










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista

Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkRevista Cubana de Estomatología
versión impresa ISSN 0034-7507versión On-line ISSN 1561-297X
Rev Cubana Estomatol vol.55 no.4 Ciudad de La Habana oct.-dic. 2018
PRESENTACIÓN DE CASO
Acute herpetic gingivostomatitis in adult patients
Gingivoestomatitis herpética aguda en paciente adulto
Helder Domiciano Dantas Martins1
Priscilla Sarmento Pinto1
Tácio Candeia Lyra1
Victor Yuri Nicolau Ferreira1
Paulo Rogério Ferreti Bonan1
1 Universidade Federal da Paraíba. Brasil.
ABSTRACT
Introduction: Herpetic gingivostomatitis is an infection caused by herpes simplex virus, which affects mainly children patients, being uncommon this manifestation in adults. It initially appears with prodromal signs and then local signs show up. The treatment for this disease is only supportive, because there is already a peak of viral replication when it was diagnosed.
Objectives: To report a case of herpetic gingivostomatitis and to discuss its clinical characteristics and treatment.
Case report: The patient looked for clinic care for presenting painful oral lesions with little time of evolution. With no medical history, the patient reported using antibiotics and antifungals. Oroscopy showed multiple coalescing ulcerative lesions affecting the gum tissue, tongue, lips and hard palate. It has been diagnosed clinically as herpetic gingivostomatitis and has been treated with supportive treatment (analgesics, topical anesthetic and chlorhexidine digluconate 0,12 %). The patient returned after one week with improvement of the condition.
Conclusion: The correct diagnosis, through the evident clinical manifestations, prevents the indiscriminate use of antibiotics, leading to better response of the patient.
Keywords : herpes simplex virus; herpetic gingivostomatitis; oral diagnosis.
RESUMEN
Introducción: La gingivoestomatitis herpética es una infección causada por el virus herpes simple, que afecta principalmente a los pacientes infantiles, la cual resulta inusual en adultos. Inicialmente surge con señales prodrómicas y solo después se presentan señales locales. El tratamiento para este cuadro es solo de soporte, pues cuando se diagnostica ya hay un pico de replicación viral.
Objetivo: informar un caso de gingivoestomatitis herpética y discutir sus características clínicas y tratamiento.
Presentación del caso: El paciente buscó atención clínica por presentar dolorosas lesiones bucales con poco tiempo de evolución. Sin historial médico, informó que estaba usando antibióticos y antifúngicos, sin remisión de la condición. En la oroscopia se observaron múltiples lesiones ulcerativas coalescentes que afectan el tejido de la gingiva, la lengua, los labios y el paladar duro. Se ha diagnosticado clínicamente como gingivoestomatitis herpética y se ha tratado con tratamiento de apoyo (analgésicos, anestésicos tópicos y digluconato de clorhexidina al 0,12 %). El paciente regresó después de una semana con una mejoría de la condición.
Conclusion es: El correcto diagnóstico, a través de las manifestaciones clínicas evidentes, previene el uso indiscriminado de antibióticos, lo que lleva a una mejor respuesta del paciente.
Palabras clave: virus herpes simples; gingivoestomatitis herpética aguda; diagnóstico bucal.
INTRODUCTION
Acute herpetic gingivostomatitis (GHA-in Portuguese) or primary herpes is an infectious disease caused by HSV-1 (herpes simplex virus 1) and less often by HSV-2 (herpes simplex virus 2).1,2 HSV-1 has a greater predilection for the head and neck, spreading mainly through active lesions and saliva. HSV-2 is more related to lesions in the genital area.1,3
Normally the primary herpes infection is asymptomatic and occurs during childhood,4 when there is presence of symptoms, these are represented by fever, cervical lymphadenopathy, headache, and presence of multiple small vesicles that progress to ulceration in the oral cavity and perioral region.3 The involvement of adult patients for primary infection is unusual.1,2
The diagnosis of GHA is performed based on clinical features found in the patient or through some laboratory tests that may be useful when there is doubt about the diagnosis, among them, the most used are viral culture, immunofluorescence and recognition through the technique of Polymerase Chain Reaction.4
There is no specific treatment for the condition; However, an option is usually a palliative where many cases can be managed by supportive care, including maintenance of fluids, use of analgesics to reduce fever and use of topical anesthetics such as viscous lidocaine to decrease oral pain.5,6
The GHA is a self-limiting illness that usually resolves within 7 to 14 days in immunocompetent individuals. The management of these patients should be facing the resolution of symptoms. Antiviral therapy is most effective when given in the prodromal stages of the disease.3,4 The objective of this study is to report a case of GHA and discuss its clinical characteristics and treatment.
CASE REPORT
The male patient, pheoderma, 19 years old, attended at the stomatology clinic at Federal University of Paraiba in João Pessoa-Paraiba, complaining of oral lesions with painful symptoms a few days of evolution.
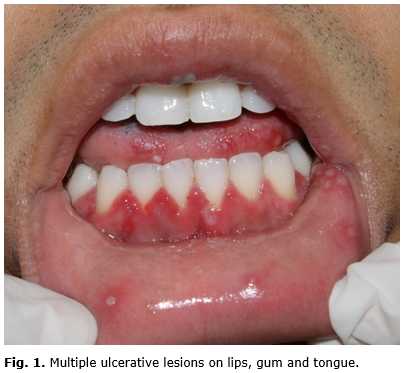
In anamnesis, it reported having good general health, with no significant pathological history and he was making use antibiotics and antifungal for three days without remission. Complained that period, fever, prostration, and dysphagia. In ectoscopic examination, presented no change worthy of note. In oroscopy observed multiple coalescing ulcerative lesions affecting the gum tissue, tongue, lips and hard palate (Fig. 1 and 2). Faced with this situation, the diagnostic hypotheses were: Primary Acute Herpetic gingivostomatitis, herpangina or other viral infection because they are the mainly differential diagnosis.

Complete blood count was ordered, ELISA Anti-HIV and syphilis in order to verify possible immune-commitment, since it was not reported any history of infection with herpesvirus. In view discrete leukocytosis and non-reactive in the other tests, the diagnosis was closed in gingivostomatitis primary herpetic acute.
The treatment was adopted to intervene in painful symptomatology, support being prescribed drugs such as analgesics and topical anesthetic, and to 0,12 % chlorhexidine digluconate; in order to assist in cleaning and possible secondary infection due to injury.
After seven days, the patient returned to the clinic, with total remission of the lesions and symptomatic complaints (Fig. 3). The patient is in follow up of 06 months, with no recurrences of injuries.

DISCUSSION
Primary acute herpetic gingivostomatitis (GHAP) begins abruptly presenting as prodromal and systemic signs: general malaise, fever and headache. Subsequently these systemic manifestations, local lesions develop as numerous punctate vesicles with 1 to 2 mm to break down rapidly and turn into small ulcerations, spontaneous remission suffering from 7 to 14 days all where these characteristics were observed in our patient.1,5,7
The involvement of adult patients by the primary manifestation of herpes simplex is very uncommon, being the most prevalent involvement in children between 6 months and 5 years of age, where they are highly contagious and may have complications ranging 8/7 It is usually seen only in adults when these are not exposed to the virus during childhood or when with compromised immunity.4 In our case, the patient was an adult where immunosuppression was discarded from the laboratory and the patient reported negative history for herpes infection.
The supportive treatment was used for eliminating the painful symptoms to allow for adequate feeding and cleaning. Antiviral therapy is indicated only at the beginning of the demonstrations, assuming that this period was not achieved viral replication apex.8 In this case, the patient appeared to meet on the sixth day of symptoms and antiviral medication was not prescribed because would not have the correct effectiveness.
Diseases such as aphthous stomatitis, acute necrotizing ulcerative gingivitis, herpangina and other viral lesions are reported as the main differential diagnosis of acute herpetic gingivostomatitis.2,9 Besides that, It is important to distinguish primary from recurrent herpetic infection by the history and previous episodes of vesicular eruptions on their lips.10 In the case reported, other viral infections were ruled out due to clinical characteristics of the lesion and the tests requested. The herpangina, as well as the reported disease characterized by the presence of multiple oral ulcers, although they typically are located in abutment and soft palate tonsil, one which was not observed in our patient.1
Although uncommon in adults, the patient's condition was quite evident and does not require the use of laboratory tests to identify the infectious agent. The literature reports that tests such as viral culture, PCR and microscopic analysis can assist in cases of infections with nonspecific manifestations.3,9
With the patient's medical history, it was clear the fundamental role of the CD in the diagnosis of disease and may be the health professional first to be sought.4 In addition, it must observe all the evolutionary history and the patient's clinical manifestations for a correct diagnosis.
This condition must be diagnosed and treated properly, returning the well-being and avoiding secondary problems for the patient, therefore, the dentist should be able to diagnose and treat GHAP. The correct diagnosis will prevent the indiscriminate use of antibiotics and other medication, as well as bring a better response to the patient.
Conflicto de intereses
No se declara conflicto de intereses.
REFERENCES
1. Neville BW, Damm DD, Allen CM, Bouquot JE. Oral and maxillofacial pathology, 4th ed. Rio de Janeiro: Saunders Elsevier; 2016.
2. George AK, Anil S. Acute herpetic gingivostomatitis associated with herpes simplex virus 2: report of a case. Journal of international oral health: JIOH. 2014;6: 99.
3. Santos MPDM, Morais MPLDA, Fonseca DDD, Faria ABSD, Silva IHM, Carvalho AA, et al. Herpesvírus humano: tipos, manifestações orais e tratamento. Odontologia Clínico-Científica. 2012;11:191-6. Access: 14/07/2017. Available from: http://revodonto.bvsalud.org/scielo.php?script=sci_arttext&pid=S1677-38882012000300004
4. Ajar AH, Chauvin PJ. Acute herpetic gingivostomatitis in adults: a review of 13 cases, including diagnosis and management. Journal-Canadian Dental Association. 2002;68:247-51.
5. Narendra SK, Sahani NC, Moharana DN. Manifestations of Acute Herpetic Gingivostomatitis in Human Immunodeficiency Virus: Positive Patients. Journal of International Oral Health. 2016;8:460.
6. Balasubramaniam R, Kuperstein AS, Stoopler ET. Update on Oral Herpes Virus Infections. Dental Clinics of North America. 2014 Apr 1;58(2):265-80.
7. Goldman RD. Acyclovir for herpetic gingivostomatitis in children. Can Fam Physician. 2016 May;62(5):403-4.
8. Geller M, Neto MS, Ribeiro MG, Oliveira L, Naliato EC, Abreu C, et al. Herpes simples: atualização clínica, epidemiológica e terapêutica. Jornal Brasileiro de Doenças Sexualmente Transmissíveis. 2012;24:260-6.
9. Regezi JA, Sciubba JJ, Jordan RC. Oral pathology: clinical pathologic correlations. 6th ed, Rio de Janeiro: Saunders Elsevier; 2013.
10. Mohan RPS, Verma S, Singh U, Agarwal N. Acute primary herpetic gingivostomatitis. BMJ Case Rep. 2013 Jul 8;2013. Access: 14/07/2017. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3736476/
Recibido: 12/01/2017
Aceptado: 24/05/2018
Helder Domiciano Dantas Martins. Universidade Federal da Paraíba. Brasil.
Correo electrónico: helderdomiciano@gmail.com

