










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista

Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkRevista Cubana de Hematología, Inmunología y Hemoterapia
versión impresa ISSN 0864-0289versión On-line ISSN 1561-2996
Rev Cubana Hematol Inmunol Hemoter vol.33 no.4 Ciudad de la Habana oct.-dic. 2017
ARTÍCULO ORIGINAL
Hematopoietic stem cell transplantation in Puebla, México. Traveled roadand goals achieved
El trasplante de células progenitoras hematopoyéticas en Puebla. Ruta seguida y actividad acumulada
José Alejandro Limón Flores, Uendy Pérez Lozano, Juan Carlos Solís Poblano, Petty Rodríguez Castillo, Vanessa Terán Cerqueda, Jorge Luis López Marthen, Gabriela Sarmiento Candelaria, Cindy Trinidad Vera Villicaña, Balbina Gutiérrez Gurrola, Diana Arlett Herrera Madrid, Vanessa Balán Ortiz, Liliana Vazquez Gutiérrez, Elizabeth Morales López, Jesús Manuel López Valles, Lilia Adela García Stivalet
Specialties Hospital National Medical Center "Manuel Ávila Camacho". Mexican Social Security Institute (Imss), Puebla, México.
ABSTRACT
Introduction: In México there are only 4 cities that have significantly active hematopoietic stem cell transplantation programs; onlyin 3 of those cities, the most important national public health institution IMSS (Mexican Social Security Institute) count with them. The cities where these programs are found are Mexico City, Monterrey and Puebla. Since the beginning of this decade, and before, the productivity of these transplant programs in this public health institution is low, performing on average 148 transplants every year.
Results: In the span comprised between April 1995 and October 2016, we have performed 474 hematopoietic transplants in our hospital; 229 of them were allogeneic and 245 autologous, in adult and children population. This accumulated experience has allowed the implementation of all the variety of hematopoietic stem cell transplantation available in our country, this has opened up the opportunity, for the first time in our institution, the possibility to provide a donor for every patient who requires an hematopoietic transplant, overcoming the phase in which patients could not be submitted to the procedure for lack of a compatible donor.
Conclusions: The goals achieved in our hospital confirm the feasibility in developing uninterrupted long term transplant programs in hospitals not specially equipped with technology nor abundant funds of the public health system in the national province, and it shows that this programs can be created and developed in hospitals with similar conditions to ours in México, Latin America and middle-low income countries.
Keywords : hematopoietic transplantation, low- median technology, budget
RESUMEN
Introducción: en méxico solo cuatro ciudades cuentan con programas de trasplante hematopoyético significativamente activos y en solo tres los tiene el IMSS, la principal institución de salud del país: Monterrey, Puebla y la ciudad de México .La productividad de estos centros del sector público es muy baja, realizando en conjunto 148 trasplantes en promedio por año desde el principio de la década actual.
Resultados: en el lapso comprendido entre abril de 1995 y octubre de 2016, se efectuaron 474 trasplantes hematopoyéticos en nuestro hospital; 229 de ellos fueron alogénicos y 245 fueron autólogos, en población adulta e infantil. Esta experiencia acumulada ha permitido la implementación de todas las variedades disponibles en el país de estos procedimientos, lo que ha generado, por vez primera en la institución, poder contar con un donante para todo paciente que requiera un trasplante hematopoyético; superándose la etapa en la que los enfermos no se sometían al procedimiento por falta de un donador compatible.
Conclusiones: la actividad acumulada en nuestra unidad hospitalaria confirma la factibilidad de desarrollar programas ininterrumpidos, a largo plazo, de estos procedimientos terapéuticos en hospitales no especialmente dotados de tecnología ni presupuesto del sector público de la provincia nacional y denota que estos mismos programas pueden ser creados y desarrollados en nosocomios con condiciones similares al nuestro en diversos territorios de México, de Latinoamérica y de países con ingreso medio-bajo.
Palabras clave: trasplante hematopoyético con tecnología y presupuesto bajos.
INTRODUCTION
The hematopoietic stem cell transplantation has experienced important progress around the world in the last decades. Worldwide at the end of 2012 a total number of one million patients that received a transplant was achieved;1,2 recently the figure of 25 million voluntary bone marrow donors was attained, as well as over 550 thousand units of cryopreserved umbilical cord stem cells. In Europe over 40 thousand hematopoietic transplants are performed annually,3 and over 19 thousand in the United States, where there are over 340 thousand transplants performed, of which 210 thousand are allogeneic and 125 thousand autologous.4
The deployed medical activity in Mexico in the field of hematopoietic stem cell transplantation has suffered an important lag in relation with developed countries and in comparison with similar underdeveloped countries despite having begun since 1979.5-7. At present it is estimated that less than 5% of patients with diseases that are susceptible of being controlled or cured with this kind of transplant will receive it. 8 The primary reason for this delay is the scarcity and low activity of the hematopoietic stem cell transplantation programs in our country, both in public and private institutions, especially acute shortage in the national province. For that reason, our country suffers a double adverse reality; the first one is the backwardness in relation to developed countriesand the second one, even more opprobrious, the underdevelopment of the province with respect to the capital. These situations undermine continually the development of modern medicine, specifically of hematology, in our country.
Since the middle of the last decade of the XX century we designed a project to develop hematopoietic stem cell transplantation in our hospital tending to eliminate the local postponement and to strengthen the implementation of this area in hematology that would allow the treatment of patients in the most effective and modern way possible. This project was based on an elemental but strategic plan that consisted in performing transplants in the simplest possible manner to the more complex; this would allow the achievement of two goals: the development of an experienced team and financial viability. Following this project we performed first autologous bone marrow transplants with cell refrigeration, later allogeneic bone marrow transplants, afterward peripheral hematopoietic stem cell transplants through apheresis, finally the more complex transplants like those that use non-related umbilical cord stem cells or related donor haploidentical stem cell transplants. Currently this approach has allowed our hospital to perform every type of transplant available in our country, guaranteeing a benefit for our patients, allowing an apprenticeship based on every day experience for our residents, locally strengthening the practice of hematology and positioning our hospital as the most developed in hematopoietic stem cell transplant in our institution, the IMSS.
METHODS
With the goal of analyzing the accumulated productivity in this area and confirming the feasibility of developing long-term programs of hematopoietic transplants in the national province, a retrospective evaluation of the activity developed in hematopoietic transplant in the last 21 years in our hospital was performed. We analyzed separately child and adult population and the number of procedures from two perspectives: the type of transplant performed and the disease that conditioned the indication for transplant.
The type of transplant was analyzed in two groups: allogeneic and autologous. The allogeneic were grouped into the following headings: a) sibling identical HLA donor using stem cells obtained frombone marrow, peripheral blood or umbilical cord; b) related donor different from sibling either from bone marrow or peripheral blood stem cells; c) related or non-related donor of umbilical cord stem cells. The autologous were grouped in the following: a) bone marrow and b) peripheral blood stem cells.
The type of diseases that conditioned the indication for transplant were divided for evaluation in: a) acute myeloid leukemia in first remission or without it, b) acute lymphoblastic leukemia in first remission or without it, c) chronic myeloid leukemia in chronic phase or without it, d) myelodysplastic syndrome, e) other leukemias, f) Hodgkin's lymphoma, g) non-Hodgkin's lymphoma, h) multiple myeloma i) non-hematological tumors, j) aplastic anemia, k) other non-malignant diseases.
The short and long-term outcomes of the different types of transplant performed were not analyzed in the present review nor the evolution followed by the patients according to the underlying diseases that conditioned the transplant.
RESULTS
In the span comprised between April 1995 and October 2016, 474 transplants were performed in our hospital; 229 of them were allogeneic and 245 autologous.
In the adult patient population a total of 248 transplants were performed, 108 of them were allogeneic and 140 autologous.
The allogeneic transplants were performed in patients with the following diseases: acute myeloid leukemia 19 patients, of which 10 were in first complete remission and 9 without it (advanced disease) ; 39 patients with acute lymphoblastic leukemia, 28 in first complete remission and 11 without it; 18 patients with chronic myeloid leukemia, 15 in first chronic phase and 3 with advanced disease; 3 cases of multiple myeloma and 1 case with non-Hodgkin lymphoma; 18 patients with non-malignant hematological diseases, 17 with aplastic anemia and 1 with pure red cell aplasia. All the donors were siblings HLA fully matched in 100 transplants, using bone marrow as the source of stem cells in 16, and in 84 peripheral hematopoietic stem cells obtained through apheresis. In 8 patients a donor different than a sibling 100% HLA compatible was employed, using bone marrow in 5 and peripheral hematopoietic stem cells obtained through apheresis in 3 (table 1).
The autologous transplants were performed in patients with the following diagnosis: 19 patients with acute myeloid leukemia, 18 of them in first remission and 1 with advanced disease; 32 individuals had acute lymphoblastic leukemia, 31 of them in first remission and one with more advanced disease; 35 patients had multiple myeloma; 38 patients with non-Hodgkin lymphoma and 13 with Hodgkin lymphoma; 2 with breast cancer; 1 with multiple sclerosis. Of the total of auto transplants in 17, bone marrow was used as the source of hematopoietic stem cells and in 123 peripheral hematopoietic stem cells through apheresis (table 2).
In pediatric patient population a total of 226 transplants were performed, 121 of them were allogeneic and 105 autologous.
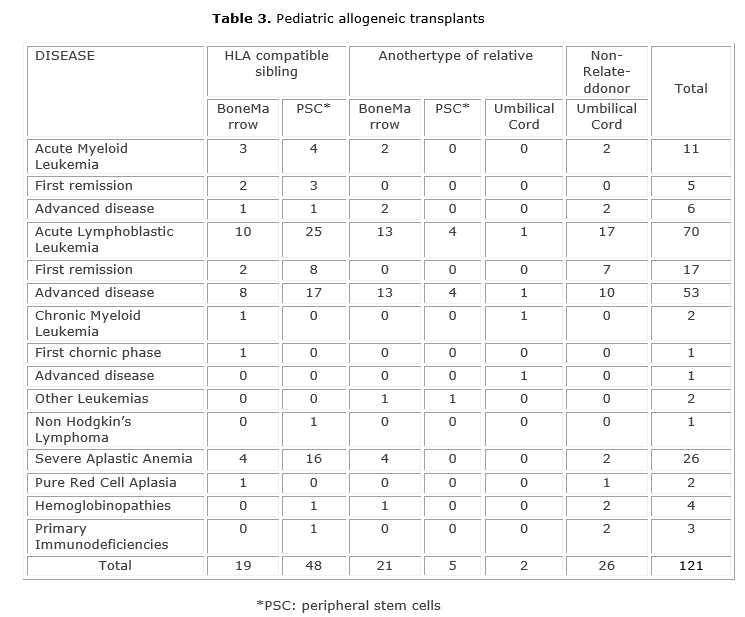
The allogeneic transplants were performed in children with the following diseases: acute myeloid leukemia 11 patients, of which 5 were in first complete remission and 6 without it (advanced disease) ; 70 patients with acute lymphoblastic leukemia, 17 in first complete remission and 53 without it; 2 patients with chronic myeloid leukemia, 1 in first chronic phase and the other one with more advanced disease; 2 suffered of other types of leukemia, and 1 case with non- Hodgkin lymphoma; 35 patients with non-malignant hematological diseases, of which 26 had aplastic anemia, 2 with pure red cell aplasia, 4 with hemoglobinopathies and 3 with immunodeficiencies. The donors were siblings 100% HLA compatible in 67 transplants, of which 48 peripheral hematopoietic stem cells obtained through apheresis was the source of stem cells and in 19 transplants bone marrow was used. In 28 patients a donor different than a sibling 100% HLA compatible was employed, using bone marrow in 21, peripheral hematopoietic stem cells obtained through apheresis in 5 and umbilical cord stem cells in 2. Of the total of allogeneic transplants performed in children, in 26 patients non-related umbilicalcord stem cells cryopreserved was used as source of progenitor cells (table 3).
The autologous transplants were performed in pediatric patients with the following diagnosis: 7 patients with acute myeloid leukemia, all of them in first remission; 73 cases of acute lymphoblastic leukemia, of which 65 were in first complete remission and 8 with more advanced disease; 4 with other type of leukemia; 16 individuals with non-Hodgkin lymphoma and 3 with Hodgkin lymphoma; 2 with non-hematological solid tumors. Of the total of autotransplants performed in 71, the source of hematopoietic stem cells was peripheral stem cells obtained through apheresis and in 34, bone marrow was used (table 4).
DISCUSSION
The route followed in our Hospital, from the simple to the complex, has allowed the development of an experienced team and financial viability, this has made possible the evolution and progressive growth of the hematopoietic transplant locally, having achieved gradually the implementation of all the varieties available of this procedure in our country: allogeneic, autologous; of bone marrow, of peripheral blood; related 100% compatible or haploindentical; non-related donor umbilical cord stem cells; myeloablative and submyeloablative conditioning ; conditioning based only in drugs or total body irradiation,9 as shown in the series of patients transplanted previously reviewed. The results vary widely depending on the type of transplant, the underlying disease and the severity of the same,10,11 from excellent cure rates close to 80% in cases with aplastic anemia, up to less than 10% in acute leukemias in which the transplant was performed without being in complete remission or with the suboptimal therapeutic procedure for their disease. Of particular importance has been to implement alternative sources of hematopoietic stem cells in recent years, particularly non-related umbilical cord stem cells since 2004,12 or coming from related donors haploindentical, different from siblings 100% compatible, since 2013; this implementation has generated the shocking phenomenon to finally count with a donor for every patient that requires an hematopoietic transplant surpassing the painful stage in which patients could not receive the procedure for lack of a compatible donor. Our hospital is the first in our institution (IMSS), in having achieved this gratifying specific situation product of the gradual maturation of the program, whichhas remained in ascent despite the various difficulties encountered by the institution and the country in the last decades.
Despite having almost 400 hospitals in our country (36 of them of third level) with more than 70 thousand doctors, a multitude of hematologists and with an insured population that surpasses 65 million Mexicans,13 the IMSS only counts with active hematopoietic transplant programs in 3 cities, Monterrey and Puebla in the national province, and in Mexico City. Additionally, the productivity of these centers is not precisely high, performing on the whole 148 transplants in average per year since the beginning of this decade (Table 5).14 Thisworrisome situation of underdeveloped conditions impact the vast majority of patients that require this type of treatment to save their lives from serious illnesses and are not able to receive it; the patients that receive the transplants are exceptionally lucky, being less than 5% of the total candidates. This severe insufficiency of transplant resource must be firstly recognized, so in the future as an expected consequence, steps are taken to initiate the establishment of the necessary measures to revert it in medium to long term. The situation is not significantly better in other institutions of the public or private sectors in Mexico where, exceptinga very few hospitals found in the three cities mentioned before, the hematopoietic transplant is an inexistent resource or manifestly insufficient.
Despite building a moderate experience compared to large transplant centers housed primarily but not exclusively in developed countries around the world, the activity performed in hematopoietic transplant in our hospital, counted with hundreds of cases in the last decades, corroborates the feasibility of developing long term programs of this kind of therapeutic procedures in hospitals not especially endowed with technology or robust budget in the public sector in the national province and denotes that this programs can be created and developed in hospitals with similar conditions to ours in various territories of México, Latin America and middle-low income countries. This creation and development contributes to the modern exercise of medicine and to improve significantly the prognosis of patients with serious diseases susceptible of being cured or controlled in the long term.
REFERENCES
1. Gratwohl A, Pasquini MC, Aljurf M, Atsuta Y, Baldomero H, Foeken L, et al. One million haemopoietic stem-cell transplants: a retrospective observational study for the Worldwide Network for Blood and Marrow Transplantation (WBMT). Lancet Haematol .2015;2(3):e91-100.
2. Carreras Foundation .Official web site. http://www.fcarreras.org/es/ (citado:August 12, 2016).
3. Passweg JR, Baldomero H, Bader P, Bonini C, Cesaro S, Dreger P, et al Hematopoietic stem cell transplantation in Europe 2014: more than 40000 transplants annually. Bone Marrow Transplant. 2016;51(6):786-92.
4. Center for International Blood and Marrow Transplant Research. (citado: August 12, 2015). Disponible en: https://www.cibmtr.org/pages/index.aspx. Summary slds. 2015
5. Gale RP, Seber A, Bonfim C, Pasquini M. Haematopoietic cell transplants in Latin America. BoneMarrowTransplant. 2016;51:898-905. doi:10.1038/bmt.2016.35.
6. Sosa-Sánchez R, Córdova MS, Labardini JS, Chávez-Peón F. Trasplante de médula ósea en anemia aplástica. Reporte del primer caso en México. RevInvestClinMex. 1980;32:49-54.
7. Morales-Polanco MR, Pizzuto-Chávez J .Bone marrow transplant in aplastic anemia. Current status and review of the first allogeneic transplants in México.GacMédMéx. 1984;120:49-57.
8. Zamora-Ortiz G, Velázquez-Sánchez-De-CimaS , Hernandez-Reyes J, Vargas- Espinosa J, Ruiz-Delgado GJ, Ruiz-Argüelles GJ. Veinte años de experiencia con trasplantes de células hematopoyéticas en la Clínica Ruiz de Puebla, México. Rev Hematol Mex 2013;14:63-70
9. Limón Flores JA, Pérez Lozano U, Solis Poblano JC, Rodriguez Castillo
P, Zagoya Martinez P, Terán Cerqueda V, et al. El Servicio de Hematología del Hospital de Especialidades del IMSS de Puebla. Datos y cifras. Rev Hematol Mex 2014;15:60-68.
10. Limón-Flores JA, Pérez-Lozano U, Solís Poblano JC, Rodríguez-Castillo P, Zagoya-Martínez P, Lobato-Tolama RD. El programa de trasplante hematopoyético del Hospital de Especialidades del IMSS de Puebla. Experiencia de 15 años. Hematología. 2010;11(4):179-84.
11. Perez Lozano U, Ruiz Ovalle JL, Limon Flores JA, Lobato Tolama RD. Autotransplant in Multiple Myeloma with Oral Melphalan without Cryopreservation. J BoneMarrowRes. 2015;3(1):1-5.
12. Novelo-Garza B, Limon-Flores A , Guerra-Marquez A, Luna-Bautista F, Juan-Shum L, Montero I ,et al. Establishing a cord blood banking and transplantation program in Mexico: a single institution experience. Transfusion. 2008 Feb;48(2):228-36.
13. Diario Oficial de la Federación .Segunda sección. 28 de Abril de 2014. Programa Institucional del Instituto Mexicano del Seguro Social (P.I. I.M.S.S.) 2014-2018. (accedido diciembre 15, 2016). Disponible: https://www.diputados.gob.mx/LeyesBiblio/dof/2014/abr/DOF_28abr14.pdf
14. Reporte Interno. Coordinación Normativa de Donación y Trasplantes de Órganos, Tejidos y Células. Instituto Mexicano del Seguro Social. Año 2011-Junio 2016. Durango No 289 4º piso, Colonia Roma, Delegación Cuauhtémoc, Código Postal 06700, Ciudad de México.Tel. (52) 5552865936
Recibido: enero 18, 2017.
Aprobado: agosto 9, 2017.
J. Alejandro Limón Flores MD . OncoHematology Division Chief Haematology esidency Postgraduate Course Head Professor. Specialties Hospital "Manuel Ávila Camacho", IMSS. 2 Norte.2004, CP 72000, Puebla, Pue, México. E-mail: jose.limonf@imss.gob.mx


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}