










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Articulo
 texto en
texto en  Español (pdf)
Español (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkRevista de Ciencias Médicas de Pinar del Río
versión On-line ISSN 1561-3194
Rev Ciencias Médicas vol.27 no.4 Pinar del Río jul.-ago. 2023 Epub 01-Jul-2023
Articles
Characterization of patients with healthcare-associated infections
1University of Medical Sciences of Pinar del Río. León Cuervo Rubio" Clinical Surgical Teaching Hospital. Pinar del Río, Cuba. University of Medical Sciences of Pinar del Río. General Teaching Hospital "Abel Santamaría Cuadrado". Pinar del Río, Cuba. University of Medical Sciences of Pinar del Río. Provincial Pediatric Teaching Hospital "Pepe Portilla". Pinar del Río, Cuba. University of Medical Sciences of Pinar del Río. Raúl Sánchez" Teaching Polyclinic. Pinar del Río, Cuba. University of Medical Sciences of Pinar del Río. Faculty of Medical Sciences "Dr. Ernesto Che Guevara de la Serna". Pinar del Río, Cuba.
ABSTRACT Introduction: healthcare associated infection is the localized or generalized condition resulting from the adverse reaction to the presence of an infectious agent or its toxin, and which was not present or in incubation period at the time of the patient's admission to the hospital. Objective: to characterize patients with care-associated infections at the "Pepe Portilla" Provincial Pediatric Teaching Hospital between January 1 and December 31, 2018. Methods: observational, descriptive and cross-sectional study between January and December 2018. The universe was studied in its entirety and was constituted by 453 patients according to established selection criteria. Descriptive statistical methods such as absolute and relative percentage frequencies were used to analyze the results. Results: the most frequent age group was between one and five years old (32,67 %) and male sex (53,20 %). The most frequent site of infection was respiratory (42,83 %), followed by enteral and phlebitis (19,43 %). The total rate of infections was 2,7 x 100 live discharges and in terms of services, the highest rate was obtained in progressive care (14,7). Candida (36,36 %) was reported as the most frequent microorganism and 8,47 % of the patients submitted to artificial ventilation or with central venous catheter presented some infection. Conclusions: in the period studied, HCAI had a higher incidence in males and children under five years of age; there was a higher rate of infection in closed wards, with Candida being the most frequent causative germ and it was related to the use of catheters.
Key words: INFECTION; CROSS INFECTION; SEPSIS; CARE FACILITIES.
INTRODUCTION
The term hospital comes from the Latin "hospitium" and means "care of the sick". Hospitals, intended to save lives, can paradoxically become important reservoirs of biological agents, causing infections that are often severe and resistant to the use of antibiotics.1
Healthcare-associated infections (HAI) are one of the major public health problems affecting patients in hospital units worldwide. It is defined as the localized or generalized condition resulting from adverse reaction to the presence of an infectious agent or its toxin, and which was not present or in incubation period at the time of the patient's admission to the hospital. Nosocomial bacterial infections can appear from 48 to 72 hours after the patient's admission and mycotic infections after five days of stay, although the time may be shortened due to invasive procedures and intravascular therapy.2
Although for more than a decade many of the infection control efforts of health care workers have been aimed at providing a safer hospital environment for patients, the incidence of healthcare-associated infections remains high. According to World Health Organization statistics, an average of 8,7 % of hospital patients have nosocomial infections, with an attributable mortality that can be as high as 35-55 %, depending on the type of infection. The most frequent are those of surgical wounds, urinary tract (related to the use of bladder catheters), lower respiratory tract (trachea and bronchi) and those associated with the use of catheters.3
The pediatric population is particularly special and should be analyzed differently when addressing the problem of nosocomial infections, since it has its own characteristics that differentiate it from the adult population (such as its immunological immaturity). Barragán et al.,4 in a pediatric intensive care unit established a prevalence of nosocomial infection of 33,3 %, with males being more frequently affected.
A study carried out in the ICU of the "Gustavo Aldereguía" Hospital in Cienfuegos revealed a nosocomial infection rate of 5,2 to 10,8 %, with a tendency to decrease. The overall rate of deaths due to sepsis and its cause ranged from 1,5 to 7,3 %.3
The overall mortality attributed to nosocomial infections in pediatrics is estimated at 11 %. Regardless of its nature, it doubles the burden of nursing care, triples the cost of drugs, and increases the cost of tests to be performed by seven times.2
Even more important are the costs in human lives; it is estimated that infection is the cause of death in 1 to 3 % of admitted patients. It is estimated that figures as impressive as those reported in the United States of 25 to 100 thousand deaths per year are to be had.1
In summary, healthcare-associated infections contribute significantly to hospital morbidity and mortality, as well as to the excessive cost of hospitalized patients due to increased hospital days and high social costs generated by the disabilities and deaths they cause.5
Taking into account these precepts, it was decided to conduct this research, addressing the following scientific problem: What was the behavior of healthcare-associated infections in the "Pepe Portilla" Provincial Pediatric Teaching Hospital during 2018?
METHODS
An observational, descriptive and cross-sectional study was conducted at the "Pepe Portilla" Provincial Pediatric Teaching Hospital "Pepe Portilla" of Pinar del Río during 2018. The universe was studied in its entirety and consisted of 453 patients, chosen according to the following selection criteria:
Inclusion criteria.
Exclusion criteria
The information was obtained from the database of the hygiene and epidemiology department of the institution and from the review of the patients' medical records. For the analysis of the information, descriptive statistical methods were used, such as the calculation of absolute frequencies, percentages as a summary measure for qualitative and quantitative data, as well as the calculation of the mean as a measure of central tendency for quantitative data.
The data obtained were processed and presented through frequency distribution tables and graphs elaborated with Microsoft Excel 2013 software for better understanding and discussion. A database was created and elaborated to facilitate the processing of the information, with the support of the software itself. The variables studied were age, sex, location of the infection, hospital service where the infection occurred, causal germ and their association with the use of catheters.
In the research conducted, the data obtained were used for strictly scientific purposes and will only be disclosed in duly accredited scientific events or publications. The research was approved by the Hospital's Scientific Council and the principles and recommendations for physicians in biomedical research on human subjects adopted by the 18th World Medical Assembly in Helsinki in 1964 and finally ratified at the 41st World Assembly held in Hong Kong in 1991.
RESULTS
In the distribution according to demographic variables of sex and age of the patients (Table 1), there was a slight predominance of the male sex (53,20 %) and of patients between one and five years of age (32,67 %). The average age of contracting a nosocomial infection in the series was 11,92 years.
Table 1 Distribution of patients with healthcare-associated infection according to sex and age. Provincial Pediatric Teaching Hospital "Pepe Portilla". Pinar del Río, 2018.
| Age groups (years) | Male | Female | Total | |||
|---|---|---|---|---|---|---|
| No. | % | No. | % | No. | % | |
| Less than 1 | 47 | 19,50 | 57 | 26,89 | 104 | 22,96 |
| 1 to 5 | 82 | 34,02 | 66 | 31,13 | 148 | 32,67 |
| 6 to 10 | 40 | 16,60 | 29 | 13,68 | 69 | 15,23 |
| 10 to 15 | 47 | 19,50 | 39 | 18,40 | 86 | 18,98 |
| 16 to 18 | 25 | 10,37 | 21 | 9,91 | 46 | 10,15 |
| Total | 241 | 53,20 | 212 | 46,80 | 453 | 100 |
Mean = 11,92
In relation to the location of the infection (graph 1), it was observed that the respiratory type predominated with 42,83 %. In second place was phlebitis, 19,65 %, followed by infections of enteral location.
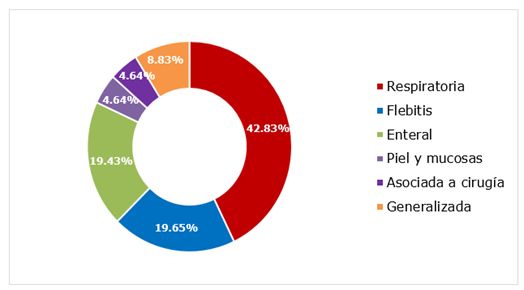
Graph 1 Distribution of patients with healthcare associated infection according to location of the infection.
When stratifying by services (Table 2), it could be seen that the greatest number of nosocomial infections developed in the miscellaneous 1 service (18,54 %), followed immediately by the gastroenterology and respiratory tract services, both with 17,44 %.
Table 2 Distribution of patients with healthcare-associated infection according to hospital service.
| Hospital service | No. | % | |
|---|---|---|---|
| P E D I A T R I C S | Gastroenterology | 79 | 17,44 |
| Pediatric specialties | 16 | 3,53 | |
| Miscellaneous early childhood | 31 | 6,84 | |
| Miscellaneous second childhood | 16 | 3,53 | |
| Miscellaneous 1 | 84 | 18,54 | |
| Miscellaneous 2 | 49 | 10,82 | |
| Respiratory tract | 79 | 17,44 | |
| Oncohematology | 18 | 3,97 | |
| Progressive care | 29 | 6,40 | |
| PICU | 26 | 5,74 | |
| Surgery | 21 | 4,64 | |
| Orthopedics | 5 | 1,10 | |
| Total | 453 | 100 | |
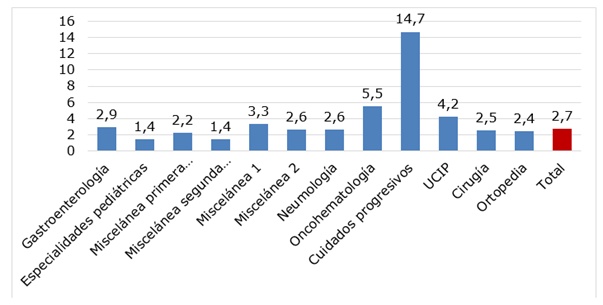
Regarding the rate of nosocomial infections by service (Figure 2), it was found that in the progressive care unit there was a disproportionate peak of infection associated with medical care. The other services oscillated in a stable range between 5,5 (oncohematology) and 1,4 (pediatric specialties and second childhood) and the total rate was 2,8.
After distributing the patients according to the germ causing the nosocomial infection (Table 3), it was possible to identify that out of 66 isolates, the most frequent pathogen was Candida (36,36 %) in the total, as well as in pediatric wards (30 %) and PICU (60 %). However, in the operating room the most frequently isolated germ was E. coli (40 %). On the other hand, in the orthopedics service there was only one isolation and it corresponded to the Enterobacter germ.
Table 3 Distribution of patients with healthcare-associated infection according to causal germ
| Causal germ | Pediatrics | PICU | Surgery | Orthopedics | Total | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| No. | % | No. | % | No. | % | No. | % | No. | % | |
| Staphylococcus epidermidis | 5 | 12,50 | 1 | 5,00 | 0 | 0 | 0 | 0 | 6 | 9,09 |
| Staphylococcus aureus | 2 | 5,00 | 1 | 5,00 | 1 | 20,00 | 0 | 0 | 4 | 6,06 |
| E. coli | 0 | 0 | 0 | 0 | 2 | 40,00 | 0 | 0 | 2 | 3,03 |
| Pseudomona | 5 | 12,50 | 3 | 15,00 | 0 | 0 | 0 | 0 | 8 | 12,12 |
| Enterobacter | 2 | 5,00 | 1 | 5,00 | 1 | 20,00 | 1 | 100 | 5 | 7,58 |
| Acinetobacter | 9 | 22,50 | 2 | 10,00 | 0 | 0 | 0 | 0 | 11 | 16,67 |
| Candida | 12 | 30,00 | 12 | 60,00 | 0 | 0 | 0 | 0 | 24 | 36,36 |
| Otros | 5 | 12,50 | 0 | 0 | 1 | 20,00 | 0 | 0 | 6 | 9,09 |
| Total | 40 | 60,61 | 20 | 30,30 | 5 | 7,58 | 1 | 1,52 | 66 | 100 |
Regarding the occurrence of nosocomial infections secondary to catheterization (Table 4), it was evidenced that this incidence was low with 8,47 % in total. Of the patients with deep venous approach, 12,24 % developed secondary systemic infection and 4,40 % of the ventilated patients developed pneumonia due to this cause. In the sample studied there were no cases of infection secondary to the use of bladder catheterization.
Table 4 Distribution of patients with healthcare associated infection according to infection secondary to catheterization.
| Catheterized patients | HCAI secondary to catheterization | |
|---|---|---|
| No. | %* | |
| Artificial ventilation (n = 91) | 4 | 4,40 |
| Central venous catheter (n = 98) | 12 | 12,24 |
| Total (n = 189) | 16 | 8,47 |
* Relative to the total corresponding procedure
DISCUSSION
The overall HAI rate is currently considered the maximum exponent of the quality of inpatient care and represents an important epidemiological indicator, with values that should not exceed 7 %. Its predominance in children under one year of age, with a decrease in the following age groups, seems to be related to the presence of certain risk factors in this age group.6
Ortega Franco et al.,7 report in their casuistry that the highest number of patients with the disease was found in the one-four years age group (48,28 %) followed by the 10-19 years age group (40,23 %) with a predominance of male sex (57,6 % of the cases), which coincides with the results obtained in the present study.
On the other hand, López Méndez et al.,3 report a predominance of children under one year of age with 178 (34,4 %) children, without analyzing their sex. This coincides with the international literature reviewed, but differs from the results obtained in the present study.
According to World Health Organization (WHO) statistics, the most frequent sites of infection are surgical wounds, urinary tract (related to the use of bladder catheters) and lower respiratory tract (trachea and bronchi), which coincides with authors such as Licorish et al.,8 who in their series reported that the most frequent nosocomial infection was surgical wound infection in 14 patients (24,5 %),followed closely by systemic (22,8 %), in both cases with primacy in those aged five-17 years (30,0 %), although in the total casuistry they predominated in infants between zero and 11 months. In comparison with this study, the results differ significantly.
Saavedra et al.,9 refer among the most frequent types of infection pneumonia (17,3 %), surgical site infection (16,8 %) and urinary tract infection (14,6 %) and Serra Valdés(10) reports that lower respiratory tract infections reached more than 50 % of all infections (pneumonia and bronchopneumonia), which is similar to the results obtained in this study.
With respect to phlebitis, which is reported as the second most frequent cause of nosocomial infection in the present study, several authors report it as an infrequent form of presentation of HCAI. Abreu Pérez,6 reports in his series that it only represented about 8,6 % of the total number of cases, behind Deep Venous Approach infections (31,4 %), ventilator-associated pneumonia (24,3 %), non-focalized infections (22,9 %), bacteremias (21,4 %) and enteral infections (20,0 %).
On the other hand, enteral infections were cited as a frequent cause of HCAI in the research conducted by López Méndez, et al.,3), representing 27,4 % of the total number of cases (n=130), second only to acute respiratory infections, which occurred in 160 children (33,7 %).
Sepsis rates by service vary, depending on the characteristics of each unit, and as the complexity of the unit increases, so does the risk of acquiring nosocomial sepsis.(9 Hence, unlike other hospital services, intensive care units tend to have the highest frequency of HAIs. Patients in these units are particularly affected by such infections because of the severity of their underlying medical problems and the greater number of invasive interventions to which they are subjected. It is estimated that HAIs in ICUs account for 20 % of the total number of HAIs, despite the fact that the number of ICU beds represents only 5-10 % of the number of hospital beds.1
Authors such as Saavedra et al.,9 report in their casuistry that the services that contributed the most patients with HAIs were those belonging to surgical specialties (63,6 %), compared to those belonging to medical specialties (36,4 %), which differs from the present casuistry.
Admás Licorish et al.,8 report in their series that, of the types of infections confirmed in the members of the sample studied, most of them were acquired in the intensive care unit (28 out of 57), especially systemic infection (in 9), which was also the predominant one globally (in 16), followed by infection contracted in the operating room in 11, at the expense of the surgical wound in 10. The remaining ones occurred in patients admitted to the Hematology, Urology and other services, with 7, 2 and 14, respectively, which also differs from the results obtained in the present investigation.
Domínguez Ronquillo,5 refers that, in relation to the type of patient, a predominance of patients with clinical conditions was found with 32 cases (although not broken down by services) (58,2 %), a result that differs from international series where several studies attribute to surgical patients the highest risk of infection, up to 57 % of surgical patients with positive diagnosis of HCAI. These results coincide with those obtained in this study.
Regarding the rate of infections per hospital service, Lugo et al.,2 report in their research that the highest infection rates were reported in the Pediatric Intensive Care Units (17 to 27), Neonatal Intensive Care (13 to 15), Neurosurgery (15 to 25) and Medical Pediatrics (7 to 15), all per 1000 days-stay.
In the present study, although services such as "Miscellaneous 1", "Gastroenterology" or "Respiratory tract" had a high percentage of nosocomial infection (see Table 2), they are not among the services with the highest rate of these infections because the number of patients attended is much higher than the rest of the services; the same is true for oncohematology, progressive care, etc. For example, in the period studied, 2514 patients were admitted to miscellaneous ward 1 compared to only 197 in progressive care.
Regarding the main isolated germs, Riquelme et al.,11 in a study carried out in children with special needs reported that the most frequently identified agents were rotavirus (n: 16; 13,9 %), parainfluenza virus 3 (n: 11; 9,6 %) and adenovirus (n: 4; 3,5 %). Villalobos 12 states that, of 590 isolates obtained from blood samples in intensive care units, 12 % corresponded to Klebsiella pneumoniae; 10,7 % to S. aureus and 5,4 % to E. coli.
Lopez et al.,13 report that the etiology of the infection was identified in 15,91 % of the cases studied, more than half corresponded to Gram-negative bacilli, the most common being P. aeruginosa, K. pneumoniae and E. coli).
With respect to this particular section, it is understood that the prevalence of some germs over others in various hospitals and countries is directly related to the fact that each hospital and each service within that hospital has a differ With respect to this particular section, it is understood that the prevalence of some germs over others in various hospitals and countries is directly related to the fact that each hospital and each service within that hospital and even each service (ward) within the same institution has its own microbiological map (as well as the human organism), which in turn will be related to the procedures carried out, adequate asepsis and antisepsis techniques, etc.
Most of the authors cited here, Cuban and from the international literature consulted, differ from the results obtained in this research where the main germ isolated was Candida albicans.
The use of invasive procedures such as catheters or mechanical ventilation constitutes a risk factor per se for contracting this type of infections. In a study carried out by Vizzuet,14 in neonatal intensive care services, he cites as main risk factors for the development of nosocomial infection the use of vascular catheters: with nosocomial infection 35 days [CI 27 44] vs. without nosocomial infection: 9 [CI 7 10], (p= 0.0000) and endotracheal cannula: with nosocomial infection: 20 days [CI 12 29] vs. without nosocomial infection: 6 [CI 4 9], p= 0.0000.
Lopez et al.,13 found that 25 % (77/308) of nosocomial pneumonias were associated with mechanical ventilation. Of all the cases presented, the etiology causing the infection was identified in 15,.91 % (49/308), isolating a total of nine germs. These figures are higher than those obtained in this study.
Salcedo Reyes,15 reported that in his casuistry secondary bacteremia was associated in 67,9 % with central venous access and in 32,1% with peripheral venous access. Respiratory infection was related to endotracheal intubation (ETI) in 54,2 % and to tracheotomy in 25,0 %, figures that are similar to those observed in the international casuistry but which differ from those obtained in this study.
It was concluded that the age group most frequently affected was one to five years and the male sex. The most frequent site of healthcare-associated infection was respiratory, followed by phlebitis and enteral infections. The highest risk of developing an infection was in the progressive care unit. Of the germs isolated we found that Candida was the most frequent microorganism, followed by Acinetobacter and third place was occupied by Pseudomona. Slightly less than 1 in 10 catheterized patients (artificial ventilation or deep venous approach) had an infection.
BIBLIOGRAPHICAL REFERENCES
1. Pacheco Licor VM, Gutiérrez Castañeda DC, Serradet Gómez M. Vigilancia epidemiológica de infecciones asociadas a la asistencia sanitaria. Rev. cienc. méd. Pinar Río [Internet]. 2014 Jun [citado 14/03/2019]; 18(3): 430-440. Disponible en: Disponible en: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S1561-31942014000300007&lng=es 1. [ Links ]
2. Zamudio Lugo I, Espinosa-Vital GJ, Rodríguez-Sing R, Gómez Gonzalez CJ, Miranda Novales MG. Infecciones nosocomiales. Tendencia de 12 años en un hospital pediátrico. Revista Médica del Instituto Mexicano del Seguro Social [Internet]. 2014 [citado 14/03/2019]; 52(S2): 38-42. Disponible en: Disponible en: https://www.medigraphic.com/cgi-bin/new/resumen.cgi?IDARTICULO=50645 2. [ Links ]
3. López Mendez L, Pastrana Román I, González Hernández JC, Alvarez Reinoso S, Rodríguez Ramos JF. Caracterización de las infecciones nosocomiales. Rev. Ciencias Médicas [Internet]. 2013 Mar-Abr [citado 14/03/2019]; 17(2): 87-96. Disponible en: Disponible en: http://www.medigraphic.com/pdfs/pinar/rcm-2013/rcm132j.pdf 3. [ Links ]
4. Barragán A, López P. Factores de riesgo para infecciones nosocomiales en Pediatría. Rev. Gastrohnup [Internet]. 2012 [citado 14/03/2019]; 14(2): 7-13. Disponible en: Disponible en: http://revgastrohnup.univalle.edu.co/a12v14n2s1/a12v14n2s1art2.pdf 4. [ Links ]
5. Domínguez Ronquillo D, Mestre Villavicencio P, Alvarez Cabrera J, Quesada Carvajal LZ, Sosa Palacios O. Infecciones relacionadas con las asistencia médica en la UCI “William Soler”. Rev. cuban. med. int. emerg. [Internet]. 2014 [citado 14/03/2019]; 13(2): 153-166. Disponible en: Disponible en: http://www.revmie.sld.cu/index.php/mie/article/view/18/59 5. [ Links ]
6. Abreu Pérez D, Lacerda Gallardo Á, Montero Álvarez L, Cerdeira Rodríguez M, Rodríguez Hernández Y, Borrero Marichal R. Infecciones relacionadas con la atención sanitaria en Unidad de Terapia Intensiva Pediátrica / Infections related to health care in Pediatric Intensive Care Unit. MediCiego [Internet]. 2015 [citado 13/03/2019]; 21(1). Disponible en: Disponible en: http://www.revmediciego.sld.cu/index.php/mediciego/article/view/88 6. [ Links ]
7. Ortega Franco CC, Jimenez Sanchez S, Romo Martinez J, Arriaga Dávila JJ. Estudio de prevalencia de infecciones nosocomiales en un hospital pediátrico del tercer nivel de atención. REV. ENF INF MICROBIOL [Internet]. 2014 [citado 14/03/2019]; 34(1): 6-12. Disponible en: Disponible en: http://www.medigraphic.com/pdfs/micro/ei-2014/ei141b.pdf 7. [ Links ]
8. Paris Licorish M, Mariño Castellanos MC, Maceira Soto Z, Castillo Amaro A, Leyva Founier E. Clinical and microbiological characterization of children and adolescents with infections associated with health care. MEDISAN [Internet]. 2018 Mayo [citado 16/03/2019]; 22(5): 508-517. Disponible en: Disponible en: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S1029-30192018000500008&lng=es 8. [ Links ]
9. Saavedra Carlos H, Ordóñez Karen M, Díaz Jorge A. Nosocomial infections impact in a hospital in Bogota (Colombia): effects on mortality and hospital costs. Rev. chil. infectol. [Internet]. 2015 Feb [citado 14/03/2019]; 32(1): 25-29. Disponible en: Disponible en: https://scielo.conicyt.cl/scielo.php?script=sci_arttext&pid=S0716-10182015000200004&lng=es 9. [ Links ]
10. Serra Valdés MA, Farrill Lazo R. La infección hospitalaria en el diagnóstico de salud del Hospital General Docente “Enrique Cabrera”. 2012. La Habana, Cuba. Revista Habanera de Ciencias Médicas. [Internet]. 2014 [citado 14/03/2019]; 13(2): 258-269. Disponible en: Disponible en: http://www.medigraphic.com/pdfs/revhabciemed/hcm-2014/hcm142k.pdf 10. [ Links ]
11. Flores JC, Riquelme P, Cerda J, Carrillo D, Matus MS, Araya G, et al. Mayor riesgo de infecciones asociadas a atención en salud en niños con necesidades especiales hospitalizados. Rev. chil. infectol. [Internet]. 2014 Jun [citado 16/03/2019]; 31(3): 287-292. Disponible en: Disponible en: https://scielo.conicyt.cl/scielo.php?script=sci_arttext&pid=S0716-10182014000300006&lng=es 11. [ Links ]
12. Villalobos AP, Barrero LI, Rivera SM, Ovalle MV, Valera D. Vigilancia de infecciones asociadas a la atención en salud, resistencia bacteriana y consumo de antibióticos en hospitales de alta complejidad, Colombia, 2011. Biomédica [Internet]. 2014 [citado 14/03/2019]; 34(1): 67-80. Disponible en: Disponible en: https://www.redalyc.org/articulo.oa?id=84330489009 12. [ Links ]
13. López D, Aurenty L, Nexans-Navas M, Goncalves ME, Rosales T, Quines M, et al. ETIOLOGÍA Y MORTALIDAD POR NEUMONÍA A SOCIADA A LOS CUIDADOS DE LA SALUD EN PEDIATRÍA. Archivos Venezolanos de Puericultura y Pediatría [Internet]. 2014 [citado 14/03/2019]; 77(1): 9-14. Disponible en: Disponible en: https://www.redalyc.org/articulo.oa?id=367937050003 13. [ Links ]
14. Vizzuett-Martínez R, Aguilar-Lucio AO, Mendoza-Domínguez S, Rodríguez-Zepeda JJ, Rosenthal VD. Infecciones nosocomiales asociadas con procedimientos invasivos enla Unidad de Cuidados Intensivos Neonatales de un hospital del tercer nivel. Revista de Especialidades Médico-Quirúrgicas [Internet]. 2014 [citado 14/03/2019]; 19(1): 12-16. Disponible en: Disponible en: https://www.redalyc.org/articulo.oa?id=47330738003 14. [ Links ]
15. Salcedo Reyes C, Campanioni Romero NL, Villareal Pérez PR, Reyes Navarro E, Gayardo Barrio Y. Infección nosocomial en una unidad de cuidados intensivos pediátrica. Rev. cuban. med. int. emerg. . [Internet]. 2016 [citado 14/03/2019]; 15(3): 85-93. Disponible en: Disponible en: http://www.medigraphic.com/pdfs/revcubmedinteme/cie-2016/cie163j.pdf 15. [ Links ]
Received: September 04, 2022; Accepted: March 28, 2023

