










My SciELO
 Custom services
Custom servicesServices on Demand
Journal

Article
 Spanish (pdf)
Spanish (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkRevista Cubana de Medicina Tropical
Print version ISSN 0375-0760On-line version ISSN 1561-3054
Rev Cubana Med Trop vol.62 no.3 Ciudad de la Habana Sept.-Dec. 2010
REPORTE DE CASO
Chromoblastomycosis in Santa Catarina state, Brazil
Cromoblastomicosis en el estado de Santa Catarina, Brasil
Elidiana de BonaI; Luciane Maria CantonI; Alexandre Meneghello FuentefriaII
I Especialista en Laboratorio Clínico. Facultad de Farmacia, Centro de Ciências da Saúde. Universidade Comunitária da Região de Chapecó, Brasil.
II Máster en Microbiología. Doctor en Ciencias. Profesor Adjunto. Facultad de Farmacia, Universidade Federal do Rio Grande do Sul, Brasil.
ABSTRACT
A case of chromoblastomycosis caused by Cladophialophora carrionii is reported. The diabetic and hypertensive patient presented serpiginous and verrucous lesions, with centrifugal evolution. The patient, with a history of disease for 59 years, had not been diagnosed or treated before. Dematiaceous septate hyphal and elliptical conidia were seen on microscopic observations. The isolated fungus was identified on the basis of micro-macromorphologic characteristics.
Key words: chromoblastomycosis, Cladophialophora carrionii, dematiaceous fungi.
RESUMEN
Se reportó un caso de cromoblastomicosis causado por Cladophialophora carrionii. El paciente, diabético e hipertenso, presentaba lesiones de apariencia verrugosa y serpiginosa, con evolución centrífuga. Tenía un historial de enfermedad hace 59 años sin haber sido diagnosticado hasta entonces. En el examen microscópico de observaron elementos hifales septados, pigmentados y con conidios elípticos. La identificación del hongo se basó en las características macromorfológicas y micromorfológicas.
Palabras clave: cromoblastomicosis, Cladophialophora carrionii, hongos dematiáceos.
INTRODUCTION
Chromoblastomycosis is a subcutaneous mycotic disease, usually characterized by the development of verrucose, dyschromic and ulcerative lesions.1,2 The infection frequently occurs through the trauma by contaminated organic material with conidia and mycelium of the fungus that are distributed in soil, air and plants, with the highest incidence in tropical and subtropical regions of Latin America, Africa and Asia. In Brazil, the states of Rio Grande do Sul, São Paulo, Rio de Janeiro, Minas Gerais and the entire Amazon region are reported as endemic regions.2,3
Chromoblastomycosis, as well as phaeohyphomycosis, are the major mycoses caused by dematiaceous fungi, characterized by agents of black cottonous colonies, unlike of eumycetoma, which is also a fungal infection characterized by the presence of granules which are dense aggregates of hyphae and other vegetative components. The most common species associated in the epidemiological context of chromoblastomycosis in Brazil are Phialophora verrucosa, Cladophialophora carrionii, Fonsecaea pedrosoi, Fonsecaea compacta, and Rhinocladiella aquaspersa.4-6
In the last years, about 150 cases of chromoblastomycosis have been described in southern Brazil, but none in the state of Santa Catarina. We add to the Brazilian casuistic one new and persistent case of chromoblastomycosis with mycological diagnosis.
CASE PRESENTATION
Patient, male, 73 years old, rural worker, with diabetes mellitus type 2 (DM2) and hypertension, a resident in Cunha Porã city, located in the state of Santa Catarina in southern Brazil, with a nonspecific erythematous papular and vegetating plaque on the feet and 2/3 of the lower legs (Fig. 1). The patient reports that at age 14, started with body aches and fever. After years arose red patches with edema and later verrucous lesions, presenting evolution with centrifugal serpiginous appearance and purulent draining. In culture grew a filamentous fungus, with colony wrinkled, velvety and dark green, in addition of beige colonies, with creamy aspect, typical of yeast.
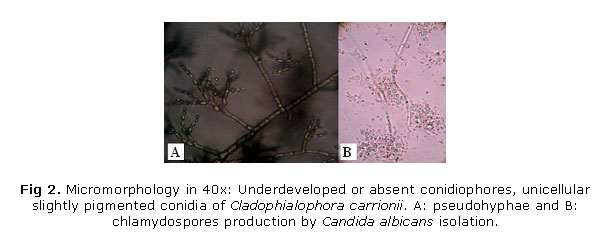
Microscopy of the dark olive-green colonies showed characteristic dematiaceous septate hyphae, 2 to 5 mm in width, with oval to elliptical conidia also dark brown color, characteristic of Cladophialophora carrionii (Fig. 2A). In turn, the microculture of yeast colonies showed chlamydospores and conformation of pseudohyphae characteristic of Candida albicans (Fig. 2B), performing the role of opportunistic in injury. The characteristics of the lesion presented also corroborate the description of chromoblastomycosis in accordance with Minotto et al.7 and Queiroz-Telles et al.8
The treatment suggested by the general practitioner was on itraconazole 100 mg daily doses for 6 months. After 40 days of use there was little improvement.
DISCUSSION
The real prevalence of chromoblastomycosis is apparently more frequent in immunocompetent patients than in immunosuppressed, such as those undergoing corticosteroid therapy, diabetes mellitus, transplant recipients, patients with chronic infectious diseases, patients on chemotherapy, among others.3,9,10 The isolation of the causative fungi from nature on several different occasions has added to the demonstration that fungi entry into the host's body occurred through traumatic inoculation.2,3 In this condition, notes the prevalence of reported cases in rural workers clinically healthy, therefore immunocompetent, but who have extensive contact with the ground in endemic regions where the causative agents are found.1
Regarding the geographical epidemiology of chromoblastomycosis, the frequency of cases occurs in most regions of tropical and subtropical climate of the planet because the biochemical and physiological characteristics of the etiologic agents are more easily expressed when associated with these climates.2,11,12 Based on the correlation between the subtropical climate of the region of Santa Catarina with the occupation of the patient reported, realizes the importance of preventive measures against subcutaneous mycoses in any situation of risk, such as a skin perforation, a tear, or even with scratches vegetable skin-piercing. The location of the lesion in lower limbs of the patient in study, closely related to the type of work activity performed, reinforces the hypothesis of traumatic implantation of the fungus in the tissue to produce this infection.1,9,13
Chromoblastomycosis caused by Fonsecaea pedrosoi is responsible for most cases of the disease in the southern and southeastern Brazil, and refractory to various treatments, which is characterized as a chronic mycosis.5,11,14 However, an incorrect diagnosis often occurs because of similarities with other causative agents. In cases of more extensive lesions, the flucytosine is the drug of choice for both etiologic agents, observing a rapid remission of the disease. But when there are relapses or resistance, the recommendation is the combination with other drugs, for example, amphotericin B, itraconazole or thiabendazole, where for a long period (3 to 6 months).1
This case is the first report described and discussed of chromoblastomycosis in Santa Catarina state, southern Brazil. The importance of the description of cases, as in this study, justified by the need to document the different patterns of clinical signs that chromoblastomycosis presents. Lesions are usually chronic for years and, of confusing laboratory diagnosis, always accompanied by subtherapeutic treatment or by resistance of the etiologic agent.
REFERENCES
1. Ameen M. Managing chromoblastomycosis. Trop Doct. 2010;40:65-7.
2. Garnica M, Nucci M, Queiroz-Telles F. Difficult mycoses of the skin: advances in the epidemiology and management of eumycetoma, phaeohyphomycosis and chromoblastomycosis. Curr Opin Infect Dis. 2009;22:559-63.
3. Martínez RL, Tovar LJM. Chromoblastomycosis. Clin Dermatol. 2007;25:188-94.
4. Naggie S, Perfect JR. Molds: Hyalohyphomycosis, phaeohyphomycosis, and zygomycosis. Clin Chest Med. 2009;30:337-53.
5. Ribeiro EV, Soares AS, Ferreira WM, Cardoso CG, Naves PLF, Silva Dias MS. Cromoblastomicose: doença presente na realidade populacional brasileira. Rev Bras Anal Clin. 2006;38:189-92.
6. Wilhelmus KR. Climatology of dematiaceous fungal keratitis. Am J Ophthalmol. 2005;140:1156-7.
7. Minotto R, Bernardi CD, Mallmann LF, Edelweiss MI, Scroferneker ML. Chromoblastomycosis: A review of 100 cases in the state of Rio Grande do Sul, Brazil. J Am Acad Dermatol. 2001;44:585-92.
8. Queiroz-Telles F, McGinnis MR, Salkin I, Graybill JR. Subcutaneous mycoses. Infect Dis Clin N Am. 2003;17:59-85.
9. Vijaya D, Kumar BH. Chromoblastomycosis. Mycoses. 2005;48:82-4.
10. Esterre P, Queiroz-Telles F. Management of chromoblastomycosis: novel perspectives. Curr Opin Infect Dis. 2006;19:148-52.
11. Lupi O, Tyring SK, McGinnis MR. Tropical dermatology: fungal tropical diseases. J Am Acad Dermatol. 2005;53:931-51.
12. Casado YJ, Gómez SE. Lesiones verrucosas en la pierna. Piel. 2007;22:33-6.
13. Najafzadeh MJ, Rezusta A, Cameo MI, Zubiri ML, Yus MC, Badali H, et al. Successful treatment of chromoblastomycosis of 36 years duration caused by Fonsecaea monophora. Med Mycol. 2009;1:1-4.
14. Andrade T, Cury A., Castro L, Hirata M, Hirata R. Rapid identification of Fonsecaea by duplex polymerase chain reaction in isolates from patients with chromoblastomycosis. Diag Microbiol Inf Dis. 2007;57:267-72.
Recibido: 27 de enero de 2010.
Aprobado: 14 de mayo de 2010.
Dr. Alexandre Meneghello Fuentefria. Departamento de Análises, Universidade Federal do Rio Grande do Sul. Avenida Ipiranga 2752, Bairro Santana 90610-000 Porto Alegre, RS Brasil. E-mail: alexmf77@gmail.com


{kind=link}
{kind=link}