










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Articulo
 texto en
texto en  Español (pdf)
Español (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkRevista de Ciencias Médicas de Pinar del Río
versión On-line ISSN 1561-3194
Rev Ciencias Médicas vol.27 supl.1 Pinar del Río 2023 Epub 01-Jul-2023
Articles
Evaluation of a patient with several chronic diseases in primary care: a case report
1Universidad Regional Autónoma de los Andes. Quevedo, Ecuador
ABSTRACT Introduction: chronic non-communicable diseases combined with an increase in life expectancy, often result in patients with multiple chronic non-communicable diseases, which requires action and comprehensive assessment by health personnel to reduce the burden of care and improve the quality of life of the patient. Case presentation: we present the case of a female patient, 65 years of age, illiterate, bedridden for two years due to obesity, sedentary. She has a history of arterial hypertension, chronic gastric ulcer and diabetes mellitus. A comprehensive evaluation of the patient was carried out by primary health care using different tools. Treatment readjustment is performed, and follow-up plans are established together with pending charts. Conclusions: patients with chronic diseases constitute a challenge for the primary care physician, requiring strategic preventive planning focused on avoiding the complications of these diseases that lead to more personal stress for the family and more outflow of resources for the state. The follow-up plans together with the pending tables are a basic and indispensable tool to follow the chronology of what to do with the patient and his family, together with a general panorama of the patient's life and prognosis. The adaptation of programs and guidelines according to the patients and their diseases and the collaboration of the patients themselves helps the primary care physician to offer a better care to the patient.
Key words: PRIMARY HEALTH CARE; CHRONIC DISEASE; NONCOMMUNICABLE DISEASES; QUALITY OF LIFE.
INTRODUCTION
The arrival of an illness in a family member determines changes in the members and is considered as a difficulty that alters the functioning of the family nucleus. Adjustment to this new environment allows changes, which generate adaptations that lead the family to a new state of equilibrium and place the patient at risk with reference to their care.1,2
In the natural evolution of the disease, a high percentage of patients reach a satisfactory resolution; however, a small number may become chronically ill, requiring special care; others, on the contrary, reach the terminal phase and become dependent on palliative care.3 In any of these cases, the care and treatment by the family physician is of great importance, since he/she is directly linked to the family and knows the data and actual situation of the patient.4
In general, the nature of chronic diseases makes health care providers and their staff get involved to placate and slow down the ailments, although they cannot be cured or reversed, primary care teams strive to improve the quality of life of patients.5 In this aspect, the first level of care plays an indispensable role, responsible for ensuring coverage in the biological, psychological and social sphere of the patient and his or her family.6
In the treatment of chronic diseases, primary health care plays an indispensable role, as well as comprehensive networks for the continuous provision of services over time in all life cycles, with emphasis on multidisciplinary groups, patient care and research systems, all for the support and development of the population and patients.7
Given the complexity of chronic diseases, it is difficult to control them and to reduce their complications.8 The family physician combines already established systems and adapts them for the benefit of individuals,9 implements strategies at the level of care and improves the care of chronic patients through: self-management, mutual peer support, informal caregiver support, home visits and tele-care (telephone calls), all focused on the patient, in addition to self-care education that promotes adherence to treatments and timely arrest of complications.10
The case of a patient with several chronic diseases is presented, as well as the care provided by the primary health care physician and the planned follow-up.
CASE REPORT
Female patient, 65 years old, resident of the city of Manta, Catholic, married with children, illiterate, economically dependent on her children. She has been bedridden for two years due to obesity, which makes it difficult for her to walk. She has a history of arterial hypertension (diagnosed in 2015 and treated with losartan 50 mg per day), chronic gastric ulcer (diagnosed in 2018 and treated with omeprazole 40mg every 24 hours) and diabetes mellitus (diagnosed in 2019 and treated with metformin 500mg every 12 hours).
The son attends the patient's scheduled medical appointment, requesting continued medication. He refers the impossibility for the patient to go to the doctor's office due to transportation difficulties. The health team decides to make a home visit to evaluate the case.
The socioeconomic survey shows that the patient is a housewife, unemployed, who depends financially on a solidarity voucher. She owns her own home, has access to drinking water and public sewage system along with daily garbage collection and electricity.
As toxic habits, the patient has a history of alcohol consumption, without smoking or consumption of illicit substances. On interrogation, the patient reports consumption of three full meals a day, little hydration of one liter a day, daily catharsis, diuresis once or twice a day, with sleep of approximately five to six hours a night. Her bathing is daily, with help.
On interrogation she reports heartburn, occasional postprandial epigastralgia, occasional constipation.
On physical examination there is erythema on the face of three days of evolution, which is caused by the application of alcohol. On the face there were stigmata of scratching and erythematous areas, neck with the presence of acanthosis in areas of folds. Pupillary reflexes were diminished in the eyes. In the mouth there were incomplete dental pieces in the lower jaw and absence of dental pieces in the upper jaw, she commented to have prosthesis that is only placed at the time of feeding. In the cardiovascular system blood pressure was 120/80 mmHg and heart rate 80 bpm. In the lower limbs there was evidence of a grade A-1 ulcer on the sole of the foot according to the Texas classification.
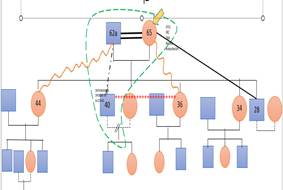
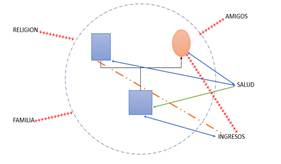
Ecomap (figure 1) and familiogram (figure 2) were performed, determining nuclear family, adult, with close relatives, traditional, urban marginal, with permeable limits.
The individual analysis shows a mature adult, within the stage of integrity versus despair according to Erikson, where she admits her mortality and fears death due to the helplessness of her partner. She also presents low therapeutic adherence. We proceeded to establish the list of problems (table 1)
Tabla 1 Lista de problemas.
| No | Problem | Type of problem | Active | Passive |
|---|---|---|---|---|
| 1 | Hipoacusia | Biological | X | |
| 2 | HBP | Biological | X | |
| 3 | DM | Biological | X | |
| 4 | Gastritis | Biological | X | |
| 5 | Obesity | Biological | X | |
| 6 | Sleep disturbance | Biological | X | |
| 7 | Polyhospitalizations | Biological | X | |
| 8 | Allergic dermatitis | Biological | X |
Treatment was readjusted, indicating losartan in tablets 50 mg orally every 12 hours, metformin in tablets at a dose of 500 mg every 12 hours and pramoxine acetate plus zinc for topical application on the face.
An educational talk was given, explaining the need for daily cleansing, adequate nutrition and the beginning of physical activity routines. A schedule of visits is made, anticipatory guidelines for falls establish guided appointments in consultation and a table of pending first visit is established (table 2).
Tabla No 2 Pendientes primera visita.
| No | Pending | Aim | Deadline |
|---|---|---|---|
| 1 | Family APGAR | Analyze intrafamily relationships | Medium term |
| 2 | Survival scales | Refer patient to programs | Short term |
| 3 | Frailty and dependency scales | Helps analyze risks and type of supervision required by patient | Short term |
| 4 | Caregiver scale | Determine support required by primary caregiver | Medium term |
| 5 | Depression scale | For caregiver and patient | Medium term |
| 6 | Elaborate follow-up plan | Assesses basic activities of daily living | Mixed terms |
| 7 | Katz Index | Assesses basic activities of daily living | Short term |
| 8 | Lawton and Brody Scale | Assesses basic activities of daily living | Short term |
A follow-up plan was prepared, which included the following actions:
Confrontation of health team
Classification of patient to the most appropriate plan
Follow-up through home visits
Coordinate medication delivery
Education - self-education - peer education
Treatment education
Orientation to healthy eating
Coordination of referrals
Coordination of consultations with primary caregiver
Coordination with family members
DISCUSSION
In order to guarantee excellence in health services, as well as to make proposals and modifications to the current regulations, it is necessary to study the processes of care. In the case of chronic noncommunicable diseases, the analysis of the provision of services in primary health care is a necessity, given their impact on individual health and population dynamics.
Rosero Acosta et al.11 made a case report on the presence of chronic diseases in an older adult patient. They reported the onset of arterial hypertension (AHT) at the age of 60 years, and later, due to sedentary behaviors and unhealthy habits and lifestyles, she developed diabetes mellitus (DM). Similar data were found in the present case report.
In Ecuador, different studies have analyzed the prevalence of HT in various populations. Álvarez Marín et al.12 studied the prevalence of HT in the administrative staff of an institution in Machala-Ecuador; they found a predominance of women (59,3 %) and over 30 years of age with the presence of this entity. Mejía Navarro et al.13 carried out a study to estimate the frequency of arterial hypertension in adults in the Mexico neighborhood, Pastaza, Ecuador, where they found a prevalence of 8,96 %, with a predominance of women and a mean age of 64,5 ± 13,2 years,
Regarding diabetes mellitus, Núñez-González et al.14 analyzed trends and spatiotemporal analysis of mortality due to diabetes mellitus in Ecuador, 2001-2016. They recorded 57 788 deaths due to diabetes mellitus in Ecuador in the period. A significant rise in DM mortality was reported in women (1,50 %; p<0,001).
Aging, together with situations such as overweight, obesity and sedentary lifestyle are risk factors for developing diabetes mellitus. If to this is added the previous existence of HT, the risk increases considerably.15 Therefore, the presence of both diseases (HT and DM) in the patient is not a rare occurrence.
Chronic diseases are characterized by their slow and prolonged evolution, progressiveness and complications in the short, medium and long term. Living with a chronically ill patient in the family is a dynamic, contextual process that is affected by the patient's state of health. Although it may take years before a significant deterioration in the patient's health is required, this limits to some extent the family dynamics, generating costs of medical care and medication, adaptation of food and the replacement of roles within the home.16
One of the greatest repercussions for the family, according to the authors, is when there is a limitation in the activities of daily living, as well as when it is necessary to fulfill the role of formal caregiver or not. In the present case, the patient shows a limitation for mobilization and activities such as bathing, hence to some extent the family functioning may be affected.
One of the main functions of the primary health care physician should be to prevent the existence of disease in his or her patients. Once they have an established disease, they must achieve a therapy capable of reducing the impact of the disease on their health, as well as preventing its possible complications. This requires strategic action planning, similar to that carried out in the present study.
At present, chronic diseases constitute a challenge for health systems; their impact can be considered pandemic, and surpasses infectious and contagious diseases. Policies should be drawn up for health prevention as a tool for better medical care.
CONCLUSIONS
Patients with chronic diseases are a challenge for the primary care physician, requiring strategic preventive planning focused on avoiding the complications of these diseases that lead to more personal and family stress and more outflow of resources for the state. The follow-up plans together with the pending tables are a basic and indispensable tool to follow the chronology of what to do with the patient and his family, together with a general panorama of the patient's life and prognosis. The adaptation of programs and guidelines according to the patients and their diseases and the collaboration of the patients themselves helps the primary care physician to offer a better care to the patient.
BIBLIOGRAPHIC REFERENCES
1. Salazar-Barajas ME, Garza-Sarmiento EG, García-Rodríguez SN, Juárez-Vázquez PY, Herrera-Herrera JL, Duran-Badillo T. Funcionamiento familiar, sobrecarga y calidad de vida del cuidador del adulto mayor con dependencia funcional. Enfermería Univ [Internet]. 2019 [citado 12/01/2023]; 16(4):[aprox 10 pp]. Disponible en: Disponible en: http://www.revista-enfermeria.unam.mx:80/ojs/index.php/enfermeriauniversitaria/article/view/615 1. [ Links ]
2. Duran-Badillo T, Herrera Herrera JL, Mireles Alonso ME, Oria Saavedra M, Ruiz Cerino JM. Funcionamiento familiar y calidad de vida en adultos mayores con hipertensión arterial. Cienc y Enfermería [Internet]. 2022 [citado 12/01/2023]; 28:e7385. Disponible en: Disponible en: https://revistas.udec.cl/index.php/cienciayenfermeria/article/view/7385/ 2. [ Links ]
3. García-Maset R, Bover J, Segura de la Morena J, Goicoechea Diezhandino M, Cebollada del Hoyo J, Escalada San Martín J, et al. Documento de información y consenso para la detección y manejo de la enfermedad renal crónica. Nefrología [Internet]. 2022 [citado 12/01/2023]; 42(3):233-64. Disponible en: Disponible en: https://linkinghub.elsevier.com/retrieve/pii/S0211699521001612 3. [ Links ]
4. Rodríguez Eguizabal E, Gil de Gómez MJ, San Sebastián M, Oliván-Blázquez B, Coronado Vázquez V, Sánchez Calavera MA, et al. Capacidad de respuesta del sistema de salud en atención primaria valorada por pacientes con enfermedades crónicas. Gac Sanit [Internet]. 2022 [citado 12/01/2023]; 36(3):232-9. Disponible en: Disponible en: https://linkinghub.elsevier.com/retrieve/pii/S0213911121000480 4. [ Links ]
5. Caparrós Boixés G, Suñer Soler R, Juvinyá Canal D, Reig Garcia G. El impacto de la pandemia de la COVID-19 en el control de las enfermedades crónicas en atención primaria. Atención Primaria [Internet]. 2022 [citado 12/01/2023]; 54(1):102233. Disponible en: Disponible en: https://linkinghub.elsevier.com/retrieve/pii/S0212656721002675 5. [ Links ]
6. Blay C, Martori JC, Limon E, Lasmarías C, Oller R, Gómez-Batiste X. Cada semana cuenta: uso de dispositivos sanitarios y costes relacionados de una cohorte comunitaria de personas con enfermedades crónicas avanzadas. Atención Primaria [Internet]. 2019 [citado 12/01/2023]; 51(6):359-66. Disponible en: Disponible en: https://linkinghub.elsevier.com/retrieve/pii/S021265671830009X 6. [ Links ]
7. Arroyo de la Rosa A, Bayona Huguet X. Guía de Atención Domiciliaria: pura atención primaria. Atención Primaria [Internet]. 2019 [citado 12/01/2023]; 51(9):527-8. Disponible en: Disponible en: https://linkinghub.elsevier.com/retrieve/pii/S0212656719304743 7. [ Links ]
8. Pascual López L, Colomar Martínez JL. Análisis de la atención recibida por pacientes con enfermedad crónica avanzada en el ámbito de atención primaria. Atención Primaria [Internet]. 2022 [citado 12/01/2023]; 54(4):102306. Disponible en: Disponible en: https://linkinghub.elsevier.com/retrieve/pii/S0212656722000269 8. [ Links ]
9. Manterola C, Otzen HT, García N, Mora V. M. Guías de práctica clínica basadas en la evidencia. Rev Cir (Mex) [Internet]. 2019 [citado 12/01/2023]; 71(5):[aprox. 10 pp]. Disponible en: Disponible en: https://www.revistacirugia.cl/index.php/revistacirugia/article/view/416 9. [ Links ]
10. Contento Escaleras M del C. Impacto de los programas de atención primaria en salud durante la pandemia [Tesis de Pregrado]. Ecuador: Universidad Estatal del Sur de Manabí; 2021 [citado 12/01/2023]. Disponible en: Disponible en: http://repositorio.unesum.edu.ec/handle/53000/2891 10. [ Links ]
11. Rosero Acosta J, Santacruz Quiñonez S, Vallejo Muñoz RE. Enfermedades crónicas del adulto mayor: Reporte de caso. Boletín Inf CEI [Internet]. 2021 [citado 12/01/2023]; 8(2):117-27. Disponible en: Disponible en: https://revistas.umariana.edu.co/index.php/BoletinInformativoCEI/article/view/2693 11. [ Links ]
12. Álvarez Marín MG, Álvarez Marín AM, Carrión Arias LE, Villa Feijóo AL, Arriciaga Nieto AK, Porres Gonzaga KJ, et al. Prevalencia de hipertensión arterial y correlación con los factores de riesgo psicosociales en el personal administrativo de una institución de Machala-Ecuador. Rev Latinoam Hipertens [Internet]. 2020 [citado 12/01/2023]; 15(2):112-7. Disponible en: Disponible en: https://www.redalyc.org/articulo.oa?id=170265474007 12. [ Links ]
13. Mejía Navarro AA, Mejía Navarro JC, Tenorio Correa SM. Frecuencia de Hipertensión Arterial en personas adultas del Barrio México, Puyo, Pastaza, Ecuador. Rev Cuba Reumatol [Internet]. 2020 [citado 12/01/2023]; 22(2):[aprox. 10 pp]. Disponible en: Disponible en: https://revreumatologia.sld.cu/index.php/reumatologia/article/view/707 13. [ Links ]
14. Núñez-González S, Delgado-Ron A, Simancas-Racines D. Tendencias y análisis espacio-temporal de la mortalidad por diabetes mellitus en Ecuador, 2001-2016. Rev Cuba Salud Pública [Internet]. 2020 [citado 12/01/2023]; 46(2):[aprox. 15 pp]. Disponible en: Disponible en: https://revsaludpublica.sld.cu/index.php/spu/article/view/1314/1580 14. [ Links ]
15. Mayorga Valverde JN. Atención Primaria de Salud en el manejo integrado de pacientes con enfermedades crónicas no transmisibles [Tesis de Pregrado]. Universidad Nacional De Chimborazo; 2020 [citado 12/01/2023]. Disponible en: Disponible en: http://dspace.unach.edu.ec/handle/51000/7169 15. [ Links ]
16. Ambrosio L, Navarta-Sánchez MV, Meneses A, Rodríguez-Blázquez C. Escala de convivencia con un proceso crónico: estudio piloto en pacientes con enfermedades crónicas. Atención Primaria [Internet]. 2020 [citado 12/01/2023]; 52(3):142-50. Disponible en: Disponible en: https://linkinghub.elsevier.com/retrieve/pii/S0212656718304141 16. [ Links ]
Received: January 17, 2023; Accepted: August 08, 2023

