










 Serviços customizados
Serviços customizados Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkIntroduction
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is the etiological agent causing coronavirus diseases with an extensive spectrum of clinical manifestations, from asymptomatic infections to severe illnesses.1,2,3 Asymptomatic subjects are not usually admitted to medical centers; many do not receive a confirmatory diagnosis or do not study their epidemiological contacts.
A protocol that includes symptomatic and asymptomatic patients has its scientific rationale based on the dynamics of the viral infection and its interaction with the host,4,5 a health policy that could be considered excessive since asymptomatic patients are supposed to deploy a good defense against SARS-CoV-2 infection.2 However, with the emergence of new strains, the clinical spectrum expands, with asymptomatic beginnings and torpid evolution being observed, mainly in unvaccinated patients.1,2,3 Since the pandemic period, therapeutic protocols included a robust antiviral therapeutic approach consisting of type I interferon (IFN) + Lopinavir/Ritonavir + Chloroquine combined therapy. Among these components, the IFNs seem to be the foremost pertinent one, being recognized by the World Health Organization (WHO).6 In this sense, the human recombinant interferon-alpha 2b (IFNα-2b) (Heberon Alfa R, Cuba) treatment was used on symptomatic and asymptomatic patients.4,5
There are no reports of standard treatments established for asymptomatic patients because of the lack of adequately designed studies to support a decision.7 In this context, case series studies in which symptomatic and asymptomatic patients are compared in response to specific therapeutic modalities are beneficial to demonstrate the practical impact of antiviral therapies and the importance of even timely treatment in the absence of symptoms.7
This work has the objective to evaluate the treatment contribution of the combined therapy based on human recombinant interferon-alpha 2b + Lopinavir/Ritonavir + Chloroquine vs. Lopinavir/Ritonavir + Chloroquine in asymptomatic and symptomatic COVID-19 patients.
Material and Methods
Study design and subjects in the study
An observational study was carried out in patients with a positive diagnosis of COVID-19 by RT-PCR admitted to “Dr. Luis Díaz Soto” General Hospital from April 1st to July 30th, 2020.
The patients with a positive diagnosis of COVID-19 by Reverse Transcription - Polymerase Chain Reaction (RT-PCR) (5-8) were selected. Patients transferred to another hospital before becoming negative or before completing the treatment were excluded. Those selected as the control group presented contraindications to the use of Interferon.5
The therapy was employed in two groups:
Group 1: Patients who used combined triple therapy based on human recombinant interferon-alpha 2b + Lopinavir/Ritonavir + Chloroquine.
Group 2: Patients who did not use human recombinant interferon alpha 2b, only Lopinavir/Ritonavir + Chloroquine.
For Group 1, from a total of 308 patients treated with interferon + Lopinavir/Ritonavir + Chloroquine admitted to the hospital, we selected a statistically representative sample of 40 patients (described in the statistical analysis section) using a simple randomization process in order to obtain an N statistically comparable to the N of the Group 2 (control).
For Group 2, we selected 27 patients who only received treatment with Lopinavir/Ritonavir + Chloroquine because of real or subjective intolerance to the use of interferon.
This design was necessary due to the low number of patients with real or subjective intolerance to the use of recombinant human interferon-alpha 2b because of its high safety profile. As a result, two groups arose considering the clinical expression of the disease at the time of hospital admission and during hospital stay (symptomatic/asymptomatic).
SARS-CoV-2 diagnosis
All patients enrolled in this study followed the World Health Organization criteria and recommendations using RT-PCR assay from nasopharyngeal + oropharyngeal swab samples.8
Monitoring of the time of negativization
A RT-PCR test was performed on days 9th, 14th, 20th, and 26th after the beginning of the treatment to know the impact of different combined treatment therapy on patients' time to viral clearance.5 Blood extraction was performed during hospital admission and discharge to know the behavior of the inflammatory markers such as neutrophil/lymphocyte ratio, C-reactive protein, and Ferritin according to hospital care protocol.5 Two and four months after discharge from the hospital, second and third blood samples were taken from patients with two consecutive negative RT-PCR results5 to know the serological immunity status.
Serological analysis of IgG, IgA, and IgM SARS-CoV-2 antibody
Costar 3 590 plates coated with 100 µL of 1 µg per well of recombinant SARS-CoV-2 nucleocapsid protein (RNP) and 2 µg per well of S peptide (P77) in Coating Buffer (0,1 M carbonate/bicarbonate buffer pH 9,6). The plates were incubated for one hour at 37 °C. After washing three times with distilled water and 0,05 % Tween 20, the plates were blocked with 250 µL/well of blocking solution (PBS, 2 % Skim Milk Powder, 0,05 % Tween 20, 2,5 % Goat sera) for one hour at 37 °C. 100 µL of blood samples and controls at 1/20 dilution in sample buffer (PBS, 0,2 % Skim Milk Powder, 0,05 % Tween 20, 0,25 % Goat sera), were incubated for 30 minutes at 37 °C. Bound specific IgA, IgM, or IgG antibodies were detected using secondary antibody peroxidase-conjugated diluted in PBS-T solution (2,68 mMKCl, 1,47 mM KH2PO4, 136,89 mM NaCl, 8,1 mM Na2HPO4 and 0,05 % Tween 20). Development of a color reaction was performed adding 100 µL/well of substrate solution of TMB- 3,3', 5,5'-Tetramethylbenzidine (Cat. # T0440, Sigma Life Sciences, USA) incubated at room temp 10 minutes. The reaction was stopped with a stop solution (2 M H2SO4). Microtiter plates were read at a wavelength of 450 nm using a UMELISA reader (PR-521, Tecnosuma Internacional).
Antiviral drugs included in the treatment protocol
Heberon® (Heberon Alpha R, named INF): Recombinant human Interferon-a2b administered by intramuscular injection three 3 million IU three 3 times daily per week.5
Lopinavir/Ritonavir (LPV/RTV, named K): 250 mg, one capsule twice daily (500 mg/day) for 30 days.5
Chloroquine (named C): 150 mg, one1 tablet twice daily (300 mg/day) for 10 days.5
Statistics procedures
The representativeness concerning the total patients admitted during the time designated was calculated from a 5 % error and a 95 % confidence using the following equation:
Where,
 = Desired sample;
= Desired sample;
 = All patients (308);
= All patients (308);
 = 1,96 (95 % confidence);
= 1,96 (95 % confidence);
 = 0,5;
= 0,5;
 = 0,5;
= 0,5;
 = 0,05 (maximum permissible error 5 %)
= 0,05 (maximum permissible error 5 %)
Quantitative variables were presented as mean ± standard deviation (SD). The categorical variables were presented as counts and percentages. Mean comparisons between groups were made using Mann-Whitney test, and the Wilcoxon matched-pairs signed-rank test for non-parametric values was used for paired comparisons. Categorical data was compared using the Chi-square test for proportions comparison. The Kaplan-Meier plot portrayed the time to viral clearance and compared it with a log-rank test. Correlation analysis was performed for variables hypothetically related. The p< 0,05 was considered statistically significant. We used GraphPad Prism 8 to perform all the statistical analyses and figures.
Ethical approval
The Institutional Ethics Committees and Research Board of General Hospitals approved this study that followed the principles of the Declaration of Helsinki.9 The National Expert Group in handling COVID-19 approved this study as well.
This work was carried out with the approval of the national group to fight COVID-19, the Ministry of Public Health, the “Dr. Luis Díaz Soto” Hospital Direction and the Biomedical Research Direction of the Center for Genetic Engineering and Biotechnology.
Each patient was properly informed and decided to participate voluntarily expressing the wish for signing an informed consent. In addition, there were no ethical conflicts when selecting the cases and the treatment scheme due to the results of other clinical trials.
Results
Demographic and clinic characteristics
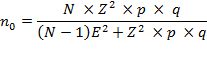
In Group 2, the proportion of female patients (63 %) was significantly higher than in Group 1 (35 %). Instead, the time elapsed between the date of supposed contagion and the date of hospital admission was substantially shorter in Group 2 than in Group 1 (Table 1). Other variables such as age, the clinical expression of the disease, and comorbidities did not show significant differences between both groups (Table 1).
Table 1 Analysis of demographic and clinical characteristics of Group 1 and Group 2
COPD: chronic obstructive pulmonary disease; SD: standard deviations; a Chi-square test (proportions comparison); bMann-Whitney test (independent samples). Source: Created by the authors from primary data and statistical analysis.
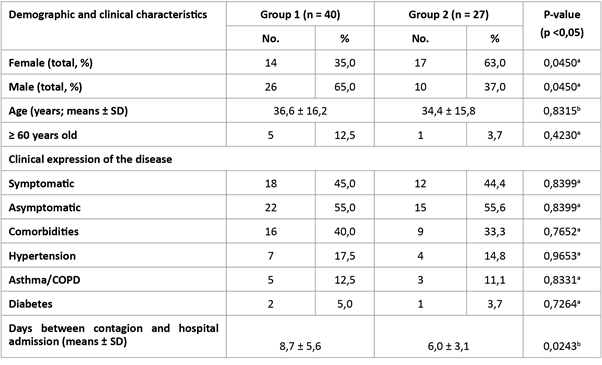
Of the 40 patients included in Group 1, 18 manifested some symptoms related to SARS-CoV-2 infection upon admission and during the hospital stay, and 22 had an asymptomatic infection by the SARS-CoV-2 virus. (Figure 1 A) The most frequent symptoms in this study were the typically expected of a respiratory illness, cough, and fever. (Figure 1 B) However, other symptoms were reported such as nausea, hypogeusia, arthralgia, convulsions, and conjunctivitis, although much less frequently (1 % each).
In the case of the patients in Group 2, 12 had symptoms related to the disease upon admission and during the hospital stay, and 15 were asymptomatic. (Figure 1 C). Nevertheless, the frequency of symptoms was similar to that of the symptomatic patients in Group 1. (Figure 1 D).
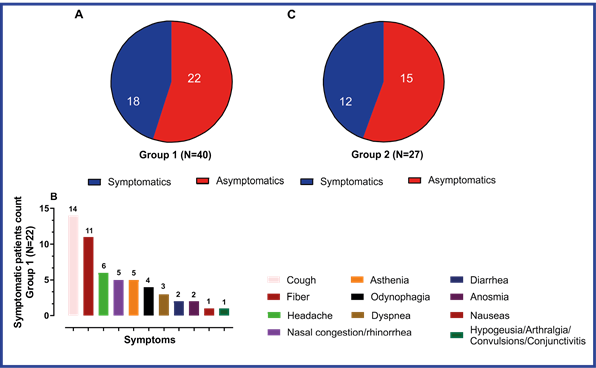
Fig. 1 A: The proportion of symptomatic and asymptomatic patients in Group 1 (IFN+K+C). B: Relation of symptoms and number of subjects by Group 1 (IFN+K+C) symptoms. C: Proportion of symptomatic and asymptomatic patients in Group 2 (K+C). D: Relation of symptoms and number of subjects by Group 1 (K+C) symptoms. Source: Created by the authors from primary data and statistical analysis.
Time to viral clearance in the study group
Group 1 had a significantly shorter time of negativization by RT-PCR than Group 2. By day 9th, 60 % of the patients in Group 1 had become negative. In contrast, 20 % of patients in Group tested negative on the 9th day. (Figure 2 A).
Patients were stratified into symptomatic and asymptomatic and considering p-value is as descriptive, the major difference in time to negativization between groups was observed in symptomatic patients. (Figure 2 B, C) In contrast, within the same group, symptomatic and asymptomatic patients did not show significant differences in time of negativization in Group 1, whereas in Group 2 there were differences. (Figure 2 D, E).
Fig. 2 A: Time to viral clearance between Group 1 and Group 2 patients portrayed by Kaplan-Meier plot and compared with a Log-rank test. B: Percent of negativization of symptomatic patients treated with IFN+K+C vs. K+C. C: Percent of negativization of asymptomatic patients treated with IFN+K+C vs. K+C. D-E: Percent of negativization of symptomatic vs. asymptomatic patients treated with IFN+K+C and K+C. Source: Created by the authors from primary data and statistical analysis.
Inflammatory markers
In Group 1, the paired analysis of the values collected after hospital admission and discharge showed a behavior towards normalization of the neutrophil / lymphocyte ratio (NLR) values. During admission, asymptomatic patients had mean values significantly lower than those of asymptomatic patients. However, the mean values were similar at the hospital discharge. The results of C-reactive protein and Ferritin showed a similar behavior in this group. (Figure 3 A, B, C).
In Group 2 patients, the behavior towards normalization of the NLR values was apparently similar to that of group 1. However, only symptomatic patients significantly reduced the final values vs. the initial ones as opposed to asymptomatic patients. In addition, considering the p-value as descriptive, the significance is lower to that of Group 1. At the time of hospital admission, the mean values of NLR in patients showed significant differences, indicating that asymptomatic patients have lower mean levels. The same behavior was observed at hospital discharge. (Figure 3 D) Similar behavior was obtained for the values of C-reactive protein and Ferritin in this group. (Figure 3 E, F).
The proportion of patients with NLR, C-reactive protein, and Ferritin values above the standard upper limit at the time of hospital admission was similar in the two treatment groups. However, at hospital discharge, Group 1 had a significantly lower proportion of patients with values above the upper limit than the Group 2. (Figure 3 G).
The number of symptoms was positively and significantly related to the values of inflammatory markers (symptoms number vs NLR, Spearman r= 0,5237, P value< 0,0001; symptoms number vs CRP, Spearman r= 0,5042, P value< 0,0001; symptoms number vs Ferritin, Spearman r= 0,4468, P value= 0,0002). As the symptoms increased in numbers in each patient, the vouchers for NLR, C-reactive protein and Ferritin did as well. However, the R-values of correlations were between 0,4 and 0,5.
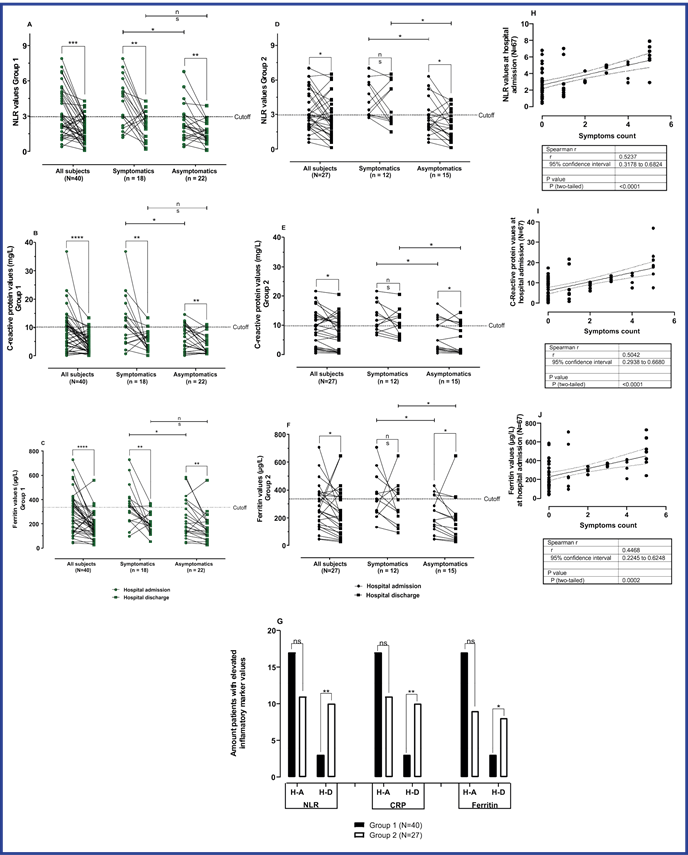
Fig. 3 Paired comparison of values of the neutrophils/lymphocytes ratio (A), C-reactive protein (B), and Ferritin (C) at hospital admission and at hospital discharge of Group 1 and Group 2 (D-F) using Wilcoxon matched-pairs test. The comparison of values of each analyte at hospital admission and hospital discharge between symptomatic and asymptomatic patients using the Mann Whitney test was made.G:Chi-square for proportions comparison between Group 1 and Group 2, considering neutrophils/lymphocytes ratio, C-reactive protein, and Ferritin values at hospital admission and discharge.H-J: Spearman correlation between each inflammatory marker and symptoms count.
SARS-CoV-2 antibodies
Group 1 patients showed a significant decrease in antibody titers 4 months after hospital discharge compared to 2 months. In contrast, significant differences were obtained between the mean values of IgA and IgM antibodies at 4 months compared to 2 months. In the case of IgG, the mean values did not vary significantly despite having shown a significant behavior towards the decrease of antibody titers 4 months after hospital discharge. (Figure 4 A).
In a separate analysis of symptomatic patients of Group 1, the same behavior was observed. (Figure 4 B) However, a significant decrease in IgG values were detected in asymptomatic patients of the same group at 4 months of convalescence. (Figure 4 C).
In Group 2, the decrease in antibody values at 4 months was consistent with what was observed in Group 1. Also, the mean values of IgA and IgM were significantly lower at 4 months compared to the results of 2 months of convalescence. Nevertheless, in this case, the IgG mean values were significantly decreased at 4 months. (Figure 4 D, E, F).
The comparison of mean values of IgA, IgM, and IgG between treatment groups showed that patients treated with IFN+K+C had higher mean values of antibodies than patients treated with K+C 2 and 4 months after hospital discharge. (Figure 4 G, H).
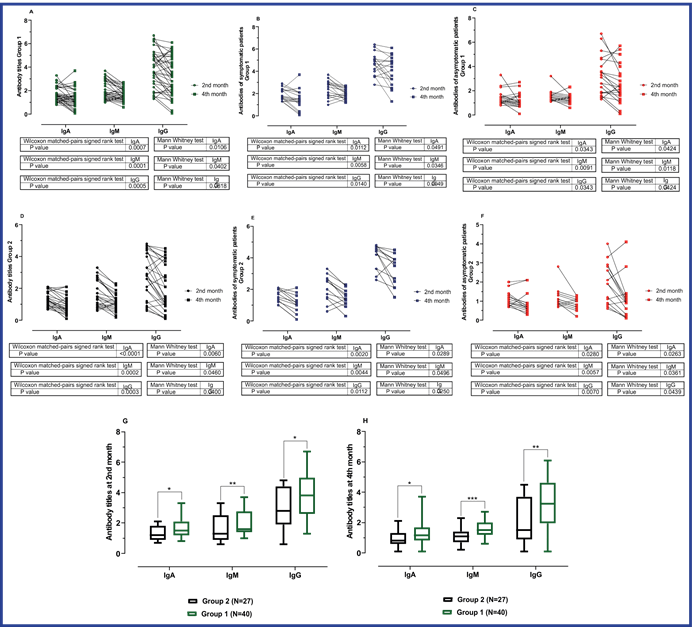
Fig. 4 A-C: Paired and mean comparison of antibody titers of the group treated with IFN+K+C at 2nd and 4th months. D-F: Paired and mean comparison of antibody titers of the group treated with K+C at 2nd and 4th months. G-H: Mean comparison of antibody titers of the group treated with IFN+K+C vs. K+C at 2nd and 4th months. Source: Created by the authors from primary data and statistical analysis.
On the 9th day after starting treatment, Group 1 patients had detectable titers of the significant classes of specific SARS-CoV-2 immunoglobulins (IgA, IgG, and IgM). The mean of antibodies was not significantly different between symptomatic and asymptomatic patients at this time point. (Figure 5 A) However, on the 14th day, symptomatic patients had a significantly higher mean value than asymptomatic patients. (Figure 5 B).
The analysis of paired samples showed a significant increase in IgA, IgM, and IgG levels between the 9th and 14th days in symptomatic patients. (Figure 5 C) However, for asymptomatic patients, a significant increase was only detected for the mean values of IgG titers on the 14th day compared to the 9th day. (Figure 5 D).
The existence of a positive association between antibody titers and the number of symptoms suffered by patients was determined by IgA (Spearman r= 0,4011, P value= 0,0103), IgM (Spearman r= 0,4203, P value= 0,0069), and IgG (Spearman r= 0,5493, P value= 0,0002).
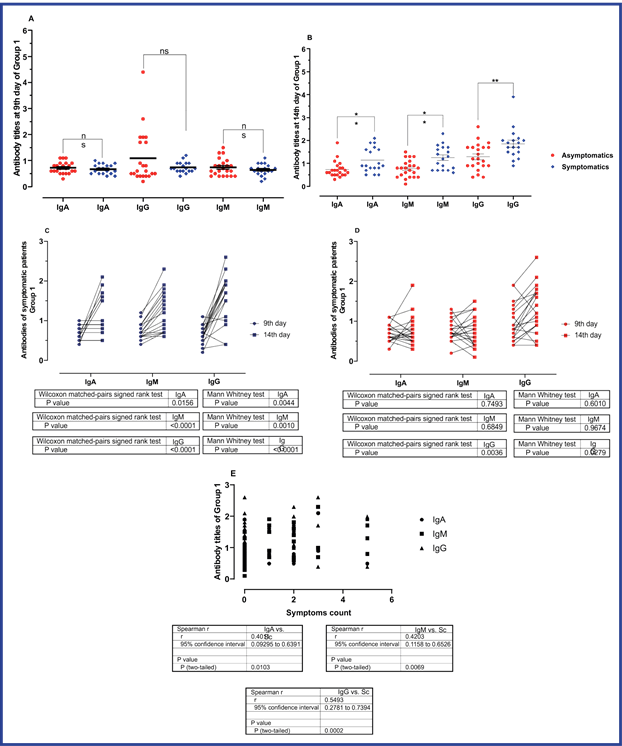
Fig. 5 A: Mean comparison of antibody titers of symptomatic patients vs. asymptomatic patients treated with IFN+K+C at 9th day of hospital admission and B: at 14th day. C-D: Paired and mean comparison of antibody titers of symptomatic and asymptomatic patients treated with IFN+K+C. E: Spearman correlation analysis between the number of symptoms of each patient and antibody titers at 14th day. Source: Created by the authors from primary data and statistical analysis.
Discussion
Several studies have documented cases of patients with a positive diagnosis of SARS-CoV-2 that never presented symptoms (asymptomatic.10,11,12 An asymptomatic infection does not necessarily imply a lower viral load or a lesser probability of transmitting the virus, in fact these patients bear higher viral loads, and consequently are very powerful transmitters of SARS-CoV-2.10,11 The immune systems of these individuals are capable to neutralize the virus more rapidly. This doesn’t mean that asymptomatic patients have a stronger or more durable immune response7,10,13 or are exempt from complications, as demonstrated by typical COVID-19 radiological lung lesions.11,14,15 On the other hand, subjects with symptomatic infection may experience a remarkable variety of symptoms, which may have different intensity levels.10 Patients with symptoms are more likely to develop severe forms of the disease due to failures in host response mechanisms, such as alterations in the interferon pathway.16,17,18
For the treatment, drugs like IFNs, LPV / RTV and chloroquine have been used with different levels of efficacy.19,20,21
Interferons (IFNs) act as direct antiviral protein. They also have the function of inhibiting cell proliferation, acting as immunomodulators, and desensitizing immune response after its activation, in addition to other pleiotropic effects that target relevant components of the pathophysiology of COVID-19 (REF, ACE2, and ISG).16 IFNs have a fundamental contribution in accelerating the elimination of the virus in both symptomatic and asymptomatic patients, shortening the viral clearance time and hospital stay.4,22,23 The absence of IFN, leads to an imbalanced immune response.16,17,18,21,24,25 These elements become more visible in subjects with mutations in the INFs genes, signaling protein pathway, or autoantibodies against IFN, who have a greater risk of developing severe or critical forms of the disease with a worse prognosis.22,26,27,28,29 Therefore, exogenous IFN treatment acts as replacement therapy. This therapy becomes more effective in the early stages of the disease.30
The viral clearance time did not show differences between symptomatic and asymptomatic subjects in Group 1, which could be interpreted as a significant result if it is assumed that asymptomatic patients have a more effective neutering immune response against SARS-CoV-2 virus.13,15 IFN could mediate a faster viral clearance that allows them to have a response rate to viral clearance like that of asymptomatic subjects. However, other therapies such as the LPV / RTV and chloroquine do not show a therapeutic benefit in shortening the time to viral clearance of infected patients21,22 because it did not significantly accelerate clinical improvement, reduced mortality, or decreased hospital stay.16,17
Type I IFNs block IL-17 signaling and affect the biological properties of the neutrophils generating neutropenia, roles strongly associated with SARS-CoV-2 and COVID-19 pathophysiology.16 Considering the role of Type I IFNs in regulatory T cell development and the inverse correlation between regulatory T cell count and disease severity in COVID-19 patients,31 it may be reasonable to consider deregulation of IFN as a highlighted event in the pathogenesis of COVID-19 that warrants IFN-based replacement therapy. The practical benefits of the use of exogenous INF in people infected with SARS-CoV-2 not only lie on its own antiviral and immunomodulatory capacity but in other roles such as its contribution to ACE2 expression.26,32 It has been demonstrated that the use of IFN-α2b for COVID-19 reduces the viral load in a short time,33,34,35,36 which correlated with a reduction in acute inflammatory markers such as NLR,37,38,39,40 C-reactive protein (CRP)16,28,33 and ferritin levels.41,42,43 Also, patients who use IFN in the viremic phase of the disease have a lower risk of developing the severe and critical forms of COVID-19 and dying from it.17,33,34
The virus's seroconversion and neutralization occur between the 5th and 14th day after symptoms in hospitalized patients with COVID-19.43,44,45 Symptomatic subjects in the group treated with IFN+K+C showed a significant increase in specific IgA, IgG, and IgM antibodies on the 14th day compared to the 9th day after initiating treatment. Also, a direct positive relationship was demonstrated to imply the number of symptoms of COVID-19 antibody titers.
Although asymptomatic SARS-CoV-2 infection generates polyfunctional antibodies that neutralize the virus and target infected cells, there are differences with symptomatic subjects in the case of antibody-mediated cellular cytotoxicity, IgA, and IgM titers. These differences lie in the fact that in asymptomatic subjects, their IgA and IgM titers are usually lower and follow different kinetics in favor of IgG,44 which corresponds to the results obtained in this study. Symptomatic subjects in Group 1 showed a significant increase in IgA, IgG, and IgM from the 9th to the 14thday. In contrast, this trend was only crucial for IgG in asymptomatic subjects. This difference may be due to the relationship between the titles and the symptoms and the difference in IgA and IgM kinetics.44,45 Treatment with IFN might have influenced the antibody response of these subjects, enhancing them. Type I IFNs are a bridge between innate and acquired immunity that regulate the activation and functions of various immune cell populations, specifically dendritic cells46 and T cells.47 IFN-α / β directly influences the fate of CD4 (+) and CD8 (+) T cells during the initial phases of antigen recognition. Treatment with IFN enhances the response of memory T cells,47 which is diminished in asymptomatic subjects.48
However, the main limitations of this study were that it was not conceived as a double-blind, controlled clinical trial and the relatively small sample size.

