










My SciELO
 Custom services
Custom servicesServices on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkRevista Cubana de Estomatología
Print version ISSN 0034-7507
Rev Cubana Estomatol vol.49 no.4 Ciudad de La Habana Oct.-Dec. 2012
PRESENTACIÓN DE CASO
Lymphoepithelial cyst in the palatoglossus arch
Quiste linfoepitelial en el arco palatogloso
Evanice Maria Marçal Vieira,I Vinícius Canavarros Palma,I Tereza Aparecida Delle Vedove Semenoff,I Andreza Maria Fábio Aranha,I Flares Baratto-Filho,II Álvaro Henrique BorgesI
I University of Cuiabá, Cuiabá, Mato Grosso, Brazil.
II University of Curitiba, Paraná, Brazil.
ABSTRACT
The objective of this study was to describe a case of a lymphoepithelial cyst in the palatoglossus arch. A 16-years-old black man said that he was observed a lesion in his mouth. On the physical exam, a pedicled, consistent, smooth surface 1.5 x 1 cm lesion, similar in color to the adjacent mucosa, was found. The lesion was surgically removed and the microscopic exam showed mucosal fragments with pedicled lesion; the cystic cavity sometimes lined with pseudostratified cylindrical epithelium and others with stratified squamous flat interface of the epithelium. Around the cyst, a
well-delimited mass of lymphoid tissue, presenting lymphoid follicles, was also seen. Lymphoepithelial cyst has clinical characteristics similar to those of others lesions that occur in the oral cavity. The diagnosis should be based on conservative biopsy, with total removal of lesion.
Key words: pathology, oral pathology, cyst, lymphoepithelial cyst.
RESUMEN
El objetivo de este estudio fue describir un caso clínico de quiste linfoepitelial en el arco palatoglosso. Paciente de 16 años de edad, sexo masculino, raza negra, que durante la anamnesis relató que observó una lesión en la boca. Al examen físico se observó una lesión pediculada, de consistencia firme, superficie lisa, de 1,5 x 1,0 cm de tamaño, con color similar al de la mucosa adyacente. La lesión fue removida quirúrgicamente y el examen microscópico mostró fragmentos de mucosa con lesión pediculada, la cavidad del quiste a veces revestida por epitelio cilíndrico pseudoestratificado y otras veces por la interfase plana del epitelio escamosa estratificado. Alrededor del quiste, una masa bien delimitada de tejido linfoide con presencia de folículos linfoides. El quiste linfoepitelial tiene las mismas características clínicas de otras lesiones que ocurren en la cavidad oral, el diagnóstico debe ser realizado por biopsia, de manera conservadora, con eliminación total de la lesión.
Palabras clave: patología, patología oral, quiste, quiste linfoepitelial.
INTRODUCTION
Lymphoepithelial cyst, also called branquial cyst, is a lesion in the oral cavity with rare incidence.1-6 Histologically, it consists in a cystic cavity usually coated by stratified squamous epithelium, lined by a well-defined mass of lymphoid tissue, organized by the presence of many follicles and typical germinative centers.1,7 The stratified squamous epithelium is thin, rectified, without epithelial crests, and it is usually parakeratinized.2,3 The cystic lumem often contains desquamated epithelial cells, lymphocytes and an amorphous eosinophilic material.1-3
Although the lesion pathogenesis is not clear, some authors have suggested that the developmental lesion derived from the remaining of the second branquial arch, while others have postulated the relation to ectopic focus of mucosal epithelium or salivary glands which was trapped in lymphoid tissue and after proliferated, forming the cysts.7,8 Others authors have reported that the epithelium of tonsillar crypts can be obstructed and form cysts involved by lymphoid tissue, surrounding it.1,2,7 Clinically, the lymphoepithelial cist is described as asymptomatic submucosal mass, mobile, yellow, present by months or years, and a variable size from milimeters to 1.5 centimeters.2,6,7 In mouth, its occurrence is common in mouth floors and tongue, in ventral or postero-lateral portions.4,6,9 The greater prevalence of this lesion occurs in female gender, in rate over to 2:14, and age between 15 to 65 years old.4-7
The lymphoepithelial cysts are benign, successfully treated by surgical excision. Relapses are rare and they can be resulted by the residual remaining left when the lesion was simply aspirated or drained.2,7,9,10 The aim of this study was to report a clinical case of lymphoepithelial cyst with rare occurence in the palatoglossus arch.
CASE REPORT
A 16-years-old black man, came to the Semiology Clinic at Dental School of the University of Cuiabá, Cuiabá-MT, Brazil, with chief complaint of “small ball inside the mouth”. During the anamnesis, related that he ever observed this lesion, but only the last months he felt worried about the possibility that could be something with malignat characteristics. The lesion showed a characteristic pedicle, firm consistency, smooth surface, similar in color to the adjacent mucosa and measuring 1,5 x 1,0 cm (Fig. 1). Because of the clinical characteristics and localization, the diagnostic hypotheses included fibroma, hyperplastic lymphoid aggregate and lymphoepithelial cyst.

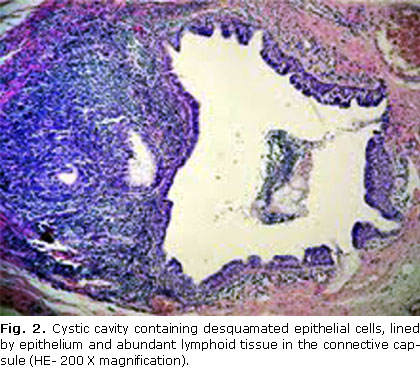
The treatment administered in the present case was surgical. The collected material was sent to be analysed in the Surgical Pathology Laboratory of the University of Cuiabá. The microscopic exam showed fragments of the mucosa, presenting in the lamina propria and subepithelial region. The cystic cavity was sometimes lined by pseudostratified cylindrical epithelium and others by stratified squamous flat interface (Fig.2). Around the cyst, a well-delimited mass of lymphoid tissue, presenting discrete lymphoid follicles organized with many germinative centers, distributed in an abundant manner, in one of the faces of the lesion (Fig. 3). These characteristics are compatible to oral lymphoepithelial cyst. The two-year follow up evolved favorably, and a relapse was not observed.

DISCUSSION
Considering the clinical aspects (pedicled form of the lesion, similar color to the adjacent mucosa and firm consistency), at first moment, diagnostic hypothesis of fibroma was considered. In the literature, there are reports of differential diagnostic with lipoma, when the staining is clearer and soft consistency.2,10 Depending the localization, it should be differentiated by the mucocele.1,3,5,9 About 50 to 80% of the cases of lymphoepithelial cysts ocurr in the bucal cavity floor,1,4,6 followed by ventral and posterior surfaces of the tongue.2,4,7 In this case report, the lesion occured in the palatoglossus arch, with rare frequence (4 to 5 %), such as in soft palate, vestibular region of the mandibular mucosa and retromolar region.4,7
The histological aspects showed cyst lined by pseudostratified or stratified squamous epithelium. Small focus of lymphocytic exocytosis and epithelial cells destruction were observed in the area of the stratified paviment epithelium. The cyst was not regularly surrounded by well-delimited and organized lymphoid tissue, presenting several follicles, some with evident germinative centers. The lymphoid tissue was abundant in the face of the cyst in contact with the squamous epithelium, and scarce in the pseudostratified cylindrical epithelium. The lymphoepithelial cyst is usually lined by stratified squamous epithelium, with desquamated epithelial cells to the cyst lumen.1,2,6,7 However, several authors reported coating by cylindrical epithelium, ciliate or not, sometimes with mucin cells, in monolayers or pseudostratified, and even the occurrence of small areas without epithelial lining.1,6 The main characteristic is related to the presence of the lymphoid tissue in the cyst wall1,2,6,7 with lymphoid follicles formation and germinative centers.2 The situation of lymphoid tissue abundance in one portion of the cyst wall was reported by some authors.1,2,10
Because this lesion is harmless, the necessity of biopsy or surgical remotion can be discussed, mainly when it is well-characterized and the diagnosis can be clinically defined.2,4-6 However, the lymphoepithelial cyst is commonly treated by the surgical remotion1,2,4,5,7,9, as it was in this case report. All injuries must be cautiously diagnosed and when there are doubts about the differential diagnosis, it is necessary to perform a biopsy and microscopic examination to establish a conclusive position.3,4,6
CONCLUSION
By the fact that lymphoepithelial cyst has similar clinical characteristics to other lesions that occur in the oral cavity and considering its rare occurrence, it is important to emphasize that the diagnosis should be done by biopsy, in a conservative way, removing it totally.
REFERENCES
1.Khelemsky R, Mandel L. Lymphoepithelial cyst of mouth floor. J Oral Maxillofac Surg. 2010;68(12):3055-7.
2.Neville BW, Damm DD, Allen CM, Bouquot JE. Oral and Maxillofacial Pathology. Saunders/Elsevier; 2009.
3.Gallagher G, Kabani S, Noonan V. Oral lymphoepithelial cyst. J Mass Dent Soc. 2006;54(4):52.
4.Yang X, Ow A, Zhang CP, Wang LZ, Yang WJ, Hu YJ, Zhong LP. Clinical analysis of 120 cases of intraoral lymphoepithelial cyst. Oral Surg Oral Med Oral Pathol Oral Radiol. 2012;113(4):448-52.
5.Silva MM, Castro AL, Soubhia AMP, Crivelini MM. Lymphoepithelial cyst in jugal mucosa. Int. J. Odontostomat. 2011;5(1):55-8.
6.Khelemsky R, Mandel L. Lymphoepithelial cyst of mouth floor. J Oral Maxillofac Surg. 2010;68:3055-7.
7.Stramandinoli-Zanicotti RT, de Castro Ávila LF, de Azevedo Izidoro AC, Izidoro FA, Schussel JL. Lymphoepithelial cysts of oral mucosa: two cases in different regions. Bull Tokyo Dent Coll. 2012;53(1):17-22.
8.López-Jornet P. Oral lymphoepithelial cyst. Ann Dermatol Venereol. 2007;134(6-7):588.
9.Nonaka CF, Henriques AC, de Matos FR, de Souza LB, Pinto LP. Nonodontogenic cysts of the oral and maxillofacial region: demographic profile in a Brazilian population over a 40-year period. Eur Arch Otorhinolaryngol. 2011;268(6):917-22.
10.Varnholt H, Thompson LDR, Pantanowitz L.Salivary gland lymphoepithelial cysts. Ear, Nose & Throat Journal. 2007;86(5):265.
Recibido: 19 de agosto de 2012.
Aprobado: 5 de septiembre de 2012.
Dr. Evanice Maria Marçal Vieira. University of Cuiabá, Cuiabá, Mato Grosso, Brazil. Correo electrónico: evanice_mmv@yahoo.com.br
