










 Servicios personalizados
Servicios personalizados Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
The burden of oral diseases and chronic conditions that result from it is high worldwide.1 World Health Organization (WHO) mentions that between 60 % and 90 % of schoolchildren have carious lesions.2 Inadequate oral health has consequences that alter the student's quality of life.3
Education and health are fundamental rights and are closely related, an adequate education will allow developing skills, values and attitudes for students to have a healthy life. On the other hand, health problems cause children to stay away from school for a long time. In other cases, children have to temporarily interrupt their education to care for sick parents or siblings.4,5
Currently, chronic diseases are on the rise many of which are attributed to people's lifestyles, these behaviors being acquired mostly in childhood and adolescence hence the need to promote healthy schools that allow the acquisition of personal skills and social factors that lead to the creation of positive values and attitudes towards health.6,7
The Ministry of Health of Peru (MINSA) through the health promotion program in educational institutions, it strengthens health promotion through the joint effort of schoolchildren, teachers, parents and the educational community in order to promote healthy behaviors.8 Oral health in Peru has improved in recent years, but there are still gaps in the provision of services between the rural and urban population, within which we find the lack of infrastructure and equipment, poor organization and management of health facilities of the first level of attention, underutilization of the existing public offer, low or no human resources and poorly paid.9,10
The Pan American Health Organization (PAHO) positions Peru as one of the countries with the highest prevalence of dental caries in the Americas region, according to the 2002 study by the Oral Health Strategy of the Ministry of Health of Peru, the prevalence of dental caries and periodontopathies in schoolchildren aged 6 to 12 years is 90 % and 85 % respectively.11
The objective of the study was to determine socioeconomic factors in relation to oral health in students from a rural Peruvian area.
Methods
Design of observational, descriptive cross-sectional study. The sample consisted of 604 schoolchildren of both sexes, belonging to two schools (IE Institución Educativa in Spanish - IE Andres Bello and IE Nuestra Señora de las Mercedes), from the Pilcomayo district, Huancayo province, Junín department, Peru, during the months of October to November 2017.
To determine the prevalence was established by the number of cases of dental caries,12 the experience of dental caries was calculated using the DMFT index,13 referring to the degree of severity the dental caries significance index (SIC)14) was used. Oral hygiene condition was estimated using the Simplified Oral Hygiene Index (OHI-S),15 the clinical consequences of untreated caries were evaluated by the PUFA index (arithmetic sum of dental pieces with pulp (P) involvement, ulceration (U), fistula (F) and tooth abscess (A).16
The socioeconomic factors were evaluated through a survey directed towards the parents, the variables studied were: education of the father and education of the mother (educational level concluded by the father / mother who was living with the child), occupation (main activity of the head of the household), family responsibility (person in charge of family support) and family burden (number of economically dependent children living in the home).
The instruments were validated in a pilot study with a group of schoolchildren with similar characteristics, making the necessary corrections, for the collection of data a dental clinical record was prepared. The inclusion criteria were: belonging to the selected educational institutions, signed informed consent and assent, the exclusion criteria were: presence of any systemic disease that prevents the evaluation of the school, for the collection the indications of the WHO were followed.17
Calibration by examiners
The two evaluators were subjected to calibration and concordance tests, and the results were submitted to the Cohen Kappa index to establish the agreement between the observers, obtaining the value 0.90 (p < 0.05).
Statistical analysis
The data were analyzed in the Microsoft Excel program and subsequently the statistical quantification was performed using the statistical package STATA 14, for the descriptive analysis we obtained percentages and frequency measurements, average scores and standard deviations of the variables. The relationship of each of the socioeconomic factors with the experience of dental caries was evaluated by the simple binary logistic regression tests.
Ethics approval
The present study complies with the ethical principles of the Helsinki declaration, it also had the approval of an ethics committee, schoolchildren were previously consulted about their willingness to participate in the investigation by signing the agreement in schoolchildren under 12 years of age and informed consent from their parents, explaining what it was and the possible benefit it would bring since the results obtained would be shared with the parents to take actions regarding the oral health of their children.
Results
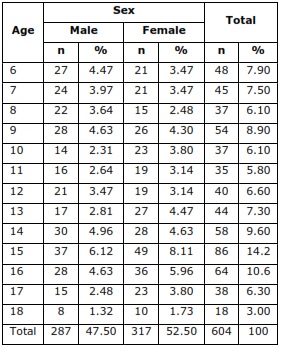
604 students were included, the average age was 12.07 years (SD = 3.59). The sample distribution consisted of 317 women (52.50 %) and 287 men (47.50 %) (Table 1).
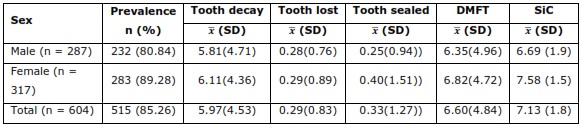
A prevalence of dental caries of 80.84 % and 89.28 % was found in male and female students respectively, the experience of dental caries was high (6.60) according to the WHO criteria and a severity of dental caries (7.13) (Table 2).
Regarding the clinical consequences of untreated caries, there was a higher prevalence in females 205 (33.94 %) compared to males 168 (27.81 %), pulp involvement was the most frequent (41.71 %) of those that presented clinical consequences (Table 3).

Regarding the oral hygiene condition, the majority presented a regular oral hygiene condition 350 (57.9 %), followed by the bad oral condition 174 (28.8 %) and the good condition 80 (13.2 %) (Fig. 1).
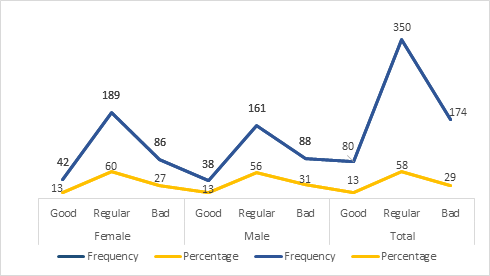
Fig. 1 - Oral Hygiene condition in students of a rural Peruvian population
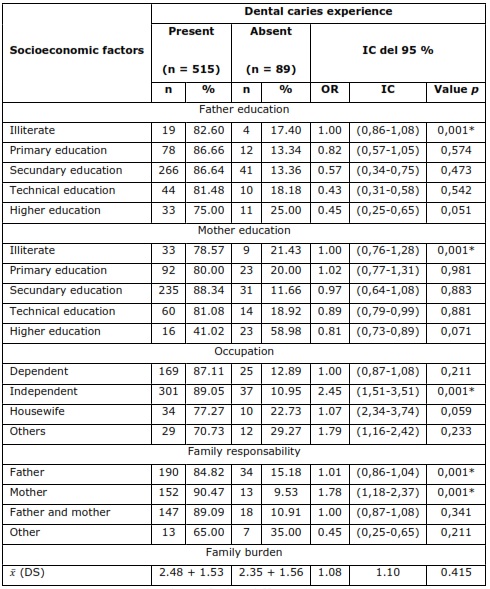
In relation to socioeconomic factors, the degree of illiterate instruction in both the father and the mother and the family responsibility of the parents showed statistically significant association with the experience of dental caries (EDC), independent occupation is a risk factor (p = 0.001) for EDC, observing that children whose parents work independently are 2.45 times more likely to have HCD than those whose parents work dependently (Table 4).
Discussion
Inadequate oral health affects the integral development of schoolchildren, which increases the risk of absenteeism and school delay even more in students of rural origin, the study shows a high prevalence of dental caries being higher than reported by Farooqi FA et al. (73 %)18) in schoolchildren from a rural community in India, García R et al. (25.91 %)19 in schoolchildren in rural communities of Sinaloa-Mexico, San Martin E et al. (20.2 %)20 in schoolchildren from the rural community of Ayangue-Ecuador, Akinyamoju CA et al. (12.2 %)21 in schoolchildren in rural communities in south-western Nigeria and below Aquino C et al. (95.6 % ) 22) in schoolchildren from a rural Peruvian community. The etiology of dental caries is multifactorial, within which social determinants such as socioeconomic status may increase the risk of developing carious lesions.23
In relation to the experience of dental caries, this was greater than reported by Aquino C et al. (5.79),22Ferrazzano GF (1.17),24Kumar S et al. (4.82),25 in addition the study evidenced the small amount of sealed teeth, this is due to the lack of access to health services.
More than half of the students from 6 to 18 years of age had clinical consequences of untreated caries, being greater than that reported by Carrasco-Loyola M et al. (25.71 %),26Narang et al. (22 %)27 and less than reported by Mota-Veloso I et al. (64.6 %),28) the main component was the pulp commitment contributing with more than 67 % of the PUFA index, which can trigger the partial or total infection of the dental pulp (pulpitis) and in more extreme cases the dental loss leading to a greater economic expense of the parents and more time for the rehabilitation of the schoolchild, the high presence of lesions associated with untreated dental caries exemplifies the lack and poor distribution of human resources and inputs in Peruvian rural areas.29
Regarding the oral hygiene condition, it was mostly regular, which is consistent with Barros VA et al., 30Freitas L et al,31 regarding sex, showed that women had better oral health according to Akinyamoju CA et al.,21 This may be because women are more concerned about their oral health as opposed to men, according to the study by Furuta M et al.,32) Women had almost twice as many dental check-ups in the year as opposed to men. In addition, they scheduled their appointments according to the treatment recommended in these check-ups and have better health indicators. 32
That is why the teaching of an adequate dental brushing technique in educational institutions, this would allow maintaining adequate oral hygiene for healthy students and improve the oral condition in what already have gingival inflammation.33
The study showed that students of parents who had a lower level of instruction had more carious lesions, which is consistent with Chaffee BW et al.,34 the educational level of parents positively influences the teaching-learning process of their children on the care of their oral health.35
Regarding family responsibility, the fact that parents work on the oral health of their children, which differs with Mattos M,36) Gaeta M et al.,37 this may be due to the time they dedicate to work, which limits their interaction with their children about oral health care.
Regarding the work condition, the independent one showed a relationship with the experience of dental caries, the progressive incorporation of women into work activity, means that the education of their children is increasingly focused on educational institutions, so that promotion of programs for the promotion and prevention of oral diseases are a priority even more for students of rural origin. 38
In conclusions, the level of illiterate instruction, family responsibility and self-employed parents showed a statistically significant association with the dental caries experience of a Peruvian rural area.

