










Meu SciELO
 Serviços customizados
Serviços customizadosServiços Personalizados
Artigo
 texto em
texto em  Espanhol (pdf)
Espanhol (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkRevista de Ciencias Médicas de Pinar del Río
versão On-line ISSN 1561-3194
Rev Ciencias Médicas vol.27 no.2 Pinar del Río mar.-abr. 2023 Epub 01-Mar-2023
Articles
Multicentric disease of the lower genital tract, challenge to the colposcopist
1University of Medical Sciences of Guantánamo. General Teaching Hospital "Dr. Agostinho Neto". Guantánamo, Cuba.
2 National Institute of Oncology and Radiotherapy Havana, Cuba.
Dear Readers:
The lower genital tract (LGT) in women is constituted by the anatomical structures that include the anoperineal region, vulva, vagina and cervix; it constitutes seat area of premalignant lesions and genital cancer, therefore it occupies special interest in gynecological care. The fact that two or more of these structures are affected is known in the medical literature as multicentric disease, the term being used for the first time in 1960.1
The presence of lesions in the vagina and vulva is of interest to this editorial because of the need to raise awareness among women and men, as well as their sexual partners, about protection during sexual intercourse, due to the risk of infection by the human papillomavirus (HPV). This constitutes the main risk factor for the development of premalignant lesions that require the existence of associated cofactors such as: irresponsible sexual behavior - the number of partners or sexual partners -, infections by trichomonas, Chlamydia trachomatis, smoking and states of immunosuppression for the origin and development of multicentric disease of the lower genital tract.
Baquendo et al.,2) refer in their study to the presence of HPV serotype 16 in 94% of lesions of vaginal intraepithelial neoplasia (VIN), associated to previous history of premalignant lesions of the cervix, in patients with previous hysterectomies and others in climacteric and menopausal stage (Fig. 1).
In this sense, it is necessary to emphasize that high grade squamous intraepithelial lesion (HSIL) is directly related to HPV, hence it is considered a pre-existing condition and therefore the risk of developing cancer of the lower genital tract is much higher; a different fact occurs in low grade lesions, which can evolve directly or disappear depending on the existing balance between persistence and viral clearance, a process that usually occurs in approximately two years.3
Similar situation is presented in the vulva and perineum, its incidence shows an increase, with potential increase in the coming years, at the expense of young women due to HPV infection, an aspect that becomes noticeable in daily clinical practice.
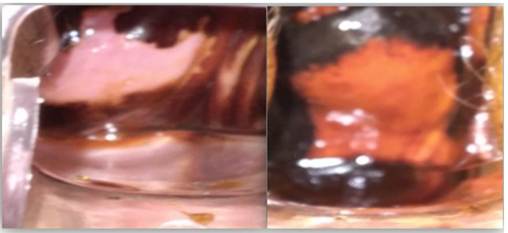
The symptomatology that accompanies these vulvoperineal lesions is highlighted by the presence of pruritus, followed by macular or papular lesions, white, red or pigmented, the appearance of lesions that often go unnoticed and are detected on physical examination, can be localized or multiple (Fig. 2).

Studies by Guijarro Guedes et al. showed in a series studied (N=203) that vulvar intraepithelial neoplasia (VIN) presents as a low grade lesion in 49 %, high grade in 44 % and as cancer in 7 %.4
In this regard, it should be noted that vulvar condylomatosis is a risk factor for the subsequent development of premalignant lesions, as it is the pathway for the possible infection of high-risk oncogenic viruses, which represents a health problem present in women; HPV infection affects between 96 % and 100 % of the cervix and vulva as well as anal intraepithelial neoplasia; this is not the case in male patients, as high-risk HPV infection may remain subclinical or be imperceptible during systematic urological examination in men, at least in a preventive context.
Hence, the prevention program in the GIT pathology and colposcopy consultation includes a thorough examination with 5 % acetic acid in all suspicious lesions during vulvoperineal and vaginal examination. Although identification can sometimes be difficult, most subclinical lesions can be identified.
In this case, care should be personalized in which risk factors and possible co-factors are identified and the details of the lesion (location, extent, borders of the lesion, presence of relief) are specified. In all cases, informed consent should be sought from the patient.
However, it is the treatment and follow-up strategy that constitutes a challenge in care, because although there is consensus on certain aspects such as first-line treatment for single and/or small lesions (surgical excision) and laser as the technique of choice for young women with multifocal lesions. These lesions can be approached with other destructive therapeutic techniques and the local application of pharmaceutical products of an immune stimulating nature, however, it is complex to address the problem of extensive lesions that also converge in three sites (e.g. vulva, vagina and cervix), which may be present in 30 % of multicentric lesions.4
It is a colposcopic challenge to diagnose and establish the treatment and follow-up of women affected by HPV infection, considering the epidemiological criteria, given the fact that the immunological factor is necessarily present for the development of intraepithelial lesions. However, the therapeutic arsenal does not include a systemic treatment strategy to address this growing health problem from the point of view of comprehensive care for women.
This should raise awareness, particularly among primary health care physicians, about the manifest interest in alerting and making an early diagnosis of multicentric lesions of the GIT, either in the evaluation at the level of the medical office or in municipal consultations of neck pathology.
BIBLIOGRAPHICAL REFERENCES
1. Gómez Rueda A, Zúñiga JE. Cáncer multicéntrico del tracto genital bajo. Reva Col. Obst. Ginecol. [Internet]. 1970 [citado 15/02/2023]; 21(4): 349. Disponible en: Disponible en: https://doi.org/10.18597/rcog.1203 1. [ Links ]
2. Baquedano L, Lamarca M, José Y, Rubio P, Ruiz MA. Neoplasia vaginal intraepitelial. Rev. chil. obstet. ginecol. [Internet]. 2013 [citado 15/02/2023]; 78(2):134-138. Disponible en: Disponible en: http://dx.doi.org/10.4067/S0717-75262013000200011 2. . [ Links ]
3. Tatti S, F Leider L, Tinnirello MA, et al. Enfoque Integral de las Patologías relacionadas con el Virus del Papiloma Humano en la era de la vacunación y del tamizaje virológico. Editorial Mêdica Panamericana [Internet]; 2017 [citado 24/3/2023]. Disponible en: Disponible en: https://www.medicapanamericana.com/mx/libro/enfoque-integral-de-las-patologias-relacionadas-con-el-virus-del-papiloma-humano 3. [ Links ]
4. Guijarro Guedes JA, Escamilla Galindo EP, Medina Ramos NF, Santana Mateos Y, Martín M. Revisión de la patología multicéntrica del tracto genital inferior. AEPCC XXXIV Congreso[Internet]; 2021 [citado 15/02/2023]. Disponible en: Disponible en: https://www.aepcc.org/congreso2021/formulario-comunicaciones/posters/e7103a19b5da5221dae30d9d4234fa82.pdf 4. [ Links ]
Received: March 15, 2023; Accepted: March 26, 2023

