in a factory where electrolytic methods were used to extract zinc, found a relationship between the severity of erosion and the number of teeth affected throughout the service, with a high prevalence of dental erosion.
Lussi et al.,8 in a 1991 study in Swiss adults, detected a prevalence of dental erosion of 7,7 % on vestibular surfaces in the 26-30 years age group. Dental erosion was included in 1993 in the United Kingdom in the National Dental Child Health Review. A total of 17,061 children aged five to 15 years were examined using a modification of the Smith & Knight Index.
On the other hand, the UK National Diet and Nutrition Study of children aged 1 ½ and 4 ½ years showed that 10% of the children had dental erosion on the vestibular surfaces of the upper incisors and 19% on the palatal surfaces. The review showed a weak relationship between frequent consumption of sugar-sweetened and carbonated soft drinks and dental erosion, with the time of consumption (bedtime) of these drinks most closely associated with the frequency of erosion.(9
The 1996 National Diet and Nutrition Review in the population aged four to 18 years found that more than half of this population group had some signs of erosion, occurring mainly on the palatal surfaces of upper incisors in subjects aged 11 to 14 years at 42 % and 56 % in those aged 15 to 18 years.(10
Al-Malik et al.,10 in 2002, in Saudi Arabia, mentioned that because traditional dietary habits and practices have continued but food and beverage products typical of Westernized diets are now cheap and readily available, particularly in major cities, dental erosion occurs more often. The study reported that the palatal surfaces and the most affected are the central and lateral incisors, the children showed two or more teeth affected with erosion.
Similarly, they found little relationship between erosion and social class, as measured by type of school or parental occupation. Erosion affected almost one third of the preschool sample in Jeddah, and the presence of caries was a significant predictor of erosion. A year later, Nunn et al.,11 in 2003 mention that epidemiological reports in the UK and worldwide over the past 10 years have reported the prevalence of tooth decay and indicate that it has increased among different ages over time, with tooth erosion being the most common form of childhood wear facets.
Millward et al.,12 in 1994, in a study in Birmingham, England, state that there is very little published information on the severity of tooth wear in children. Tooth wear was observed in more than 80 % of the upper incisors and 30 % of the primary molars had some exposed dentin. There was a highly significant difference between the three groups in relation to liquid intake habits; the average number of carbonated beverages consumed weekly by the children in the groups was 'mild', 'moderate' and 'severe'.
Liñan-Duran et al.,13 in 2007 evaluated in vitro the erosive effect of three carbonated beverages on the tooth surface and concluded that the comparison between the study groups shows that the carbonated beverages present erosive effect measured by the variation of the surface microhardness. The Kola Real® beverage presented a similar erosive effect to the Coca Cola® carbonated beverage, while Inca Kola® presented the least erosive effect in comparison with the previous ones, and this difference was statistically significant.
Ehlen et al.(14 in 2009 compared acidic beverages to identify the risk of dental erosion in vitro, and found that the depth of the lesion in enamel and root surface during exposure to Gatorade® was greater than that produced by Red Bull® and Coca Cola®. These three beverages were more erosive than Diet Coke® and apple juice by 100 %.
Teeth have a high functional and esthetic value. It is important to know the eruption processes of permanent teeth in the population in order to detect dental anomalies in time, which can affect the scheduling of dental and orthodontic treatment.(15,16
CONCLUSIONS
In this investigation we learned about a little researched pathology called dental erosion and its growing impact in modern times thanks to industrialization, and the foods that change the current diet of people, the lack of knowledge of correct hygiene, as well as showing that dental erosion is also related to other important factors such as salivary flow, alcohol consumption, the work environment together with direct or indirect contact with chemical substances or gases and prolonged consumption of medications with Vitamin C, medicines for chest pain or aspirin, the work environment together with direct or indirect contact with chemical substances or gases and the prolonged consumption of medications with Vitamin C, medications for chest pain or aspirin, thus highlighting the importance of maintaining a balanced diet with regard to acidic foods and citric foods that when consumed in the long term can pose a risk to our oral cavity.
BIBLIOGRAPHICAL REFERENCES
1. Alvarado T, Abigail P. Factores de riegos que producen la erosión dental en niños y adolescentes. Facultad Piloto de Odontología. Universidad de Guayaquil, Ecuador; 2021. [ Links ]
2. Hayakawa Lastarria LA, Gallo Oropeza A, Casas-Apayco L. Prevalencia de erosión dental en estudiantes de 12 a 16 años utilizando Basic Erosive Wear Examination (BEWE) en una institución educativa pública peruana. Rev Odontopediatria Latinoam [Internet]. 2019 [Citado 20/01/2023]; 9(1): 12. Disponible en: Disponible en: https://revistaodontopediatria.org/index.php/alop/article/view/162 2. [ Links ]
3. Saltos A, Ivonne V. La erosión dental asociada al consumo de bebidas carbonatadas en jóvenes de 19 a 25 años de la Facultad de Odontología de la Universidad Central del Ecuador período 2016-2017. Quito : UCE [Internet]; 2017 [Citado 20/01/2023]. Disponible en: Disponible en: http://www.dspace.uce.edu.ec/handle/25000/10517 3. . [ Links ]
4. Zero DT, Lussi A. Erosion - chemical and biological factors of importance to the dental practitioner. Int Dent J [Internet]. 2005 [Citado 20/01/2023]; 55(4):285-89. Disponible en: Disponible en: https://pubmed.ncbi.nlm.nih.gov/16167607/ 4. . [ Links ]
5. Fernández C, Marchena L, García B. Erosión dental: caso clínico. REDOE. [Internet] 2014 [Citado 20/01/2023]. Disponible en: Disponible en: http://www.redoe.com/print.php?id=156 5. . [ Links ]
6. Larsen IB, Westergaard J, Stoltze K, Larsen AI, Gyntelberg F, Holmstrup P: A clinical index for evaluating and monitoring dental erosion. Community Dent Oral Epidemiol. [Internet]. 2000 [Citado 20/01/2023]; 28(3): 211-217. Disponible en: Disponible en: https://pubmed.ncbi.nlm.nih.gov/10830648/ 6. [ Links ]
7. Skogedal O, Silness J, Tangerud T, Laegreid O, Gilhuus-Moe O. Pilot study on dental erosion in a Norwegian electrolytic zinc factory. Community Dent Oral Epidemiol [Internet]. 1977 [Citado 20/01/2023]; 5(5): 248-251. Disponible en: Disponible en: https://onlinelibrary.wiley.com/doi/epdf/10.1111/j.1600-0528.1977.tb01649.x 7. [ Links ]
8. Lussi A, Schaffner M, Hotz P, Suter P. Dental erosion in a population of Swiss adults. Community Dent Oral Epidemiol [Internet]. 1991 [Citado 20/01/2023]; 19: 286-290. Disponible en: Disponible en: https://onlinelibrary.wiley.com/doi/abs/10.1111/j.1600-0528.1991.tb00169.x 8. [ Links ]
9. Walker A, Gregory J, Bradnock G, Nunn JH, White D. National Diet and Nutrition Survey: Young people aged 4-18 years. Volume 2: report of the oral health survey. London: The Stationery Office [Internet]; 2000 [Citado 20/01/2023]. Disponible en: Disponible en: https://www.researchgate.net/publication/285868082_National_Diet_and_Nutrition_Survey_Young_People_Aged_4-18_years 9. [ Links ]
10. Al-Malik MI, Holt RD, Bedi R. Erosion, caries and rampant caries in preschool children in Jeddah, Saudi Arabia. Community Dent Oral Epidemiol [Internet]. 2002 [Citado 20/01/2023]; 30(1): 16-23. Disponible en: Disponible en: https://pubmed.ncbi.nlm.nih.gov/11918571/ 10. [ Links ]
11. Nunn JH, Gordon PH, Morris AJ, Pine CM, Walker A. Dental erosion - changing prevalence? A review of British national children's surveys. Int J Paediatr Dent [Internet]. 2003 [Citado 20/01/2023]; 13(2): 98-105. Disponible en: Disponible en: https://pubmed.ncbi.nlm.nih.gov/12605627/ 11. [ Links ]
12. Millward A, Shaw L, Smith AJ, Rippin JW, Harrington E. The distribution and severity of tooth wear and the relationship between erosion and dietary constituents in a group of children. Int J Paediatr Dent [Internet]. 1994 [Citado 20/01/2023]; 4(3): 151-157. Disponible en: Disponible en: https://onlinelibrary.wiley.com/doi/abs/10.1111/j.1365-263X.1994.tb00124.x 12. [ Links ]
13. Liñan-Duran C, Meneses-López A, Delgado- Cotrina L. Evaluación in vitro del efecto erosivo de tres bebidas carbonatadas sobre la superficie del esmalte dental. Rev Estomatol Herediana [Internet]. 2007 [Citado 20/01/2023]; 17(2): 58-62. Disponible en: Disponible en: https://revistas.upch.edu.pe/index.php/REH/article/view/1859 13. [ Links ]
14. Ehlen LA, Marshall TA, Qian F, Wefel JS, Warren JJ. Acidic beverages increase the risk of in vitro tooth erosion. Nutr Res [Internet]. 2008 [Citado 20/01/2023]; 28(5): 299-303. Disponible en: Disponible en: https://pubmed.ncbi.nlm.nih.gov/19083423/ 14. [ Links ]
15. Santacruz Fajardo MC, Chamorro Mafia Ana C. Diagnóstico y epidemiología de erosión dental. Rev. Univ. Ind. Santander Salud [Internet]. 2011 [Citado 20/01/2023]. 43(2). Disponible en: Disponible en: http://www.scielo.org.co/scielo.php?script=sci_arttext&pid=S0121-08072011000200009 15. [ Links ]
16. Hernández Cuétara L, Pérez Pupo DT, Fernández Queija Y, Limonta Pérez I. Cronología y secuencia de erupción dentaria permanente en niños de 5 a 12 años. Salud, Ciencia y Tecnología [Internet]. 2021 [citado 20/01/2023]; 1(2021): 23. Disponible en: Disponible en: https://revista.saludcyt.ar/ojs/index.php/sct/article/view/23 16. [ Links ]
Received: December 20, 2022; Accepted: March 08, 2023

