










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
Permalink
Introduction
The induction of an immune response to infectious diseases via vaccination was the major contribution of Jenner and Pasteur to public health.1 Vaccines are a small amount of a weakened or killed virus or bacteria or bits of lab-made protein that imitate the virus to prevent infection by that same virus or bacteria.2 The vaccine stimulates the production of antibodies against the specific disease, which is termed immunization. Moreover, vaccination has reduced morbidity and mortality due to childhood infectious diseases.3
To control and eradicate infectious diseases, various immunization programs have been initiated globally. The Global Vaccine Action Plan (GVAP) was endorsed by the 194 member states of the World Health Assembly in May 2012. GVAP is a framework to prevent millions of deaths by 2020 through more equitable access to existing vaccines for people in all communities.4 The United Nations Children's Fund (UNICEF) also started an immunization program to cope with infectious diseases. In 2019, UNICEF reached almost half of the world’s children with life-saving vaccines. According to UNICEF statistics, 2.5 billion children have been vaccinated since 2000. Moreover, the number of children paralyzed by polio has fallen by more than 99% at the end of 2019.5
Pakistan is a developing country with a population of 220 million. Its estimated yearly growth rate is 2% and the infant mortality rate is 57.2 deaths per 1,000 lives births.6) In 1978, the Expanded Programme on Immunization (EPI) was initiated in Pakistan for immunization coverage against poliomyelitis, tuberculosis (TB), measles, diphtheria, pertussis and tetanus (DPT). Also, the current immunization schedules contain vaccines against hepatitis B (HBV), diarrhea, Hib pneumonia, and meningitis.7 The total estimated coverage in Pakistan for a fully immunized child varies between 65%-88% with considerable variation between provinces. The coverage also varies by the antigen, being the highest for BCG, DPT, and pentavalent vaccines including DPT, and HBV. The schedule administration time for the BCG vaccine’s first, second, third, and fourth dose is at birth, six, ten, and fourteen weeks, respectively. While for pentavalent vaccine doses are scheduled at six, ten, and fourteen weeks after birth.8 In terms of coverage, Pakistan is lagging as compared to regional countries such as Bangladesh and Sri Lanka. Pakistan is third among the countries with the most unvaccinated children.9 The common reasons for lack of immunization are inadequate health infrastructure, un-accessibility, lack of awareness and education, and lack of serious policy implementation. Moreover, the lack of motivation of EPI staff, lack of accountability and lack of private sector involvement are the major barriers that lead to poor vaccination coverage.10)
The Pakistan Polio Eradication Program has been fighting to end the crippling poliovirus from the country since 1994. This program is driven by up to 260,000 polio vaccinators, quality data collection and analysis, state-of-the-art laboratories, epidemiologists, and public health experts of Pakistan and the world.11 This program is currently implementing the National Emergency Action Plan (NEAP) for Polio Eradication 2020. As per the NEAP 2020, the program is committed to stopping wild poliovirus type 1 (WPV1) and vaccine-derived poliovirus type 2 (VDPV2) transmission in Pakistan. This country is still fighting against this virus, as in 2020, 84 WPV and 83 cVDPV2 polio cases were reported.12
It has been seen that vaccination coverage is better among the educated population as compared to uneducated/illiterate and religious groups.13 But still, most of the educated strata show an anti-vaccinating attitude concerning fear of vaccine side-effects and need for more information about the risk of vaccination and the belief that they are not at risk. In Pakistan, various studies have been conducted on vaccination status and barriers among children, parents, and the general population as focus groups.14,15) The student's strata have remained less touched and have not been studied in detail.
In Pakistan, the immunization rate is not up to the mark, only about 2/3rd of children get complete vaccination coverage. Many fatal diseases are preventable if EPI is made accessible for all. In 2013, around 14 thousand cases of measles were reported that resulted in 306 deaths. While, in 2019, 53 new polio cases were documented, a higher number than in the past 3 years.9) Keeping these facts in mind, the current study was conducted to determine the vaccination status and barriers to vaccination among University students of Southern Punjab, Pakistan.
Material and Methods
Study design, setting and duration
The quantitative-cross-sectional study design was used for the current study that was conducted in Bahauddin Zakariya University (BZU), Multan and was completed between 10th February and 5th of March, 2020.
Study population and sampling technique
The study population consisted of students that enrolled in BZU. Currently, there are thirty thousand enrolled students in BZU, the public sector university that enrolls students from all over Pakistan (open merit and reserved seats) and foreign including Nepal, Indonesia, Yemen, and Palestine under foreign seats. The sample size was 380, calculated by Raosoft® sample size calculator. A simple random sampling method was used for this study. The international students were excluded from the study as they were less in number.
Study instrument validation and data collection
The initial draft of the questionnaire was prepared after a literature review.14,15 This draft was then sent to the profession from medical background to assess the relativity and simplicity. To check the internal consistency, a pilot study was conducted on 32 participants. The Statistical Package for Social Science (SPSS) v25 (IBM Corp., Armonk, NY, USA) was used and a Cronbach alpha value of 0.71 was obtained which indicates valid internal consistency. The final draft of the questionnaire was comprised of data related to demographics, history of childhood infection, vaccination status, and barriers to vaccination.
The questionnaires were distributed among the students, through simple random sampling, along with attached informed consent. The knowledge and vaccination status responses were collected on a “yes” and “no” basis. The signed informed consent was collected from each participant.
Ethical consideration
The current study was conducted following the Declaration of Helsinki. The study was reviewed and approved by the ethical committee of the Department of Pharmacy Practice, Faculty of Pharmacy BZU, Multan, Pakistan (Reference No: Acad/PRAC/18-22/26). Throughout the study, participants' confidentiality was maintained and ensured.
Results
A total of 380 participants were recruited in the study, amongst which 97.9% of participants were fell in the age range of 18-25 years. Most participants were male (86.3%), and the majority of the participants were enrolled in undergraduate programs (86%). More than half of the participants were from rural areas (58.2%). Regarding monthly income status, most of the participants were fell in the lower middle class (36.8%) followed by the high middle class (25%) and lower class (22.1%). The demographic data of respondents is given below in Table 1.
Table 1 Demographic characteristics of the participants
| Frequency | Percentage | ||
| Age | 18-25 | 370 | 97.9 |
| >25 | 8 | 2.1 | |
| Gender | Male | 328 | 86.3 |
| Female | 52 | 13.7 | |
| Department/Faculty | Pharmaceutical sciences | 147 | 38.7 |
| Biological sciences | 127 | 33.4 | |
| Social sciences | 83 | 21.8 | |
| Management sciences | 23 | 6.1 | |
| Program | Undergraduate | 326 | 86.0 |
| Postgraduate | 53 | 14.0 | |
| Social Status | Urban | 221 | 58.2 |
| Rural | 159 | 41.8 | |
| Monthly Income Status | Lower Class (PKR 4000-20,000) | 84 | 22.1 |
| Lower Middle Class (PKR 21,000-40,000) | 140 | 36.8 | |
| Middle High Class (PKR 41,000-60,000) | 95 | 25.0 | |
| High Class (PKR >60,000) | 61 | 16.1 |
In this study, 23.9% of the participants had a history of childhood infections like polio, measles, etc. Regarding vaccination status, the majority of the participants were immunized against polio (97.1%), TB (58.7%), hepatitis (44.2%), DPT (49.2%), and measles (55.3%). The barriers to vaccination were unwillingness (15.0%), inaccessibility (17.10%), financial issues (4.47%), and unawareness (63.42%). Moreover, 31% of the participants considered that the vaccine is unsafe. The detail of knowledge about immunization, the history of infectious disease, and barriers are given in Table 2.
Table 2 Responses of the participants to the history, vaccination status, and barriers to vaccinations.
| Frequency | Percentage | ||
| History | |||
| Do you have any past family history of polio, diphtheria, measles, tetanus, T.B, or any other childhood infectious disease, etc.? | Yes | 91 | 23.9 |
| No | 289 | 76.1 | |
| Vaccination status | |||
| Have you been vaccinated with the Polio vaccine? | Yes | 369 | 97.1 |
| No | 11 | 2.9 | |
| Have you been vaccinated with BCG (a vaccine against TB)? (You can look for the scar mark on your right forearm (deltoid muscle). | Yes | 223 | 58.7 |
| No | 157 | 41.3 | |
| Have you been vaccinated with the hepatitis B vaccine? | Yes | 168 | 44.2 |
| No | 212 | 55.8 | |
| Have you been vaccinated with DPT (diphtheria, pertussis and tetanus vaccine? | Yes | 187 | 49.2 |
| No | 193 | 50.8 | |
| Have you been vaccinated with the measles vaccine? | Yes | 210 | 55.3 |
| No | 170 | 44.7 | |
| Barriers to vaccination | |||
| Which of the following do you consider for being Unvaccinated? | Unawareness | 241 | 63.4 |
| Unwillingness | 57 | 15.0 | |
| Un-accessibility | 65 | 17.1 | |
| Financial issues | 17 | 4.5 | |
| Do you consider that vaccine is un-safe | Disagree | 212 | 55.8 |
| Undecided | 50 | 13.2 | |
| Agree | 118 | 31.0 |
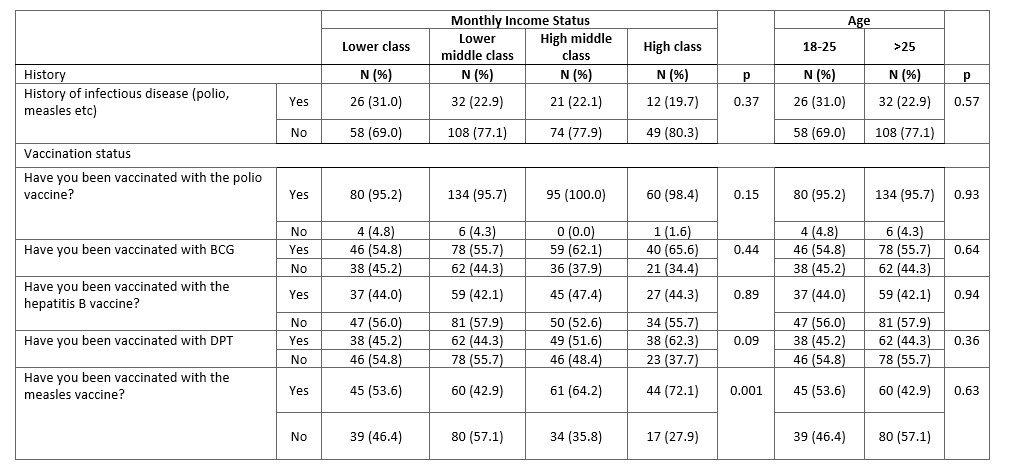
Regarding knowledge about vaccination, a significant difference was seen across the program as undergraduates had more knowledge as compared to postgraduate (p = 0.04). The rural participants were more immunized against TB (p = 0.006) and DPT (p = 0.001) in comparison with urban participants. The association of demographics with knowledge about vaccination, history of infection, and vaccination status can be seen in Table 3 and Table 4.
Table 3 Impact of demographics (independent variables) on knowledge and vaccination status (dependent variables).

Table 4 Impact of demographics (independent variables) on knowledge and vaccination status (dependent variables).
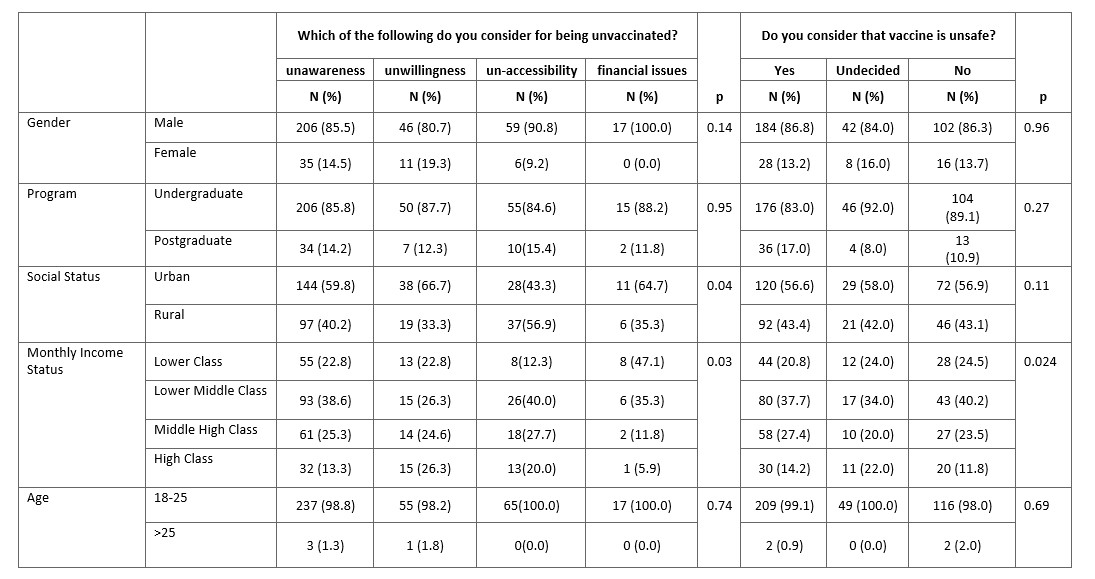
In the study was seen that unawareness, un-accessibility, and financial issues were the common barriers in lower-class and middle lower-class of the participants (p = 0.03). Moreover, the unsafety of the vaccine was considered as a barrier by the middle lower-class in the current study (p = 0.02). The association of barriers with demographics can be seen in Table 5.
Discussion
The current study was conducted to assess the vaccination status and barriers to vaccination among university students. It was seen that more than half of the participants were un-immunized against hepatitis, DPT, and almost half of the participants were being unvaccinated for TB and measles. Moreover, unawareness, un-accessibility, financial issues and wrong perception about vaccines were the most prominent reported barriers in the current study.
Pakistan is still fighting against polio as the majority population shows anti-vaccinated behavior mainly due to unawareness and misconceptions about vaccination. The WHO, UNICEF and other concerned bodies contribute major efforts to eradicate infectious diseases like polio, measles, etc.16,17) As reported by the WHO most of the countries are polio-free but Pakistan is still fighting against this infectious disease (6 It was seen in the current study that almost half of the participants were not vaccinated for the vaccine-controlled infectious disease. But the polio-vaccination status was high as compared to other listed vaccines in the current study, which is mainly contributed to the efforts of Pakistani’s health regulatory authorities that try to make Pakistan polio-free in collaboration with WHO. However, the frequency of vaccinated participants in the current study was lower than the reported study from Karachi18 and Lahore.6 This low vaccinated profile highlighted that an intensive and compulsory vaccination program should be started to increase the coverage of the recommended vaccines.
It is well established that religious extremism and terrorist activities are mainly contributed to the anti-vaccinated behavior in Pakistan and neighboring countries.14,19 Also, in the current study, it has been observed that unawareness and the perception about vaccine un-safety were the major reasons for being unvaccinated.16 In Pakistan, the majority of the population is in favor that vaccination cause immodesty and it is a ploy against the Muslim world, which is the major reported myth about vaccination. Therefore, it is a need of time to initiate focused awareness programs regarding vaccination by using social, print, and electronic media. The university administration can increase the acceptability of vaccines among the students by highlighting their benefits with on-campus-focused educational activities. Moreover, it is recommended that focused policies should be designed and implemented to address the religious barriers to vaccination. It is imperative to teach the importance of vaccination in schools. Public confidence in vaccination is important to maintain vaccination coverage rates and preventing outbreaks of vaccine-preventable diseases. Some parents may be hesitant to vaccinate their children; this issue can be addressed by implementing parent/guardian specific educational interventions at community levels.
Higher socioeconomic status and education level positively influence the immunization rate, as confirmed in other studies.20,21 Consistently, it has been observed in the current study that the lower-middle class participants considered vaccine safety as a barrier to vaccination. A cross-sectional study from Pakistan showed that the participants who fell in the monthly income range of 5,000-10,000 (PKR) were significantly associated with non-immunization.21) Moreover, the urban participants reported unawareness as a major barrier to non-immunization. This study was consistent with the previous report.22
Limitation
The current study is subjected to various limitations. Firstly, the recall bias may affect the participant's responses regarding vaccination status. Secondly, the participants of the current study were literate, therefore it cannot be generalized to the illiterate population.
Conclusions
The coverage of polio vaccination was good but there is low vaccination coverage of BCG, DPT, HBV and measles vaccine among students. Unawareness was the most common cause of poor vaccination status. Moreover, the prevalence of myths among the university students about the un-safety of vaccination is alarming, as they are educated strata of the general population. Therefore, the concerning authorities and policymakers should devise strategic and focused policies like awareness programs in education sectors including schools, colleges and universities, door to door awareness campaigns in areas where the population shows anti-vaccinated behaviors due to unawareness to increase the vaccination coverage. Also, a compulsory vaccination program should be started and supported by the regulatory authorities.

