










 Servicios personalizados
Servicios personalizados Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkINTRODUCTION
Implant stability is defined as the absence of movement at the moment of measurement.1) This factor can be measured at the moment of implant placement (primary stability) or once the osseointegration process is in progress (secondary stability).2) Primary stability includes the mechanical attachment of an implant in the surrounding bone at the insertion, whereas secondary implant stability is the tissue response to the implant and subsequent bone remodeling processes.2 Some researchers have reported that early failure may be caused by poor implant stability, thus, primary and secondary implant stability are considered key factors for treatment success.2,3)
Several methods have been used to examine implant stability at insertion and during the osseointegration period.1,2,3) Despite the availability of a wide variety of stability quantifiers, only some of these have been validated. Currently, insertion torque and resonance frequency analysis (RFA) are seen as the gold standard for evaluating in vivo implant primary stability.3 Insertion torque is a mechanical parameter influenced by surgical procedure, implant design, and bone quality. A high insertion torque means that the implant is firmly embedded into the bone and that is mechanically stable. Some authors have found that insertion torque values above 32 Ncm are an indication of adequate primary stability.3)
RFA is a method used to determine implant stability, which consists on sending magnetic pulses to a small metal rod temporarily attached to the implant. As the rod vibrates, the probe reads its resonance frequency and translates it into an ISQ value (implant stability quotient value).4 The value obtained is a combination of bone implant contact and bone density around the implants.4 RFA instruments perform a quick and simple measurement, which results in a value called ISQ. The ISQ ranges from 1 (low stability) to 100 (high stability).4,5 It has been reported that ISQ values at implant insertion should be ≥ 60 to achieve sufficient implant stability.5
RFA measurements are used to assess the implant stability immediately after placement, as well as to measure the stability during the healing time.5,6 This helps the dentist to determine whether more healing time (osseointegration) is needed before the placement of the prosthetic tooth, as well as to identify patients with compromised bone tissue, or other risk factors.6
Many factors should be considered when attempting to achieve primary stability, including bone quality, osteotomy preparation, implant design, implant surface enhancement, and implant length and diameter.7,8 Several surgical techniques have been used effectively for bone augmentation in height and width.9 However, because of postoperative complications, longer treatment duration and high treatment costs, it is sometimes difficult for the patient to accept these procedures.9,10 As an alternative to more complicated augmentation procedures, short dental implants have been increasingly used in case of vertical alveolar bone height deficiencies.10 Recent studies have reported equivalent success rates for rough-surfaced short implants when comparing to standard length implants.11,12 Although success and survival of short implants have been extensively investigated, studies on midterm and long-term outcomes are limited.
This study aimed to determine the influence of implant length on primary and secondary stability in type II and type III bones using resonance frequency analysis method.
METHODS
A prospective study was conducted in the department of Oral maxillofacial Implantology at the School of Dentistry of the University of Chile between April 2006 and June 2007. All patients gave their informed consent in writing to take part in the study.
The present study included 16 patients (4 males and 14 females) with a mean age of 46 years (maximum age 72 years and minimum age of 26 years). A total of 38 screw type implants were placed in the maxilla and mandible, in type II and type III bones according to Leckholm y Zarb classification. The following implant trademarks were included in this study: Brånemark System® MK III, OSSEOTITE® Implant System, LTX 3i, Restore®, B&W®.
Inclusion criteria were: (1) Smokers consuming less than 5 cigarettes per day; (2) Systemic diseases outlined accord with the American Society of Anesthesiologists (ASA) classification (ASA I and ASA II); (3) Minimum bone availability of 15 mm in height and 5 mm in width; and (4) Periodontal health and adequate oral hygiene.
Exclusion criteria were: (1) Presence of active infection or inflammation; (2) Presence of pathological lesions in the maxilla or mandible; (3) Patients with previous history of head and neck radiotherapy treatment.
The patient’s medical charts were completed registering personal data, medical health, and bucco-dental status. Extra-oral and intraoral pictures and periapical and panoramic radiographs were taken. Sites with inadequate bone volume were evaluated clinically and with Cone-beam computed tomography (CBCT) before surgery. All surgeries were performed by lifting a full-thickness flap and performing the full sequence of surgical drills. 21 implants had an average contact area of 237 mm2 including 2 sizes (diameter of 3.75mm and a length of 13mm and 15mm) and seventeen implants had an average contact area of 129 mm2 (diameter of 3.75 mm and a length of 7 mm). The contact area was quantified through a simplified method.13
After implant placement, primary implant stability was measured by the ISQ value (ISQ1). RFA measurements were recorded using Osstell™ Mentor, using a transducer screwed to the implant called Smartpeg®, which is connected wirelessly to a minicomputer that transforms the RFA records into ISQ units. Each implant was measured from two different angles, around 90 degrees apart and parallel to the crestal line. Secondary implant stability (ISQ2) was recorded at the moment of implant connection, between 4 to 6 months after the implant placement.
Statistical analysis: the normality of data was assessed by Shapiro-Wilk. The implant length data was compared with the primary and secondary stability ISQ values using the unpaired T-test. The alpha value considered was 0.05, and software used was SPSS v. 11.0 (IBM, NY, USA).
RESULTS
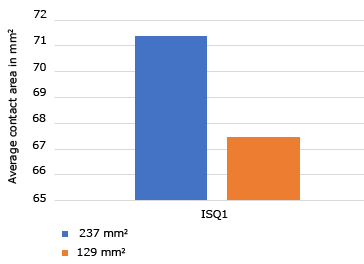
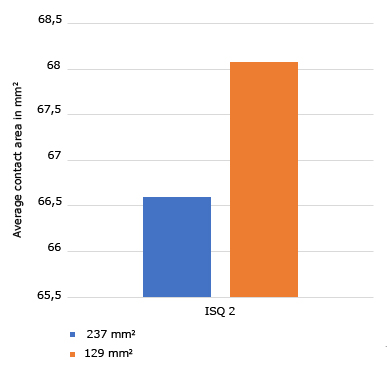
For implants with an average contact area of 237 mm2 including 2 sizes (3.75 mm/13 mm and 3.75 mm/15 mm) the ISQ1 average value was 71.37 and the ISQ2 average value was 66.6. For implants with an average contact area of 129 mm2 (3.75 mm/7 mm) the ISQ1 average value was 67.47 and the ISQ2 average value was 68.08. When comparing the implants with an average contact area of 237 mm2 and with an average contact area of 129 mm2 no significant differences were found in terms of ISQ1 and ISQ2 average values. Average ISQ1: p = 0.6172 and average ISQ2: p = 0.5174 with Wilcoxon Test (Fig. 1 and Fig. 2).
In the present study, no significant differences were found in terms of ISQ1 and ISQ2 values, when comparing implants with different lengths. Similarly, to our results, Bischof et al14 did not find that the length or diameter of the implants had a significant influence on the primary stability for both immediate and delayed loading implants. This corroborates our study findings when comparing the primary and secondary stability of short (129 mm2) versus long (237 mm2) implants of the same macro-design. Correspondingly to our results, Barikani et al15) found that the difference was not significant between implants of 15 mm and 13 mm long, neither in narrow platform nor in regular platform implants. Other studies also reported that implant length and diameter, when considered as single parameters, did not have any effect on stability.16,17
Das Neves et al18 in 2006 carried out a systematic review of longitudinal studies between 1980 and 2004 on the use of short implants. The researchers reported that implant failure was associated with a series of factors, which become influential when two or more of them act together. These factors include poor bone quality, short implants, small diameter, parafunction, gender, infection and location of the implanted area. It was concluded that short implants without other risk factors do not compromise clinical success.
As in the present study, Rossi et al19 found an average ISQ value of 70.2 ± 9 at implant insertion for 6 mm long implants. In a later study, Queiroz et al20) compared the mechanical stability of short implants versus standard implants placed in the edentulous posterior mandible by means of RFA. It was reported that the mean ISQ value at implant placement was 68 for standard implants and 72 for short implants. However, no significant difference was found between the short and standard implants in the observation periods.
Results demonstrate that implant length does not influence primary and secondary stability in type II and type III bones. Furthermore, implants with an average contact area of 237 mm2 (13 mm and 15 mm length) compared with implants with an average contact area of 129 mm2 (7 mm length) show no significant differences in terms of ISQ1 and ISQ2 average values.

