










 Serviços customizados
Serviços customizados Espanhol (pdf)
Espanhol (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkIntroduction
Urinary tract infection (UTI) is one of the most frequent diseases in clinical practice considered as the existence of pathogenic microorganisms in the urine due to infection of the urethra, bladder, kidney or prostate; with or without the presence of symptoms, being in both hospitalized and outpatients around the world. 1 Anatomically they are divided into infections of the lower tract (urethritis, cystitis and prostatitis) and upper tract (pyelonephritis and intrarenal abscesses). 2
UTI urinary tract infection ranks second among infectious processes, being the main cause of bacteremia and sepsis in older adults. The treatment is based on the most probable etiology and the expected sensitivity of the uropathogens, described in microbiological maps. 3,4) The microorganisms that are isolated from urine cultures will vary according to the circumstances of the patient and their underlying diseases. The etiology of UTI is modified by factors such as age, diabetes, urinary tract obstruction, or urinary catheterization. Previous exposure to antibiotics and the history of hospitalization will also determine differences in the etiological profile.
More than 95% of UTIs are caused by a single bacterial species. E. coli causes between 75-95% of episodes of acute uncomplicated cystitis. Staphylococcus saprophyticus, Proteus mirabilis, Klebsiella pneumoniae, Streptococcus agalactiae and enterococcus are responsible for the vast majority of the remaining episodes. The uropathogens in the vast majority of the times come from the intestinal flora itself. 5Antibiotics have been one of the greatest contributions for the cure of diseases. The discovery of penicillin by Fleming, in 1529, marked a milestone in the history of medicine. After almost nine decades, we face again an uncertain future, because bacteria have developed adaptation mechanisms against the action of antimicrobials, constituting a public health problem.6
The tendency towards the emergence of resistant strains against several groups of antimicrobials has been driven by the inappropriate use of antimicrobials, self-medication and therapeutic non-compliance. 7 The high prescription of antibiótica is conditioned by their evident efficacy in healing and prevention of multiple infections, 8 however, most of the authors assure by studies that in a large number of patients it is done unnecessarily.
The negative consequences of the increase in bacterial resistance are expressed in terms of morbidity, mortality and health costs derived from medical care that ocul. threaten the sustainability of health systems. As a result of the above, it is considered advisable to develop a set of measures that tend to rationalize the use of antimicrobials, improving their indications and their use, decreasing as far as possible the toxicity and the cost they generate.These measures are nono as antibiotic policy. Tais set of standards soldo be based on updated knowledge about the use of antimicrobials, on the protocols of Good Clinical Practice Guidelines in force in the hospital and on the microbiological data of the center. 3,9,10
The correct and timely use of the microbiological resource provided by the microbiology laboratory allows doctors to know the causative biological agents in the different processes that patients may present, as well as the “in vitro” behavior of the existing antimicrobial resistance, with the objective to adapt the antimicrobial treatment according to the suspected or confirmed germ, sensitivity and available drugs with their cost, toxicity and resistance induction.
In each institution, service or room it is necessary to have identified the main microorganisms that cause infectious processes; as well as its antimicrobial resistance pattern. Activity that demands a constant update, thus becoming a research problem, faced in the study generated by this research report.The study of urinary sepsis is of constant motivation for health professionals related to these patients, in order to improve the quality of care. The microbiological pattern of antimicrobial resistance of the most frequently isolated germs in positive urine cultures was determined in the microbiology laboratory of the provincial teaching hospital Celia Sánchez Manduley.
Methods
A descriptive cross-sectional observational study was carried out, in a universe formed by all the urine cultures made to the patients who went to the microbiology laboratory of the Provincial Teaching Hospital “Celia Sánchez Manduley”, in the province, with the order of bacteriological study of the urine, in the period from January to December 2018. The sample was made up of 2482 urine cultures.
The analysis log books of the Microbiology Laboratory were consulted. The data evaluated were: urine culture positivity, more frequently isolated germs, antimicrobial resistance of isolated microorganisms in general and Escherichia coli in particular, antibiotics that were used in most patients were used for the study: Ciprofloxacin nalidixic acid, tetracycline, cefazolin, ceftazidime, cotrimoxazole, amoxicillin, cefotaxime, azithromycin, gentamicin, nitrofurantoin. Data were processed according to descriptive statistics.
Results
The results of the urine cultures performed are reflected in graph 1. A total of 2482 urine cultures were performed and a positivity of 714 studies was observed, representing 28.76%.
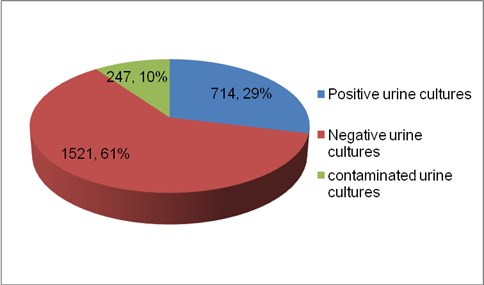
Table 1 show the most frequently isolated germs in urine culture; as illustrated, a higher prevalence of Escherichia coli was obtained for 58.12%, followed by Enterobacter ssp with 26.05%, always taking n as the total positive urine cultures, 714.
Table 1 Germs isolated from urine cultures.
| Germs | No | % |
|---|---|---|
| Escherichia coli | 415 | 58.12 |
| Enterobacterssp | 186 | 26.05 |
| Staphylococcus coagulase positive | 62 | 8.68 |
| Providence | 13 | 1.82 |
| Proteus ssp | 13 | 1.82 |
| Klebsiellassp | 6 | 0.84 |
| Beta hemolytic streptococcus | 6 | 0.84 |
| Citrobacterssp | 6 | 0.84 |
| Enterococcus ssp | 4 | 0.55 |
| Pseudomonas ssp | 3 | 0.42 |
In table 2 total antimicrobial resistances is expressed as a percentage of bacteria isolated in urine cultures.
Table 2 Antimicrobial resistance expressed in total isolated bacteria.
| Antibiotic | Resistance | |
|---|---|---|
| No | % | |
| Nalidixic acid | 315 | 44.11 |
| Cefotaxime | 329 | 46.08 |
| Ciprofloxacin | 319 | 44.67 |
| Cotrimoxazole | 307 | 42.99 |
| Ceftazidime | 306 | 42.85 |
| Amoxicillin | 276 | 38.65 |
| Tetracycline | 259 | 36.27 |
| Cefazolin | 148 | 20.72 |
| Gentamicin | 97 | 13.58 |
| Azithromycin | 89 | 12.46 |
| Nitrofurantoin | 10 | 0.14 |
| Total | 714 | 100 |
The high resistance of isolated germs to different antimicrobials is shown: cefotaxime (46.08%), ciprofloxacin (44.67%), nalidixic acid (44.11%), cotrimoxazole (42.99%) and ceftazidime (42.85%). In the case of Escherichia coli (table 3), the resistance pattern of isolated germs against different antimicrobials is illustrated: ciprofloxacin (52.04%), nalidixic acid (51.80%), cefotaxime (45.54%), amoxicillin (44.81%), and cotrimoxazole (40.04%), with slightly higher values in all cases. It is important to note that the lowest resistance of these microorganisms was for nitrofurantoin, which remained around 1.44%.
Table 3 Antimicrobial resistance to Escherichia coli, present in 415 urine cultures.
| Antibiotic | Resistance | |
|---|---|---|
| No | % | |
| Nalidixic acid | 215 | 51.80 |
| Cefotaxime | 189 | 45.54 |
| Ciprofloxacin | 216 | 52.04 |
| Cotrimoxazole | 167 | 40.24 |
| Ceftazidime | 162 | 39.03 |
| Amoxicillin | 186 | 44.81 |
| Tetracycline | 159 | 38.31 |
| Cefazolin | 57 | 13.73 |
| Gentamicin | 46 | 11.08 |
| Azithromycin | 53 | 12.77 |
| Nitrofurantoin | 6 | 1.44 |
Discussion
Microorganisms can reach the urinary tract by hematogenous or lymphatic dissemination, although there are abundant clinical and experimental data that show that the rise of microorganisms from the urethra is the most frequent pathway produced by UTI, especially by microorganisms of intestinal origin (that is tos say, Escherichia coli and other enterobacteria). 10,11 This offers a logical explanation of the greater frequency of UTI in women than in men and of the increased risk of infection after catheterization or bladder instrumentation.
From the concept of bacterial virulence or pathogenicity in the urinary tract it follows that not all bacterial species are equally capable of causing an infection. The more compromised are the natural defense mechanisms (for example, obstruction or bladder catheterization), the lower the need for virulence of a bacterial strain to cause infection. Bacterial infection is a complex process, in which not only the infectious bacterium has an important role, but also the host. In fact, an important part of the problems arising from the ITU are due to the host's response to it.
Urinary tract infections are the second cause of infectious processes in human pathology, affecting mostly women. From the age of 50, the incidence is equated with the male sex,12Its diagnosis of certainty and adequate treatment, immediately after having taken the sample for bacteriological study, is especially important to prevent kidney damage.The positivity of this study was superior to that reported by Guzman W and colaborados,12,13 in a study conducted in 2017 to the populations of Zumbahua, Colta and Guamote in Ecuador, and found in a similar study in the community of Navarra, 12 both lower than 22%.
The urinary tract is a sterile space. Retrograde ascent of bacteria is the most common mechanism of infection. In women, they can more easily ascend to the urinary tract, due to the relative proximity of the urethral orifice to the anus and to the shorter length of the urethra, congenital urinary tract abnormalities, neurogenic bladder, patients who have a susceptible urothelium, which facilitates increased bacterial colonization, or certain immunodeficiency associated with low levels of IgA and IgG. 11,12
The predisposition to colonization in patients with recurrent UTI, in the absence of anatomical or functional alterations, is related to a greater capacity of adhesion of bacteria, such as Escherichia coli, to the internal prepucial skin, to the perineum, to the vaginal introite and to the urethra; Often, these microorganisms have type P fimbriae, a bacterial adhesion mechanism that makes them more virulent and related to the urothelium. These patients may also have some immunodeficiency associated with low levels of IgA and IgG. 12,13
The literature reviewed allows us to verify that Escherichia coli is still the predominantly isolated uropathogen, followed in a variable order by Proteus mirabilis, Enterococcus faecalis, Klebsiella pneumoniae, Pseudomonas aeruginosa, Enterobacter cloacae, Streptococcus agalactiae, Staphylococcus saprophyticus, Serratia marcescens y Morganella morganii.4,6,14,15
The values reported in this study, regarding the isolates of Escherichia coli, coincide with what is reported by the scientific literature. 4,6,14,15 and the values reported by Sánchez, in the study carried out in the Colombian microbiology laboratory in 2009-2013, where Klebsiella ranked second. 4 When assessing the resistance pattern obtained in this study, it is thought that it could be related to the protocols for the use of antimicrobials for urinary sepsis in recent years.
The resistance of the main uropathogen causing ITU, the Escherichia coli bacteria, to the antibiotics used in the Microbiology Laboratory of the Provincial Teaching Hospital “Celia Sánchez Manduley” in Manzanillo, showed a resistance pattern with values far superior to the results produced by the researches consulted. 4,6,7,12) Inthe study carried out in Quito, enteropathogens showed resistance levels higher than those of this research for cotrimoxazole (56.7%) and nalidixic acid (53.3%). In the last decade there has been a significant increase in resistance from E. coli to ampicillin, first-generation cephalosporins and cotrimoxazole. 5,7,12 In general, more than half of Escherichia coli strains are resistant to ampicillin and amoxacillin, which invalidates these antibiotics for empirical use.
With respect to cotrimoxazole, in our environment the sensitivity is in a range greater than 40% (table 3). This greater resistance is not only observed in vitro, but also has an increased risk of clinical and bacteriological failure in urinary tract infections treated with cotrimoxazole. (13 Escherichia This work also shows a high resistance pattern for second and third generation cephalosporins.
It is important to highlight that literature shows that nitrofurantoin is only recommended for ambulatory oral therapy in low infections, not high infections, due to its low concentration in plasma and renal tissue. 4,8,16,17 Bacteria acquire the ability to resist the action of antibiotics through various mechanisms, such as antigenic variability, modification of the permeability of the inner membrane, extraction of the compound and enzymatic inhibition, as well as by modification of the ribosomal white, or alteration of the composition and content of bacterial wall glycoproteins.
This resistance is transmitted between microorganisms of the same genus and between microorganisms of different genera.4,8 14,15,16 These results coincide with the criteria that justify resistance to an antimicrobial and may be supported by the following criteria: extensive and indiscriminate use of antimicrobials, irrational or inappropriate prescription of antibiotics, tendency to multiresistance, that exhibit the germs associated with in-hospital infections, and the high existence of cross resistance. 15
The knowledge of the prevalence of in vitro resistance patterns of Escherichia coli to some antimicrobials, observed in the present study, allows the doctor to orient himself in his daily practice when starting the empirical treatment (without bacteriological confirmation) of the UTI. The correct diagnosis, as well as the early treatment of these infections, is of the utmost importance, since in addition to beingresolve the signs and symptoms of the acute condition, secondary complications are avoided.

