Servicios personalizados
Servicios personalizados Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Empathy in health care is defined as a cognitive and behavioral attribute that implies the ability to understand the patients´ experiences and feelings regarding their health - disease process.1,2 Several authors show that the presence of empathy allows the development of advantages for the patient such as: a) improving satisfaction, b) increasing complacency, c) establishing better therapeutic relationships with the health professional; and also advantages for the health professional such as: a) improving ability to collect the medical history, b) improving performance of physical examination, c) improving skills for diagnosis and treatment.3,4 Generally, the population assumes that health professionals develop an empathic attitude towards the patient; however, in Peru, the reality is that many patients complain about the treatment they receive from some health professionals, which makes us consider how empathy is formed from the pre-professional training period.
Due to all this, we consider the importance of evaluating this aspect in undergraduate students in order to investigate the level of empathy according to the results obtained; and to propose strategies for future curricula. In the present study, we used the Jefferson Scale of Empathy (JSE), which was based on three factors: a) compassionate care, b) taking perspective and c) putting yourself in the other's shoes.3 These three factors cannot be considered as independent ones. To date there are no studies that measure empathy in the training of professionals in Obstetrics; therefore, the objective of this study is to measure the levels of empathy in Obstetrics Students of the Norbert Wiener University, Peru.
Material and Methods
The present work is descriptive, exploratory and cross-sectional; governed from the bioethical point of view by the Helsinki norms (1964, 2013).
The population consists of first-year to fifth-year students of the Norbert Wiener University of Lima (Peru) (n = 219, 60,33 % of the population: N = 363).
The following stratifications were found in the different academic years: First: 59; Second: 43; Third: 37; Fourth: 49 and Fifth: 31. In the Gender factor, the sample composition was as follows: female = 213 and male = 6. Data collection was performed during May, 2016.
The exclusion criteria were: absence to classes at the time of application of the instrument or refusing to respond to the mentioned instrument.
Participants were applied the Jefferson Scale of Empathy (JSE), Spanish version for medical students (version S) (adapted for nursing students), validated in Chile and Peru3,4 and adapted for obstetrics students. The application was anonymous and confidential and it was performed through a neutral operator.
Before being applied, the JSE was submitted to expert judgment (three relevant physicians of the field of medicine, gynecology and obstetrics), in order to verify the cultural and content validity.5 The students' understanding of the culturally adapted scale was performed through a pilot test. Data collection was made by a neutral operator. This operator was previously instructed in the general characteristics of this instrument and the objective of this investigation. This work was limited to the application of the instrument at the time the students were in class or in the clinical practice, with the authorization of the teacher in charge at the time of the visit. The operator could explain doubts that the students could express at the time the student delivered the answered instrument, check that each and every one of the questions was correctly answered and whether the informed consent was signed or not.
Data were submitted to normality tests (Kolmogorov-Smirnov test and Shapiro-Wilk test, according to sample size) and to equality of variance (Levene). The internal reliability of the data was estimated using the general Cronbach's alpha and the values of this statistician as each of the elements (questions), interclass correlation coefficient, Hotelling's T2, and Tukey non-additive test; estimating the means, and standard deviation. A bi-factorial analysis of variance (ANOVA), model III, was applied in order to find differences in means among the academic years, the genders and the interaction of these two factors and an ANOVA of simple entry to compare means of empathy in each component of the female gender.
The data were described by simple arithmetic and box graphs, and processed by using the SPSS 20,0® statistical program. The total growth potential (TGP) was considered as the quotient between two magnitudes: a) the effective difference between the observed scores of fifth year students minus the first year students' score (D1) with respect to b) the possible difference between the highest value of empathy allowed by the instrument (140) with respect to the effective value of the empathy of first-year students (D2): TGP = D1 / D2. The TGP is an indicator that shows the degree of progress of empathy levels that are possible to observe in cross-sectional studies; it is more accurate in longitudinal studies. The significance level used was α ≤ 0,05 and β <0,20 in all cases.
Results
The Kolmogorov-Smirnov and Levene tests were not significant (p> 0,05), therefore the data were distributed in a normal way with equal variances. Cronbach's alpha values were satisfactory (untyped = 0,765 and typified = 0,785), from which it is was inferred that the data have internal reliability. The value of the total Cronbach's alpha, if an element was removed, fluctuated between the values [0,733; 0,767]; it is inferred that the test maintains a high reliability irrespective of whether or not one of them is eliminated in estimation statistics.
The test associated with the interclass coefficient was 0,851 (F = 6,59; p = 0,005); it was highly significant; the result was consistent with the reliability indicators, Hotelling's T2 test (F = 51,2) and Tukey's non-additive (F = 13,6) were highly significant (p <0,005). In the first case, it is inferred that the means of the questions are different from each other, which shows that not all questions contribute equally to the global mean of the questions (mean = 5,3) and, in the second case, it is inferred that it is necessary to increase the power of the tests to obtain the additive character of the data.
The results of the estimation of means, standard deviation and sample size for each level of the two factors studied are shown in Table 1 and figure.
Table 1 Results of the estimation of means and standard deviation of each academic year and in each of the genres studied.
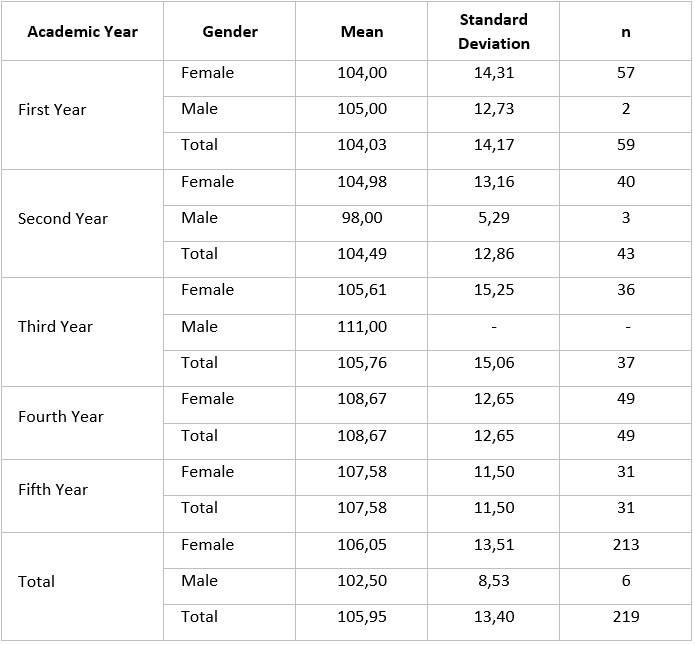
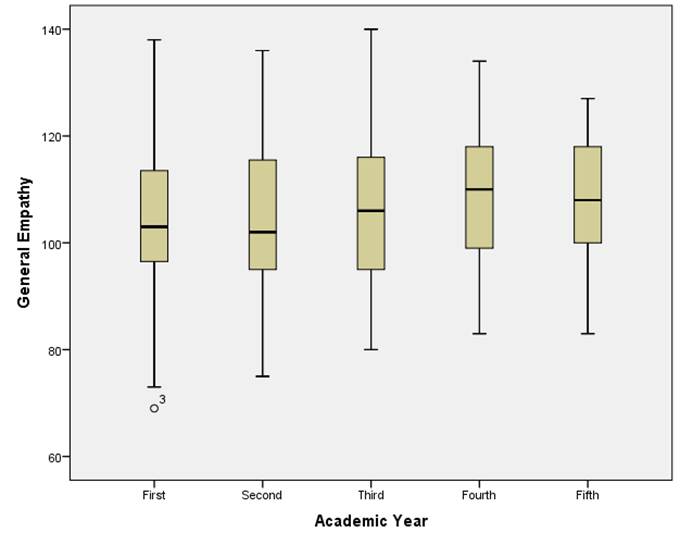
Fig Results of means and standard deviations in the levels of the factor Academic Year in box charts (including atypical data).
The results of factorial ANOVA were not significant in any of the factors studied (p> 0,05), The eta square values were 0,019, 0,001 and 0,004, respectively for both factors and their interaction; and the power was 0,316, 0,05 and 0,112, respectively, which is shown in table 2.
Table 2 Results of comparison between levels of the factors: academic year, gender and interaction between the levels of both factors studied.
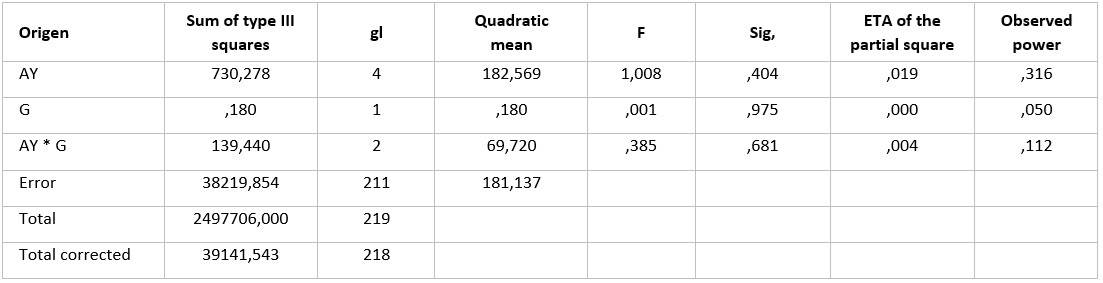
AY=Academic Year; G=Gender
From these results, it can be inferred that it is necessary to increase the size of the sample to reach the value of the accepted power (0,80). The adjusted R-square value was 0,009, which means that the factors studied explain only 0,9 % of all variation in empathy. The results of the estimation of the means of the different academic years in each of the three components of empathy: "Compassionate Care", "Taking Perspective" and "Put Yourself in the Other’s Shoes" are shown in Table 3. The comparison of means among these academic years were not significant in any of the studied components (P=228, p=0,19, p=0,55, respectively).

However, if we consider that the growth potential for first-year students was 35,97 (140-104,03); then, the difference between the empathy of the fifth and the first-year students (107,58-104,03) was 3,55 points; that is, only 10,13 % of a total growth potential for empathy.
If we consider that the growth potential of first-year students was 15,46 (49-33,54) in the component of “Compassionate Care”, then the difference between the empathy of the fifth and first year students (36,45-33,54) was 2,91 points; that is, 18,82 % of the total growth potential for this component. In relation to the “Taking Perspective” on Empathy, as in the analysis of the previous component, the potential growth of empathy in this component is 10,95 points; therefore, the difference between the fifth year and the first year was 0,47; as a consequence, the growth potential in this component was 4,3 %. It is observed in “Put yourself in the other's shoes” on Empathy, that the potential growth of this component of empathy was 9,6 (21-11,4), the difference between the fifth and first year was 0,47 (59,52-59,05); therefore, the real growth was 2,19 %.
Discussion
In the literature reviewed, there is no established cut-off point to clearly determine the level of empathy for the instrument used, as in some cases authors refer to a good level of empathy in values close to a maximum score 140.4,6,7,8,9,10,11,12,13,14,15 This constitutes an objective limitation for a possible classification in subjects, for example, in high, medium or low levels of empathy and a limitation to be able to establish comparisons between different populations of students of the same discipline or different disciplines. However, the absence of cut-off points at the moment does not invalidate the importance of measuring empathy, since this measurement itself is the necessary and sufficient reference to know if certain interventions are able to raise empathy levels.
Only one article that uses the empathy levels classified as high, medium and low scales was found,16 but this criterion was not taken into account for the present study due to the lack of validity and reliability of this concept. The analyzed values could not be compared with obstetrics students from other universities in Latin America because studies of this type carried out in the scientific literature with the same instrument and applied to these same students were not found; most of them were studies applied to dental students, followed by nursing and medical students.
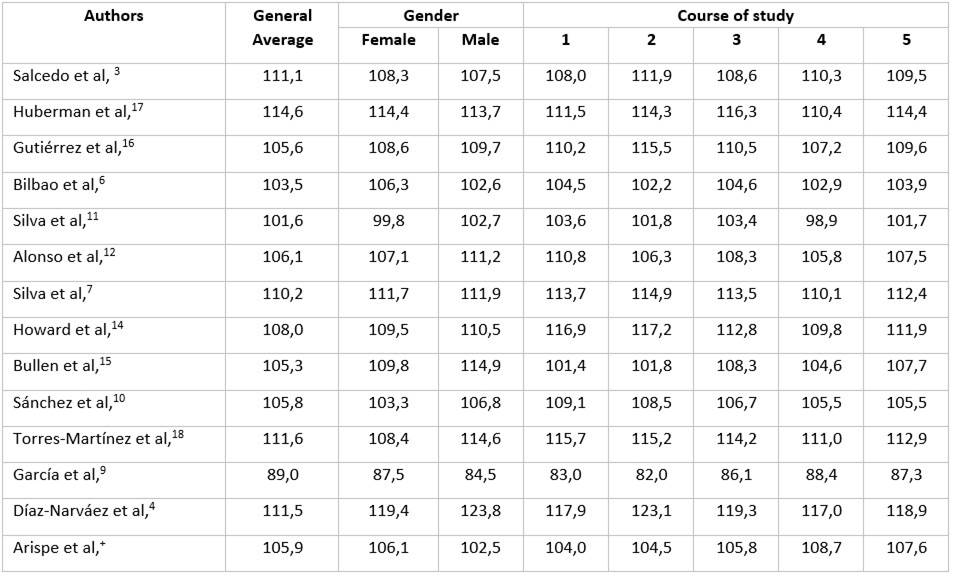
The results found in the present study of empathy levels (105,95) are relatively consistent with those found by other authors. (Appendix).
The present study shows that there is an increase in the empathy score, only in absolute values (not statistically), per year of study. These results are consistent with those found in other studies.7,8,9,10 This finding does not agree with Hojat et al.1,2 who describe that empathy increases until the third year and then decreases (a process called empathic erosion). It has been observed that there is variability in the behavior of means of empathy as the years of study pass. Such variability manifests itself from a sustained ascent from the first to the fifth year until a decline of the same type in these years of study.3,4,6,12,13,14,15,16,17,18 In general, there is a variability in relation to the empathic response of the students in all the factors studied.3,19,20,21,22,23,24,25,26,27
One of the factors that could have influenced the absence of statistical differences between the years and the low potential growth observed in the students examined is that the current curriculum is not sufficiently well constructed and would not have the potential to further develop the empathy, which requires significant modifications to achieve a sustained increase in empathy and its components as the academic year or course increases.
In other words, the main scope of this work is that it allows to estimate a measure of empathy to have a notion of the point of empathic development in which a population of students are. Such measurement constitutes the only empirical basis that allows to elaborate an integral curriculum intervention.
Some aspects that should be contained in the intervention could be: a) development of social skills and emotional intelligence in the curriculum since the first years of training;28,29 b) implementation of extracurricular workshops that favor the development of empathy; c) incorporation of the greatest possible number of hours of practice in those subjects that allow greater direct contact between students and patients, with emphasis on the mother-father-son trinomial, especially in the area of sexual and reproductive health from the first years of the studies; d) fully incorporation of the biopsychosocial approach in all subjects in a longitudinal manner; e) establishment of active teaching-learning methods under the conception of the aforementioned paradigm.
As a consequence, the study of the measurement of empathy in students constitutes a necessary and indispensable step for an empathic diagnosis and a responsible intervention to raise empathy levels.30,31) The relevance of this study is that it is empirically proven that the process of empathic decline in empathy itself and its components is not met. The need and obligation of the institutions to raise levels of empathy to develop training for professionals that take care of patients in a humanized way arises.