










 Servicios personalizados
Servicios personalizados Español (pdf)
Español (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Schizophrenia is a complex chronic psychotic disorder that shows a significant morbidity and mortality, associated whit multiple biological, psychological, socio-familiar and environmental factors. The evolution of this mental illness tends to be heterogeneous and with great compromise of the individual's functionality. For this reason, the nature of its prognosis is multidimensional. This condition generates uncertainty at the time of its diagnostic.1
In the Diagnostic and Statistical Manual of Mental Disorders Fifth Edition (DSM-5), the American Psychiatric Association1) proposed that between 0.3% to 0.7% of the global population have schizophrenia. However, variations are observed, associated with school level, ethnicity, and geographical area of origin, country and socioeconomic development. There are also differences related to sex, not so much in the proportion, but in the clinical manifestations and the evolution of the disease.
The World Health Organization2) reports that this psychiatric condition is one of the ten most disabling diseases worldwide, being considered the worst disease that affects humans. However, it is likely that this psychopathological entity encompasses a group of disorders with heterogeneous etiologies and time of onset, evolution, and therapeutic responses that vary widely from one patient to another.
The current diagnosis of schizophrenia, according to the DSM-51 and the ICD-113 is based on the presence of alterations in thought, perception, emotions, volition, awareness of self, motor behavior, cognition and oral communication. This illness is characterized by a wide variability in their clinical manifestations, which are organized into Positive symptoms, Negative symptoms and Cognitive symptoms. Positive symptoms include delusions, hallucinations and thought disorder. Cognitive symptoms include decreases in declarative memory, working memory and other executive functions, slower processing speed, social cognition deficits, etc. Negative symptoms include diminished emotional expression or avolition and disorganized speech.4,5
However, as is described in the DSM-51 among the most common symptoms of schizophrenia, oral communication disorders stand out. Such alterations of oral communication are manifested fundamentally as disorganized language that is part of the disorganized dimension of the negative symptoms of the disease.6,7 Associated to the disorganized language, the patient show a ramble wandering oral speech, full of paraphasias and neologisms, with various forms of destructuring. The patient can dissociate himself from the subject and respond incoherently to his interlocutor. The usual bizarre discourse, full of neologisms, can decline in a marked communicational deterioration.8,9
The degradation and disorganization of oral communication that takes place in schizophrenia are markedly nonspecific and variable, both in their clinical manifestations and at the time of presentation. This disorganization of oral communication can be markedly severe in the most acute moments of crisis, or they may appear in a less severe form during the prodromal and residual periods of the disease. During these periods, it manifests itself similarly to the oral discourse showed by patients with Wernicke's aphasia.10,11
Wernicke's aphasia is characterized by the presence of deficit in oral comprehension, with different levels of severity. In extreme cases, the patient simply does not understand anything. In less complex cases, the patient can understand simple words or phrases. In most cases, the patient understands several words when presented. Even so, when the number of words increases, it does not achieve an additional understanding.12
However, although the main defect in Wernicke's aphasia is in oral comprehension, the patient's oral production manifests a relative absence of content words, which implies a decrease in the significance of the speech. For this reason, such patients tend to show a semantically insubstantial oral discourse, characterized by incoherent loquacity, with an excess of words that reaches logorrhea. The grammatical structure may be adequate, although it is common that it contains an excess of grammatical morphemes. In addition, they show a notable amount of paraphasias, which can be literal, verbal and even grammatical. Neologisms are also very frequent.12
In essence, patients with Wernicke's aphasia show a semantically empty oral discourse, full of paraphasias and neologisms, similar to the oral discourse of schizophrenic patients. Even so, despite the similarity of oral discourse between both types of patients, it is assumed that the etiological factors that underlie their alterations in oral language production are different. This, even when is inexistent a unitary or definitive criterium about etiological factors in schizophrenia.13 However, a big question arises: Are the cognitive mechanisms underlying such alterations in oral language production different in both types of patients?
In the case of Wernicke's aphasia, oral speech disorders are an expression of deficit in cognitive components and mechanisms for oral language processing, which have been generally affected because of focal brain damage. This issue has been widely addressed by cognitive neuropsychology and neurolinguistics in recent decades. In this regard, abundant empirical evidence has been reported.11) However, in the case of schizophrenia, several authors have been considering that the alterations of the oral discourse that are registered in this psychiatric disease are the secondary expression of alterations of thoughts. In that case, it would not be harm to oral language processing itself.13
In a study conducted by Omar, et al.14 a comparative analysis of the performance in neurocognitive and neurolinguistics tests of Wernicke's aphasic patients and schizophrenic patients was made. However, the results were insufficient to discuss the nature of deficits for verbal communication in schizophrenia. The empirical evidence obtained about the cognitive mechanisms underlying the alterations of verbal communication in both types of patients was biased, among other reasons, by the type of tests used for neurocognitive assessment and the types of statistical analyses performed.
Therefore, a second study was implemented, in which the limitations of the first research were transcended. The present study was designed to identify the cognitive mechanisms underlying oral communication disorders in schizophrenic patients, relying on the comparative analysis of its performance in neurocognitive tests for semantic exploration and oral language production, with the execution of patients with Wernicke's aphasia in the same tests.
Method
Type of study and participants
A descriptive correlational studywas performed, with a non-experimental cross-sectional quantitative design. Two groups participated: a group of schizophrenic patients (GSP) and a group of aphasic patients (GAP).
In the GSPwere included 35 patients with a diagnosis of residual paranoid schizophrenia. The 88.6% were male, while the 11.4% was female (mean age 42.66 years, SD=4.64, with a minimum of 33 years and a maximum of 56 years). The schooling was basic in the 14.3%, secondary in the 48.6%, and higher in the 37.1% (mean schooling 11.9 years, SD=3.23, with a minimum of 8 years of study and a maximum of 17 years of study).
In the GAPware included 35 patients with a diagnosis of Wernicke's aphasia. The 70.3% were male and the 29.7% female. Mean recovery time of brain damage was 64.7 days, SD=19.26, with a minimum of 30 days and a maximum of 90 days. Mean age 49.73 years, SD=11.21, with a minimum of 28 years and a maximum of 70 years. The schooling was basic in the 13.5%, secondary in the 59.5%, and higher in the 27.1% (mean schooling 11.4 years, SD=4.37, with a minimum of 9 years of study and a maximum of 17 years of study).
Hypothesis and variables
For the execution of the study, the following research hypotheses were considered:
Hy-1.The conservation status of semantic processing and the record of semantic paraphasias that show GSP is similar to the conservation status of the semantic processing and to the record of semantic paraphasias shown by GAP.
Hy-2. The processes of lexical concepts activationat the semantic system level are significantly more conserved in GSP than in GAP.
Hy-3. The processes of lexical activation for oral denomination at the linguistic processing subsystem level are significantly more conserved in GSPthan in GAP.
Hy-4.The record of phonologicalparaphasias and grammatical paraphasias is significantly more frequent in GAP than in GSP.
Hy-5. The record of neologismsis significantly more frequent in GSP than in GAP.
Hy-6. The record of semanticparaphasias in GSP is similar to the registry of semanticparaphasias in GAP.
Based on these research hypotheses, the following Variables were considered: (1) Semantic processing, (2) Activation of lexical concepts, (3) Lexical activation for the oral denomination, (4) Phonological paraphasias, (5) Grammar paraphasias, (6) Semantic paraphasias, and (7) Neologisms.
Methods for obtaining data
Obtaining the data for the empirical verification of Research Hypothesiswas performed using the following test:
Semantic Image Matching Test:to explore the conservation, activation and recovery status of conceptual and categorical representations in the Semantic System.
Homonymous Image Identification Test: to explore the activation of lexical concepts and the access to the phonological output lexicon from the semantics, without the participation of the sequencing planning of phonemes for the articulation.
Oral Denomination Test of Images: to explore the lexical activation for oral denomination from the semantics and planning processes of the phoneme sequence for articulation.
Picture Arrangement Test of the WAIS-R-NI: to stimulate spontaneous language to identify the presence of phonological paraphasias, grammatical paraphasias, semantic paraphasias, and neologismsin the speech.
Procedures for data analysis
For the computational processing of the data, the Statistical Package for Social Science (SPSS.21.0) was used. The previous descriptive analysis of each of the variables involved the calculation of mean, standard deviation and range. The statistical analysis of data to submit the research hypothesis to verification involved the use of the Student’s t-test, with p <0.01, and the calculation of itscorrespondingeffect size, according to Hopkins’ criteria.
Ethical procedures and informed consent
For the implementation of the study, theStatement of Ethical Principles for Medical Research in Human Beingsof the World Medical Association were observed. Access to the participants of each group was supported by collaboration agreements between researchers and the corresponding health institutions. The participants were informed about the objectives of the study and the voluntary and anonymous nature of their cooperation. All signed informed consent for participation, supervised by the Ethics Committee of the institution.
Results
Table 1shows the data of mean, Standard deviation, and range (Minimum and Maximum),errors recorded by the participants of both groups in each of the variables considered in the study, based on the research hypotheses formulated. These data generally indicate that despite the marked interindividual variability registered in all participants, the GAP showed marked difficulties in the linguistic variables, compared to the GSP. Meanwhile, the performance in the semantic variables was similar in both groups.
Table 1 Mean, Standard deviation, and range of the failures of each group in each of the study variables
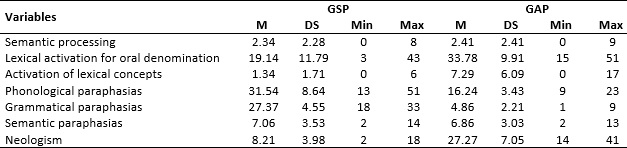
M: Mean; DS: Standard deviation; Min: Minimum; Max: Maximum.
The conservation status ofsemantic processingshown by the GSP was similar to the state of conservation of semantic processing shown by GAP patients. Similarly, the record of semantic paraphasiasin the GSP is similar to the record of semantic paraphasiasin the GAP.
For its part, the processes of lexical concept activation at the level of the semantic system, as well as the processes oflexical activation for oral denomination at the linguistic processing subsystem level, are more conserved in GSP patients than in GAP patients.
In the case of phonologicalparaphasias and grammatical paraphasias, these are more frequent in GAP patients than in GSP patients.However, the record of neologismsis more frequent in GSP patients than in GAP patients.
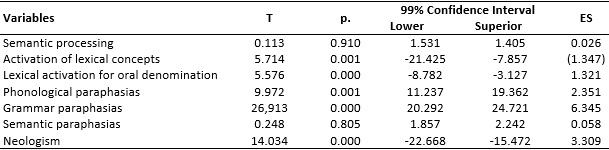
The differences in the values obtained for each group of patients in the linguistic variables are statistically significant. Well, the values of Student-t, with GL=70, indicate that the Lexical activation for oral denomination, the Activation of lexical concepts, the Phonological paraphasias, the semantic paraphasias, as well as neologisms, show statistically significant differences between both groups (see Table 2).
Discusion
Since the 70s of past century, many authors pointed out that in schizophrenia, the deficit of thought was manifested clinically as language disorders, but language was not really affected. Other slightly more recent authors have also expressed this point of view and have carried out some studies in this regard, from which they have reached favorable conclusions about the non-linguistic origin of oral speech disorders in schizophrenia.15
However, this perspective contrasts with opposite views, where some authors strongly defend the linguistic origin of oral discourse alterations in schizophrenias.16 This is widely expressed in a work published by Dörr17 who states that schizophrenias are forms of speech disorders and based on his point of view of the matter, he develops a whole theory about the genesis of schizophrenia, placing in linguistic functions, the origin of all the alterations of this mental illness, including obviously, alterations of oral communication. This work, although in several aspects lacks scientific approaches and enters into absolutely speculative planes, has been positively considered by many authors, it gives the measure that many ambiguities persist. In fact, the current scientific literature very often is not very precise when this issue is addressed.18) Expression of the latter is the hot debate starred by Palaniyappan, Du, Zhang & Feng19about the genetic determinants of language network dysconnectivity in drug-naïve early-stage schizophrenia, and the historical pursuits of the language pathway hypothesis of this illness.
In a review of the Diagnostic and Statistical Manuals of Mental Disorders, DSM-IV,5 of the International Classification of Diseases, ICD-10, in its chapter F of Mental Disorders and Behavior,6 and other literature, there were references to language disorders in schizophrenia, associated with both positive symptoms and negative symptoms of the disease. In all cases, it remains in the background that such alterations in oral discourse are secondary to thought alterations. However, they are referred to as language disorders.
In the new edition of the Diagnostic and Statistical Manual of Mental Disorders, the DSM-53 references to speech disorders are found (speech) in schizophrenia, which are shown as the way to express the characteristic disorganized thinking of these patients; the term "language" is not used (language). In the Spanish edition of the DSM-53 the term “speech” is used all the time, subordinated to disorganized thinking, and even refers to the similarity between discourse in schizophrenia and disorganized discourse characteristic of sensory aphasia (Wernicke).
This is an important advance, because finally the alteration of language is explicitly distinguished as a secondary symptom to the alteration of thought and is broken to some extent with the entrenched idea of language alteration as a symptom of schizophrenia. Even so, it is still relevant to base, relying on solid and abundant empirical evidence, the non-linguistic nature of oral communication disorders in schizophrenia.14 That is why it is necessary to elucidate the cognitive mechanisms that are at the base of verbal communication alterations in schizophrenia.
This study was conducted with three fundamental intentions. First, to obtain empirical evidence on the cognitive mechanisms that underlie the alterations of verbal communication in aphasic and schizophrenic patients, from the analysis of their execution in neurocognitive tests for the exploration of thought, and the oral production of language. Second, to analyze comparatively the execution of both types of patients in the referred tests. Third, to discuss the nature of deficits for verbal communication in schizophrenia, based on its analysis from a neurocognitive approach.
The empirical evidence on the cognitive mechanisms that underlie the alterations of verbal communication in both types of patients were obtained, and are widely shown in the results.
The data show that disorders for verbal communication in schizophrenic patients do not respond to neurolinguistic alterations properly, their performance in linguistic tasks was above the norm. In the case of aphasic patients, the disorders for the production of language they manifest areproper neurolinguistics alterations. This is the case because their performance in linguistic tasks was affected at different levels, apart from not only the frequent interindividual variability, but in addition to the fact that in this type of aphasia, the fundamental deficit is for the understanding of language, not for its production.
These data show empirically that the alterations of verbal communication in schizophrenia do not have a linguistic nature. However, they are not enough to affirm that they are secondary to alterations of thought. Well, the applied tasks do not explore thought functions in depth, they are only limited to exploring basic semantic processing.
However, this does not rule out that these patients show alterations in the processes of abstract concept formation and categorization; since as evidenced in the results, the execution was worse as the concepts that were appealed with the items of the task used were more abstract.
This data is consistent with other evidence. In the function of activating lexical concepts for oral production, even at a semantic level, schizophrenics show conservation levels. However, the possibility of failures at this level increased to the extent that the word to be produced moved away from basic concepts. This happened even when, from the articulatory point of view, the word was simpler; which indicates that the problem is semantic, not linguistic.20
The comparative analysis in the execution of both types of patients, in the referred neurocognitive and neurolinguistic tests, is also widely shown in the results. In this case, the non-linguistic nature of the alterations of verbal communication in schizophrenia is corroborated. But in addition, as an interesting fact, an important distinction is obtained between the forms of presentation of the paraphasias and the neologisms in both types of patients.
As expressed in the results, the presence of phonological and grammatical paraphasias in aphasic patients was recorded. These were scarce in schizophrenics, which preserved levels of lexical and syntactic functions. On the other hand, in these last group, a high number of neologisms were registered, which was not evident in the case of aphasics.
For the neologisms that some aphasic patients showed, if their structure is analyzed, it could be affirmed that they result from a problem of activation of rules for the derivation of grammatical morphemes. They could be considered rather a form of paragrammatisms, which are common in the presence of production aphasias, but they refer little to the aphasias of understanding.
Unquestionably, the empirical evidence shown is enough to affirm that the alterations in verbal communication that patients with schizophrenia register are not linguistic in nature.
For an idea or an intention, to become a verbal message, first, this idea or intention must be generated from the adaptive demands of the environment, and activate at the level of the semantic system, the concepts related to the message in question. Then they activate, even at the semantic system level, the lexical concepts corresponding to the concepts referred to in the message, including information about the thematic roles.
Once the lexical concepts are activated, the process of verbal coding of that message begins, already at the linguistic level. As a result, a functional argumentative structure is developed, with information on who does what to whom. This phonological and syntactic information is activated at a positional level (the place that each word occupies in the sentence), where the syntactic structure of the sentence is activated. During this positional level, the phonological forms of the words are activated and assigned to their corresponding positions. Subsequently, the phonemic elements of the phonological form of the words are sequenced and stored in the phonological seal, while the corresponding articulatory plans are activated.
This way in which information is processed for coding as a verbal message delimits, prior to linguistic processing, a level that is properly thought. If, at this level, adequate mental representations are not produced when the verbal message is being encoded at the linguistic level, this message will express those inappropriate representations.
This is precisely what is assumed to happen in patients with schizophrenia. Some authors who have addressed the issue21 suggest that, in these patients, language is difficult to achieve, given the distortions of thought that they usually present. It was shown that, in the first stage of the disease, the discourse is usually vague and disorganized; subsequently, in phases associated with chronicity, it becomes more acute. In essence, these difficulties are considered as consequences of formal thought disturbances.22,23
Although this is an issue that has not been sufficiently addressed, there are currently two positions regarding the relational link between thinking and language in schizophrenics. On the one hand, there are those who believe that language problems may be associated with problems of concrete thinking, given the difficulty in handling abstract concepts. Meanwhile, on the other hand, there are those who focus their interest on pseudoscientific ideas.
The truth is that it coincides in schizophrenic patients with the lack of connection between the ideas expressed, what is called lax associations. The relationships between ideas may seem illogical or deviate from the original theme. In extreme cases, lax associations lead to totally incoherent thinking and discourse. It could be said that in these cases, it is possible to find alterations in the course of thought, such as acceleration, inhibition or blockages.23,24,25
Conclusions
In general, in the schizophrenic patient, there is disorganized thinking, characterized by loss of the guiding idea and rupture of normal associations. This difficulty is evident through discourse that becomes frayed, changing from one topic to another and does not have a definite objective. This process is known as tangentiality, and it occurs because the patient makes lax associations (associating objects or facts with each other, which really have nothing in common), so that his speech sounds illogical.
That is why the mental representations that are activated as part of the processes that take place in this altered thought, once they are encoded as a verbal message, do not express more than those thought alterations. Such reasoning is fully consistent with affirmation that in schizophrenia, there were alterations of thought that were expressed verbally with all the ease that the very nature of these alterations of thought allowed.

