










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Total body irradiation (TBI) is a teletherapy modality consisting of irradiating the patient’s body volume homogeneously, which, in the last two decades has suffered an important evolution, from being a cytolytic / palliative treatment, to become the elective radiotherapy method in programs of bone marrow transplant conditioning [1].
The limitations of available input data and problems inherent to the calculation procedures make it difficult to accurately determine the distribution of doses in TBI with the use of most of the planning systems available in radiotherapy services. In addition, variations in the patient's position can alter the distributions dramatically. For this reason, it is necessary to devise an experimental technique to determine the dose during irradiation.
In Vivo Dosimetry (IVD) is the measurement of the dose in real time during a radiotherapy treatment, with detectors fixed to the skin or inside a natural cavity. It is the most direct method to monitor the dose of radiation delivered to the patient [2]. It represents the only way to know if the administered dose is actually the one prescribed and if, it is, together with the verification of portal images, the ultimate quality control on the treatment that allows correcting errors [3].
The routine use of IVD systems has proved being an effective tool for reducing incidental errors, enhancing the patient’s radiation safety.
There are different measurement systems that can be used in vivo dosimetry, such as TLD, semiconductor diodes, MOSFET transistors, etc. [4]. "Hospital Hermanos Ameijeiras'' (HHA) is currently the only center in Cuba performing TBI treatments, where dose calculation is performed using an in-house treatment planning system (AMEPLAN).
To achieve further optimization and ensuring better accuracy of dose delivery during the TBI irradiations, it was decided to implement a comprehensive IVD procedure.
The purpose of this study has been to commission and implement an IVD system for the verification of treatments with the macro-beams of photons used for total body irradiation.
Materials and methods
In order to implement a redundant method of verifying the doses administered with the TBI, the different experimental options available for in vivo measurements were investigated.
A feasibility study with available instrumentation was performed, concluding that diodes specifically designed for IVD in conventional external beam therapy and EBT3 type radiochromic films EBT3 are the most effective and accurate methods.
For TBI treatments at HHA, a Theratron Elite 80 Telecobalto therapy unit is used. For this purpose, it is necessary to locate the patient at an extended distance from the source, since the collimation system of the unit ensures a maximum field of only 35 x 35 cm at the isocenter(80 cm). Therefore, in the treatment room the conditions have been established to perform the irradiations at the extended distance of 350 cm, allowing a field size of up to 153 x 153 cm. The collimator is usually rotated 45º to achieve greater patient coverage so that patients with a maximal height of 200 cms, and in a lying position with lateral support, can be treated.
In the present work, 4 IVD diode probes, model VivoLog E5, were employed. They are designed for Co-60 and electron beam qualities, with an inherent build up material equivalent to 0.5 cm of water. They were connected to a multipurpose electrometer model PTW MULTIDOS, [5]. Data processing was performed with PTW "VivoSoft" application.
Type EBT3 radiochromic films were used in the present work [6] . The films were cut in small pieces of 2 cm x 2.5 cm each. The largest dimension of the piece coincides with the vertical direction of the film.
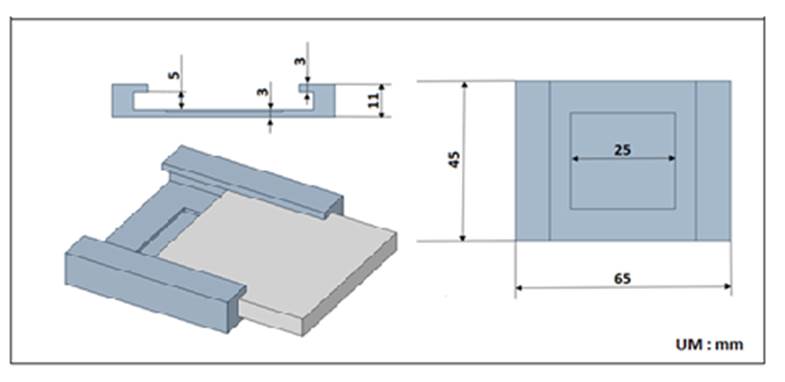
A support for the pieces of the EBT3 films was designed (figure 1), based on sheets of PMMA, which ensures the electronic equilibrium for Co-60, allowing adequate accommodation of the films on the patient, without deteriorating or contaminating the films.
The accuracy and precision required for this type of dosimetry with EBT3 films could be ensured, in addition to proper handling, by the use of a professional scanner for dosimetry. The reading (scanning) and dosimetric evaluation of the films were carried out using the computer applications provided by PTW applications for film dosimetry: FilmCAL, FilmScan, FilmAnalize.
To simulate the patient’s full anatomy, a “TBI” phantom was designed, combining different phantoms, in order to simulate the dispersion that occurs in real clinical situations. The head is composed of a fixed depth IBA acrylic phantom with insert for a Farmer type chamber. The thorax was represented by 25 cm of RW3 with sheet model 29672 / U7 that allows insertion of a Farmer chamber too. Finally, an in-house wax phantom, simulating the patient’s pelvis, was used. A picture of the TBI phantom is shown in figure 2.
Commissioning of the diodes for IVD in TBI.
The diodes to be employed had been discontinued of the IVD routine use for years; besides, they were integrated into a measurement system that was not tested for this kind of probes. Therefore, it was necessary to carry out an acceptance testing procedure, in order to verify the correctness of their functioning. Parameters to consider were: stability of the post-irradiation signal, linearity of the dose response and intrinsic precision. All these tests were performed for irradiation conditions similar to those found in the TBI practice.
The first step in the commissioning was to determine the calibration coefficient (N) for each diode, which is calculated using equation (1). Calibration refers to the combination of diode and electrometer, the change of either requires recalibration [2] .
|
Reference dose, determined from measurement with ionization chamber (Gy) |
|
Reading the diode (C) |
The response of Si diodes may change with the beam spectrum. Therefore, in order to determine the dose underneath the lung protecting blocks, where the radiation reaching the diodes is mainly produced by photons scattered in the patient and surrounding materials, it was necessary to measure a correction factor for the presence of this shielding.
For the determination of this correction factor, a Farmer type chamber was inserted in a solid water RW3 phantom, at the depth of maximum dose, in the blocked area. The diodes were subsequently placed at the entrance surface of the RW3 phantom, in the same blocker region as the chamber.
It was irradiated with a time of 10 minutes. The correction factor for the presence of blocking for each diode is calculated by equation (2):
Commissioning the radiochromic films system for IVD.
EBT3 films ware calibrated in term of entrance absorbed dose in water. They were placed on the surface of the RW3 phantom, inserted in the support described in figure 1, at a source-surface distance of 80 cm, with a 10 x 10 cm2 field.
Doses of 50.8 cGy, 144.5 cGy, 200.6 cGy, 251.5 cGy, 302.4 cGy and 500.4 cGy were imparted. One set of sheets was left unirradiated for background purposes. A waiting time of 16 hours was used for processing, thus allowing coloration to stabilize. Film calibration curve was obtained with PTW Mephysto’s Film CAL.
Test case for verification of the IVD system
Finally, before applying the in vivo dosimetry system to patients, an "end-to-end" test case was designed to check the reliability of the IVD system. The first step was to reproduce the conditions used in the TBI clinical practice at HHA. The TBI phantom described in figure 2 was used to simulate a patient. Using the AMEPLAN planning software, a typical dose per fraction of 225 cGy was prescribed to the phantom’s midline.
To measure the entry dose the different diodes and films were placed as shown in figure 2.

The measured doses were compared with that calculated by the TPS at different depths.
For measuring the exit dose, the detectors were placed in the corresponding position of the entrance dose, at the opposed side of the phantom. In these measurements, films were not used because they are not calibrated for these conditions.
Results y discussion
Commissioning of the diodes for IVD in TBI.
All diodes successfully passed the acceptance criteria to be used for IVD. A very important feature that was analyzed in detail was the stability of the post-irradiation dose. As recommended by the European Society For Therapeutic Radiology and Oncology, the dose percentage variation must be less than 0.1% [7] and for the four diodes, the percentage variation was better than that. Linearity, expressed in terms of the linear regression coefficient (R2) equalled one for all diodes. These results were compared with those obtained for other diodes reported in the consulted literature, [7] showing good consistency, which confirms its reliability. Regarding intrinsic precision, expressed by the standard deviation of repeated measurements, the highest fluctuation was 0.07%, well below the 1% tolerance recommended by the ESTRO [7].
Table 1 Calibration coefficients for IVD diodes and their block correction factors
| Diode | N ent (Gy/c) | N exit (Gy/c) | CFblock |
|---|---|---|---|
| 1 (1152) | -7,574·106 | -5,835·106 | 0,493 |
| 2 (1156) | -8,424 ·106 | -6,771·106 | 0,651 |
| 3 (1162) | -9,141·106 | -7,443·106 | 0,409 |
| 4 (1170) | -8,073·106 | -6,414·106 | 0,599 |
As expected, the calibration coefficient of the diodes were similar within a 20% (table 1), which indicated an adequate technical homogeneity in their design and that they were used previously with similar irradiation history. These values were stored in the Verisoft software.
If we analyze the correction factors obtained for each diode, we can deduce that blocking is a factor that significantly influences the response of the diode. The actual dose is almost 50% lower than that reported by the diodes in these conditions, because the diodes irradiated in blocking conditions receive essentially scattered radiation in the patient, whose effective energy is lower than the primary radiation, for which the sensitive material of the diode (Si) is more sensitive, due to its high atomic number with respect to water. This correction, therefore, cannot be ignored.
Commissioning the radiochromic films system for IVD.
As a result of the calibration of the EBT3 films, the entrance dose calibration curve was obtained.
Due to the limited availability of films and the lower sensitivity of the EBT3 film, it was decided to use this method only for entrance dose measurements. The calibration curve obtained should only be applied to determine the dose in vivo conditions, with irradiation configuration similar to that used during the calibration of the EBT3 films This means that, as in the case of this work, the method can be used for the evaluation of the entry dose. If this method is to be used for the output dose, a calibration curve should be obtained under these conditions.
Test case for verification of the IVD system
Table 2 Discrepanciesa of the dose measured at a depth of 0.5 cm in the test case
| Head | Chest | Pelvis | Thigh | |
|---|---|---|---|---|
| Diode | -2.4 | 0.5 | 3.7 | -9.7 |
| EBT3 | -4.3 | -1.6 | -0.7 |
a Discrepancies expressed as (Dose measures / Dose calculated by AMEPLAN) x100 %
The results showed that the doses measured by the EBT3 films along the central axis are in agreement with what is measured by the diodes, the average discrepancy value is around -2.7% (table 2). If we compare the doses measured in the thorax by the diode and the EBT film with respect to the measurement with the ionization chamber (located at the depth of the maximum dose) we obtain a difference of 1.6%and -0.5%, respectively. A better correspondence with the film is observed, but the differences are within the standard uncertainties of these detectors, so that a consistent advantage cannot be inferred from one detector with respect to the other, except the ease of use of the diode system.
According to the AMEPLAN planning program, the average maximum point dose (entry) should be 3.09 Gy for the analyzed case. If this value is compared with the doses measured in the different points of the TBI phantom, it is observed that in the most extreme points (head and thigh), the measured dose is lower than the prescribed dose, which can be associated to the fact that, in these areas, there is a lower contribution of the dispersion and greater distance to the measured point. In the thorax the difference is only 0.6%, as this point is in the center of the field where the dispersion conditions are more similar to those of the AMEPLAN calculation area and those of the calibration of the detectors. The weighted average of the discrepancies is equal to -6%, a value that serves as a reference to establish the action level for patient specific quality assurance purposes in IVD for TBI.
Table 3 Discrepanciesa between the measured dose and the prescribed midline in the test case.
| Head | Chest | Pelvis | Thigh | |
|---|---|---|---|---|
| Diode | 4.2 | -4.3 | 1.4 | 1.5 |
| EBT | 2.2 | -6.3 | -2.9 |
a Discrepancies expressed as (Dose measures / Dose calculated by AMEPLAN) x100 %
The prescribed dose to the midline was 2.25 Gy. As calculated, it varied from -6.3% to 4.2%, the areas where an underdose was obtained were those where the anterior-posterior dimensions of the phantom were less than the effective calculated by the program and the overdose where the opposite occurred (table 3). In this case, the weighted average of the discrepancies is 6.1%, which is very close to the previous case. This fact is a clear indication that there is a consistency in the results.
Table 4 Discrepancies of the dose measured at the exit with that prescribed in the test case
| Head | Chets | Pelvis | Thigh | |
|---|---|---|---|---|
| Diode | 28.7 | -13.6 | 4.3 | -12.2 |
The exit dose, calculated by AMEPLAN considering the prescribed dose and the depth dose curve, equalled 1.4 Gy. As it can be observed in table 4, there is a significant difference with the measured dose, which is mainly due to the fact that the depths of the points vary with respect to the depth value at which the dose was calculated. Previously, it was analyzed how the dose varies with the thickness, obtaining as a result that the entry doses are hardly affected, but the exit doses change considerably.
For all the above, the measurements of the dose at the exit, in our case, are not the best point for making the comparison of the doses in IVD for TBI irradiation control. Only the measurement of the exit dose in the area of the lungs should be performed, since they represent a great heterogeneity that cannot be correctly handled by AMEPLAN, unless a patient’s CT scan is available. In addition, estimating the value of the dose in the middle line only from the entrance dose introduces a great inaccuracy.
Conclusions
In the present work, an IVD system based on silicon diodes and radiochromic was commissioned and implemented as a tool for patient-specific quality assurance in TBI treatments. Calibration coefficients for entrance and exit dose were determined in the case of diodes; while films were used only for entrance dose verification purposes.
Based on the results of a designed end-to-end test case, it can be concluded that the proposed IVD system is an effective tool for the detection of possible gross errors or inaccuracies greater than 10% in the dose calculations for TBI. So far, with the calibration coefficients and correction factors obtained, it is advisable to implement IVD of TBI based on entrance dose both with diodes and EBT3 films, but the exit dose should be only considered with diodes.
As a result, a ± 10% action level was considered as a confident and realistic value for practical purposes in the clinical routine. The systematization of the IVD in patients to be treated with TBI will allow determining if it is necessary to relax or to make more rigorous this proposed level of action.

