










 Serviços customizados
Serviços customizados Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkIntroduction
The World Health Organization (WHO) defines anemia as a "disorder in which the number of red blood cells is insufficient to meet the body's needs". Anemia in pregnant women is defined when the hemoglobin (Hb) value in the first trimester is less than 11 g/dL and 10.5 g/L in the second trimester.1 Anemia is particularly worrying in pregnant women due to its deleterious effect on perinatal outcomes2 including perinatal mortality.3
Due to the low atmospheric pressure found at high altitude (HA) which results in a decrease of oxygen in the air causing chronic hypobaric hypoxia, several physiological adaptations take place such as increased erythropoiesis.4 However, some studies reveal that native populations at HA have undergone adaptations that would help the fetus to reduce the physiological effects of the reduced oxygen supply to the uterus.5 On the other hand, several studies have demonstrated the existence of physiological differences between women who live at sea level and those who live at HA, such as late menarche, advanced menopausal age, shorter reproductive period, among others.6 There is also evidence regarding the effects of HA on pregnant women and neonates, such as low birth weight,7 cardiac dysfunction problems;8 preeclampsia and perinatal death.9
The WHO recommends an adjustment of the cut-off point for the determination of anemia in HA populations. This adjustment increases the cut-off value by up to 4 g/dL for women living above 4000 meters above sea level (MASL). Peruvian regulations consider and apply these recommendations;10 however, there is an ongoing debate regarding the suitability of the adjustment. While there is research in favor,11 others are against, due to the discordance between the prevalence of anemia when using this adjustment factor and the data found in field and retrospective studies.12 Also, studies that measured iron status biomarkers show that iron is not affected by altitude, and the adjustment needs to be revised as it overestimates iron deficiency anemia.13 The main objective of the present work was to study hemoglobin levels and characterize anemia in pregnant women at different altitudes in Arequipa region.
Methods
A quantitative, descriptive and retrospective study was conducted with a study population of 35,725 pregnant women aged between 12 and 53 years, who were evaluated in the period from January 2018 to December 2019 in Arequipa region, Peru. Due to the closeness of the Andean Range to the Pacific Ocean, this region located in the Southern Peruvian Highlands has both locations in the above 3500 MASL as well populations living at sea level. The data was provided by the Regional Anemia Registries regional anemia registries.
The variables studied were: age (years), gestational age (weeks), weight (Kg), pre-gestational weight (Kg), place of residence (province), population altitude MASL observed hemoglobin level (g/dL), and adjusted Hb levels (g/dL), which according to the Peruvian Technical Standard "is performed when the child, adolescent, pregnant woman or pregnant woman resides in localities located at altitudes above 1000 meters above sea level". To determine the severity of anemia, the WHO criteria and the Peruvian Technical Guide were both used for observed and adjusted hemoglobin levels according to the geographic altitude of origin. Only data from singleton pregnancies was included in the study.
Adjustment of hemoglobin by altitude (Meters above sea level) as recommended by the WHO: Altitude Under 1000 MASL (0 Adjustment factor (mg/dl), 1000-1500 MASL (-0.2 mg/dl), 1500-2000 MASL (-0.5 mg/dL), 2000-2500 MASL (-0.8 mg/dl), 2500-3000 MASL (-1.3 mg/dl), 3000-3500 MASL (-1.9 mg/dl), 3500-4000 MASL (-2.7 mg/dl) and 4000-4500 MASL (-3.5 mg/dl)
Frequency distribution, as well as ranges and averages, were used to evaluate the quantitative variables. To assess the differences between the study variables was performed using the Chi-square test, with a 95 % confidence interval and Student's t-test. Stata version 14 (StataCorp, CollegeStation, TX, US) was used for data analysis.
Results
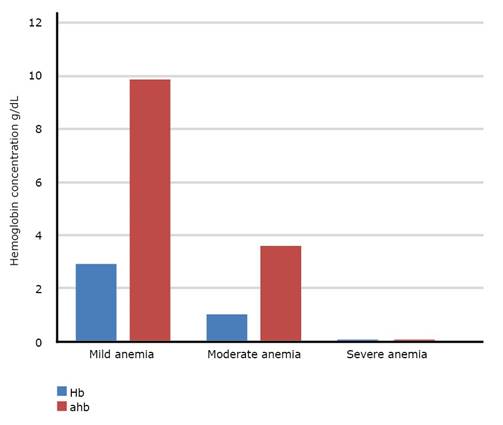
A total of 35,725 pregnant women between 12 to 53 years old from 8 provinces of the region were evaluated. 4,900 pregnant women had anemia (13.71 %). Mothers had an average age of 26.6 ± 6.32 years old, weighted 65.5 ± 9.6 kilograms with an average height of 1.52 ± 5.4 meters. The prevalence of altitude-adjusted anemia was 13.7 %; 9.9 % for mild anemia, 3.6 % for moderate anemia and 0.1 % for severe anemia. Mean gestational age was 27.7 ± 9 weeks. In table 2, we present the distribution of the sample according to altitude and general characteristics of the studied population grouped by anemia status. When the adjustment is not performed, the prevalence of anemia triples. For mild anemia is 3 %, 1 % for moderate anemia and 0.01 % for severe anemia (table and fig. 1).
Table 1 Characteristics of the studied population
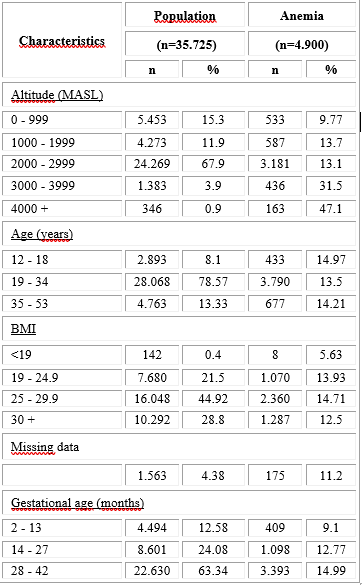
MASL: meters above sea level. BMI: Body mass index. Anemia was defined using altitude adjustment Hb values.
In Figure 2, the behavior of Hb with and without adjustment at different altitudes is shown. As it can be seen, from 2000 MASL onwards, a significant difference between the adjusted and unadjusted values is observed. Adjusted Hb levels decrease below the cut-off point (11 g/dL), constituting mild anemia.
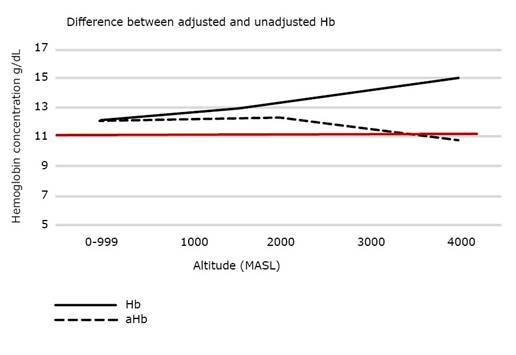
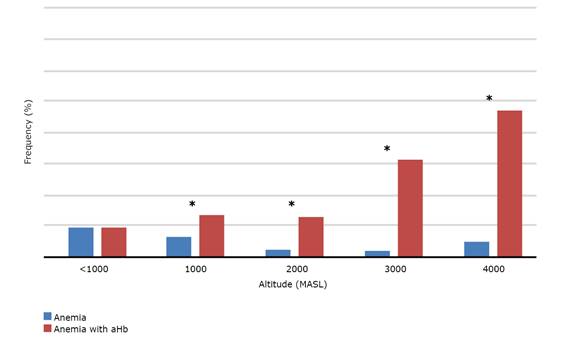
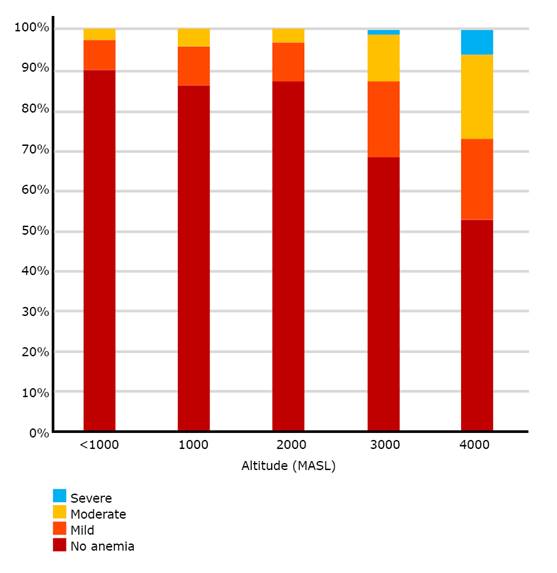
Figure 3 shows the frequency of pregnant women with anemia (Hb <11 g/dL) calculated with and without altitude adjustment. When we use altitude adjusted Hb values, a significant difference is observed in the percentage of pregnant women with anemia, being up to 5 times higher than the frequency observed without adjusting, suggesting an overestimation of the prevalence of anemia at HA. In figure 4, the distribution of the severity of anemia is presented. A visible increase in the percentage of moderate and severe anemia from 3000 MASL onwards is shown.
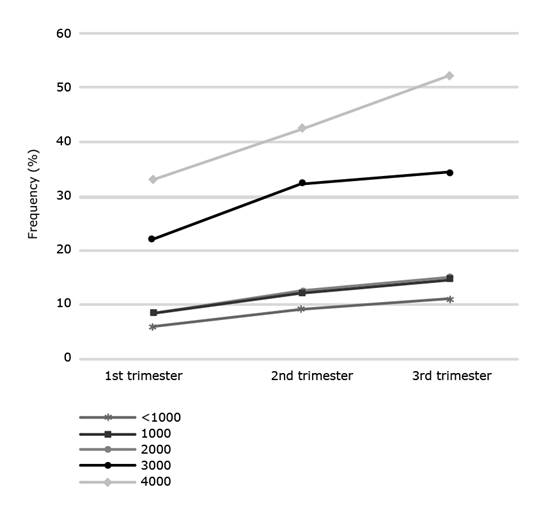
Finally, the frequency of anemia was analyzed by gestational period at each geographic altitude. In the first trimester, the prevalence of anemia was found to be higher than 20 % at 3000 MASL. This value increased by 10 % from the second trimester onwards. The increase in the frequency of anemia in the third trimester does not vary significantly at 3000 MASL. However, an increase of 10 % is observed at over 4000 MASL (fig. 5).
Discussion
The purpose of the present study was to characterize anemia in Arequipa, a region with different altitudes. Anemia prevalence increased with altitude. Overall, the prevalence was 13.7 % with values ranging from 9.77 % to 47.1 % when analyzing cities at sea level and above 4000 MASL. These results differ from the results obtained in the Pakistani Highlands, in which a higher prevalence of anemia was found in pregnant women at low altitudes. However, the difference in sample sizes might be the reason behind this difference. Nevertheless, some results concur with our findings. In preschool children, altitude was one of the main determinants for anemia alongside younger age using data from a nationwide survey.14
Not much research has been done regarding the relationship between age and anemia in pregnant women at HA. In our study, we show that the highest percentage of anemia was found in the group of women between 12-18 years of age. These findings are in contrast to a study performed in Korean women in which the highest prevalence of anemia was found in the 25-29 years’ age group.15 However, another nationwide study in Malaysia failed to determine any statistical difference associated with Hb level and age.16
Another factor to consider is BMI and gestational weight gain; which may be important indicators of possible pregnancy complications such as gestational diabetes. In our study, the mean BMI was 29.79, which is in agreement with reference values for pregnant women.17 In a study conducted in pregnant women at sea level and at high altitude, no significant statistical difference was found between the two groups, although the study concludes that fasting maternal plasma glucose is lower at high altitude than at sea level, which would be associated with greater sensitivity to insulin.18 On the other hand, studies suggest a relationship between BMI and the presence or absence of anemia. A Peruvian study suggest an association between excessive weight gain during gestation especially in underweight and normal weight women, with decreased hemoglobin values in gestation; Nevertheless, in our study, we did not find a significant difference in the prevalence of anemia in normal weight versus overweight pregnant women (p=0.721).
The WHO recommends a correction of the cut-off point for the diagnosis of anemia in HA populations; which increases the cut-off value by up to 4 g/dL for women living above 4000 MASL. Regarding the severity of anemia, it was observed that, after using the correction factor established by the WHO, it increases significantly. These results are in agreement with those obtained in a study carried out in Tibet. The authors conclude that the adjustment factor may have overestimated the prevalence of anemia in pregnant women since most of them did not show clinical signs compatible with anemia.19
In order to evaluate the WHO Hb adjustment factors, we have graphed the expected hemoglobin for each altitude based on our formula: Hb = (.0000002*altitude2) - (.00001 * altitude) + 13.9, where the altitude is in meters.20 It becomes evident that the WHO Hb adjustment factors are adequate, as they fall precisely on the exact curve of the expected Hb values obtained from different high-altitude residences in different populations.
Another study conducted in HA Bolivian pregnant women shows an increase in the prevalence of anemia when using the WHO correction factor, compared to two other approaches made in previous works and an additional one proposed by the authors.21
Another factor related to the WHO recommend adjustment criteria is ethnicity. In a review that studied the relationship between anemia, ethnicity and the accuracy of the adjustment factor for the diagnosis of anemia and severe anemia it was shown that the presence of anemia could be underestimated for people of African ethnicity compared to Caucasians when a single adjustment factor was used.22
Ethnicity is a major variable when it comes to HA adaptation. It has been shown that Tibetan people are highly adapted to environmental hypoxia thus exhibiting decreased Hb levels than the Hans despite living at the same altitude.23 Generational exposure is the factor explaining these difference. Although not as pronounced, Hb differences amongst people from the Southern and Central Andes have been reported. The Andean Southern population are predominantly of Aymaran descent and have lower rates of chronic mountain sickness, a disease triggered by HA maladaptation. However, we are in disagreement with the use of the term maladaptation.24 The Arequipa region is located at the Southern Andes but it also is one of the main destinations for internal migration. As our study relies on registries provided by the Regional Health System that do not generally collect ethnicity information, we could not assess the impact of ethnicity in Hb levels constituting a limitation of our study. As Gassmann et al (2019) argue, individual reference values should be defined for each ethnic group.25
Regarding the relationship between gestational age and anemia, a trend of decreasing hemoglobin levels, and thus increasing anemia, was observed for each trimester for all pregnant women and at all altitudes. A study in pregnant women from Tanzania at altitudes between 1300 and 2300 MASL where anemia is highly prevalent in pregnant women, reported a decrease in Hb levels in the last semester of gestation.26 Similarly, Xing's study in pregnant women in Tibet shows a decrease in hemoglobin concentration as gestation time increases. This phenomenon could be due to physiological changes of life at HA or changes as a result of the gestation period. Hb levels decrease physiologically during pregnancy, due to an increase in blood volume during gestation, this physiological hemodilution occurs in the second and third trimester of pregnancy, so it is essential to determine whether a pregnant woman with Hb levels less than 11g/dL is really anemic or it is a non-pathological hemodilution.27
Anemia is considered a major risk factor in pregnancy since several studies have associated it with low birth weight, preterm birth and other related problems. A meta-analysis of reported anemia in the first trimester was associated with low birthweight.28 As high altitude is, likewise, associated with increased risk of adverse perinatal outcomes, the coupling of environmental hypoxia and anemia might be an important public health problem that is not being properly addressed. There is little information on these phenomena in populations at high altitudes, and the studies conducted on the subject are scarce or have sample size limitations. For instance, a study conducted by Nahum and Stanislaw in 235 pregnant women shows a negative correlation between birthweight and maternal hemoglobin level, which would be related to the effects caused by exposure to high altitudes during pregnancy.29
The strength of our study lies in the sample size and the fact that the analyzed data came from an anemia surveillance program used by the regional government for decision-making. Therefore, it is representative of the Arequipa province, especially as it is reflecting that the geographical complexity impacts severely anemia frequencies. Nevertheless, a major limitation of our study is the lack of measurement of iron-related biomarkers. Surveillance data rely on point of care devices for the measurement of hemoglobin. As we show, altitude greatly impacts anemia rates and there is an ongoing debate regarding the suitability of current diagnostic thresholds, a throughout iron status measurement study should be performed in this population. Also, the database did not assess ethnicity in the population. For a multicultural country such as Peru, the inclusion of this variable should be prioritized in future surveillance programs, especially since it is known to be a major player of high-altitude adaptation.
Anemia continues to be a serious public health problem both in children and in pregnant women in Peru and in the world. It is also associated with multiple environmental, social, economic and cultural factors.30 Anemia is also more prevalent in rural and Andean areas, which are coincidentally located at medium and high altitudes. Several research needs arise such as the effect of ethnicity in HA adaptation, the suitability of the current guidelines to diagnose anemia, the extent to which anemia during pregnancy is pathological or an effect of normal hemodilution.
Despite official statistics showing an improvement in anemia rates in our country, we found an increase in the prevalence of anemia in pregnant women directly proportional to the rise in altitude. Likewise, it was found that Hb levels decrease with the progress of the pregnancy. This could suggest that as the fetus requires more Hb particularly in the last trimester of in-utero development, it is highly probable that the mothers are receiving insufficient iron and B12 vitamin. This has transcendental importance for the optimal development of the fetus. Even though our study did not assess iron status biomarkers to examine the suitability of the current altitude adjusted Hb recommendation, the increase in the prevalence of anemia and its severity using this approach is significant. As several studies suggest there might be an overestimation of anemia using this criterion. Given that the major interventions are provided as a result of these diagnoses, we call for a revision of the current guidelines and an assessment of Hb and iron status reference values and respective adequate therapies for pregnant women in HA populations according to ethnicity.
We conclude that anemia in pregnant women in the Arequipa Region is highly affected by altitude. Prevalence of the condition differs significantly when altitude adjusted, or unadjusted hemoglobin values are used. Adjusting by hemoglobin values results in triple the prevalence of anemia. A throughout revision of the suitability of current guidelines to diagnose and prevent anemia at high altitude is needed.

