










 Serviços customizados
Serviços customizados
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Introduction
The coronavirus disease 2019 (COVID-19), caused by the new severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), emerged in Wuhan, China in December 2019.1 It was declared a global pandemic in March 2020, today with more than 93 million confirmed cases and more than 2 million deaths. In Qatar, the figure is 147 089 to date, with 246 deaths.2
Some authors describe risk factors for death and unfavorable evolution in patients with COVID-19 such as age, chronic respiratory and heart disease, diabetes mellitus, cancer, hematological neoplasia, liver disease, etc.3,4
According to research, angiotensin-converting enzyme 2 (ACE 2) is shared as a receptor for SARS-CoV and SARS-CoV-2 viruses, both of which are mainly spread through the respiratory tract. Person-to-person aerosol transmission is definitely the main source of contagion although transmission through contaminated hands or surfaces has also been described.5 The mean incubation period is between 2 and 12 days (median 5.1 days).6,7,8,9
In the diagnosis of the disease, RT-PCR, a laboratory test that uses samples of nasal swabs, tracheal aspirates, or bronchoalveolar lavage (BAL) is used to detect the virus. The preferred route for collecting samples from the upper respiratory tract is nasopharyngeal and oropharyngeal swabbing.10,11
Among the two most common laboratory findings recorded on admission in hospitalized patients with pneumonia due to COVID-19 we can mention leukopenia (9-25 %) or leukocytosis (24-30 %), lymphopenia (63 %), levels of elevated alanine aminotransferase and aspartate aminotransferase (37 %) in addition to the alteration of C-reactive protein, neutrophil/lymphocyte index and the highest levels of D-dimer that are related to complicated COVID-19 and death.12,13,14
Several studies validated the use of the first chest X-ray severity index (CSE-chest-severity-score) as an indicator of poor prognosis. These results reaffirm how COVID-19, despite its many non-respiratory manifestations, is primarily a primary pulmonary disease. Changes in the parenchyma can be evolved on the chest radiograph, since opacification is the main indicator of the disease progression.15,16,17,18,19
The Cuban Hospital in Qatar is one of the institutions that exclusively treats patients infected by COVID-19 with a significant influx of patients referred from isolation centers. Despite this, no study that validates the use of the clinical, radiological, and humoral variables related to the unsatisfactory evolution and indicator of the severity of these patients has been recorded.
Framed in the current situation of the pandemic and based on current knowledge, the present investigation was carried out with the objective of determining the predictive value of clinical, radiological, and humoral variables related to unsatisfactory evolution in young and middle-aged patients infected with COVID-19.
Material and Methods
An observational, retrospective and case-control study was carried out on a universe of 484 patients infected by COVID-19 admitted to the Cuban Hospital in Qatar between March and July 2020.
Hypothesis: Radiology and clinical variable are good predictors of poor outcome in young and middle-aged patients with COVID-19 disease.
Null hypothesis: There are no clinical and/or radiographic variables capable to predict the poor outcome in patients with COVID-19 disease.
Alternative hypothesis: There are clinical and/or radiographic variables capable to predict the poor outcome in patients with COVID-19 disease.
The sample of 60 patients was calculated with the OpenEpi online software, following the parameters: two-tailed test, 95 % significance level, 80 % detection probability power, 2:1 ratio of controls per case, the hypothetical proportion of controls with exposure 40, the hypothetical proportion of cases with exposure: 80.52 Odds Ratio to be detected 6.20. 13. For this, 20 cases and 40 unpaired controls were selected using a simple random probabilistic method for both groups. When necessary, an excluded individual was replaced by another with inclusion criteria, using the same method.
Inclusion criteria have a positive TR-PCR test, an X-ray study, and a leukogram the day of admission before its complication. The workers of the Hamad Corporation were excluded.
Definition of cases: patients with respiratory failure who required invasive ventilation (FiO2> 60, SpO2 <92 %) or death (permanent, irreversible cessation of all biological functions that sustain a living organism), with a hospital stay of more than 10 days. Controls: patients who followed the regular course of the disease, without any complications described, until discharge.
The data of the images were the result of the blind evaluation of the first chest X-ray, carried out by two second-degree specialists in Radiology, members of the research team.
Clinical and laboratory information was collected from the patient's digital medical record by a team participant. For the collection of all the information, individualized data collection sheets were used (emptied into an Excel document for statistical processing), linked by a unique code to preserve the privacy of the patients studied. The data were processed using SPSS version 25 statistical software.
The bioethical aspects were treated following the declaration of Helsinki. The use of the informed consent was not necessary. The primary data will be archived for a period of 5 years, then it will be erased and destroyed.
The outcome used was the clinical evolution, dichotomized into satisfactory evolution (patients who followed the regular course of the disease, without any complications described until discharge) or unsatisfactory evolution (patients with respiratory failure who required invasive ventilation (FiO2> 60, SpO2 <92 %) or death [permanent, irreversible cessation of all biological functions that sustain a living organism], with a hospital stay of more than 10 days).
The demographic input variables used included: age measured in completed years, then converted into qualitative, divided into age group 20-30, 31-40, 41-50, 51-60, 61-65. Gender: female or male. Nutritional status for which the body mass index (BMI) measured in kg / m2 was used, then characterized according to the WHO as: underweight <18 kg / m2, normal 18-24.9 kg / m2, overweight 25- 29.9 kg / m2, obese 30-39.9 kg / m2 and morbid obesity more than 40 kg / m2. Leukogram according to its value and converted into qualitative, dichotomized: normal between 4x103 u/L and 10x103 u/L or abnormal <4x103 u/L > 10x103 u/L. Comorbidities divided into absence of comorbidities, presence of one comorbidity, and presence of two comorbidities. Specific comorbidities (diabetes, high blood pressure [HBP]). The severity index of the initial chest X-ray (CSE) which was divided into 6 quadrants using vertices, bases, and hila as limits.15 It was dichotomized in 0-1 quadrant affected or 2-6 quadrants affected, based on the amount of affected quadrants by condensation or some radio-opacity detected in the initial chest x-ray. (Figure 1)

In the univariate analysis, frequency tables were used for qualitative variables and the mean and standard deviation for quantitative variables.
In the bivariate analysis, the Chi-square test was used, p values below 0.05 were defined as significant.
The multivariate analysis was built using the variables resulting from the Chi-square tests with p values below 0.1. Binary logistic regression was carried out using the forward step of the Wald method, with p values less than 0.05 being significant; the final result for the predictive mathematical calculation is shown in the Odds Ratio.
Results
The sample consisted of 60 patients who met the eligibility criteria. There was no exclusion in the calculations due to loss data. The average age of the sample was 41.65 years. The average age of the patients with unsatisfactory evolution was 46 years and 39.6 for the other group.
The results of the univariate analysis are shown in tables 1 and 2. Advanced age, female sex, being diabetic, hypertensive, having two comorbidities (diabetes, HBP), nutritional status, overweight, and the involvement of 2-6 quadrants in the first chest X-ray and abnormal leukogram were the most frequent findings in patients with unsatisfactory evolution due to the severity of the infection.
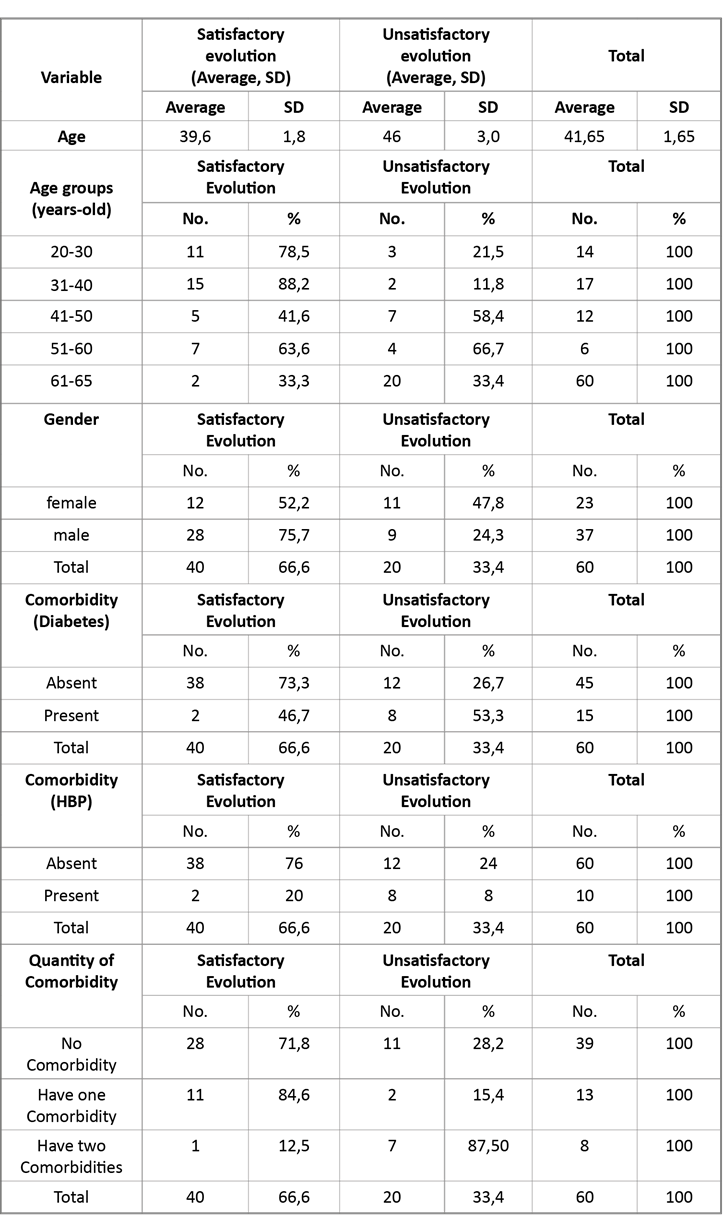
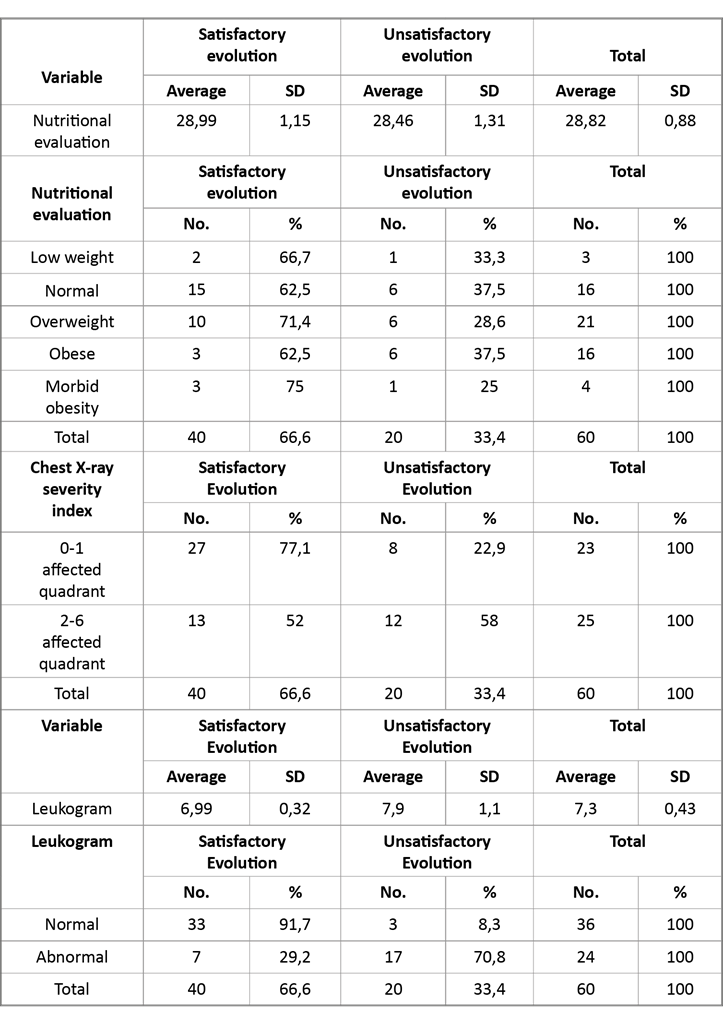
In the bivariate analysis, the progressive increase in age, the age group 61-65 years, suffering HBP, diabetes, having 2 comorbidities, the abnormal leukogram, and the chest X-ray severity index (CSE) resulted with statistical significance. (Table 3)

In the multivariate analysis, two models with statistical significance were obtained, each with the following interpretation. In model 1, only the leukogram with an abnormal value compared to normal is evaluated and the probability of complications is 26,714 times. In model 2, after a goodness adjustment, the abnormal leukogram variable compared to normal and the CSE of 2-6 / 6 compared to 0/6, increase the chances of complication by 68,634 and 12,201 times respectively when they are associated in the same patient; the other resulting models lacked significant p values. (Table 4)

Discussion
The present work showed that being older, belonging to the group of 61-65 years, being female, suffering from hypertension, diabetes, suffering from more than two comorbidities of those evaluated, having 2 or more affected lung quadrants in the evaluation of the initial chest X-ray, and having abnormal leukograms, is related to the unsatisfactory evolution due to the severity of the infection in young and middle-aged patients infected by COVID-19. In addition, two models that predict unsatisfactory evolution were made using the independent variables severity index of the initial chest X-ray and leukogram value with a sensitivity of 83,3 % and a specificity of 85 %, which could be used as a tool to evaluate the prognosis in these patients. Based on the findings, the null hypothesis is discarded, confirming the certainty of the alternative hypothesis.
Case-control studies are subject to selection biases due to loss of information and confusion, which were minimized with the correct methodological design, random and selective selection of cases and controls, blind evaluations by radiologists who analyzed the images, and, finally, the use of multivariate analysis which yielded several predictive models and those that with the most elements of truthfulness were adjusted to the objective were selected; therefore, we validated the results.
In the research, low-cost diagnostic means were used for the evaluation. They are highly available in primary and secondary healthcare centers and provide a tool with the possibility of being disseminated for its use.
Even though young and middle-aged patients were selected in the analysis, the bivariate study demonstrated that the progressive increase in age favored unsatisfactory evolution due to the severity of the infection that led to respiratory failure requiring invasive ventilation or death. The authors agree with the results of Huang et al,1 Williamson et al, 3 Wang et al,10 Toussie et al,15 Cellina et al,16 Bernbeim et al,18 Shi et al,20 Li Y et al,21 Li K et al.22
The female gender had a worse evolution in the bivariate analysis with no changes after controlling for probable confounding variables such as obesity and comorbidities. This result contrasts that reported by the other authors.1,3,10,15,16,18,20,21,22,23,24 It is attributed to the fact that, on that date, the hospital was preferably designated for women.
The comorbidities found were bronchial asthma, type 2 diabetes mellitus, and arterial hypertension. There were only 3 patients affected with asthma with good evolution, therefore we excluded it from the analysis; however, a relationship was observed in the bivariate analysis, with statistical significance between suffering from diabetes mellitus and AHT with an unfavorable evolution. Similar results were obtained by the authors in their works;1,3,10,17,19,20,21,22,23,24 both comorbidities were without sufficient statistical independence in the multivariate analysis.
The nutritional status was not relevant in the present studies, some authors associate obesity with unsatisfactory evolution in patients with COVID-19;3,4,15 the aspects that differentiate both studies are age and ethnicity, which are variables that could influence these results. The other studies reviewed did not include this variable in their investigations.
Concerning imaging findings, other authors used tomography to study patients with COVID-19, concluding that there is a relationship between the number of affected segments and unsatisfactory evolution.18,20,21,22 Tomography as an imaging variant provides better detail of the lung parenchyma with the limitation of being a more expensive study that uses excess ionizing radiation, so it is not useful for evolution. Instead, the present study used the first chest X-ray, a modality available in most healthcare centers with a lower cost, which uses much less ionizing radiation and is very useful to evaluate the great changes that occur in the parenchyma in complicated patients. The final analysis determined that the number of affected quadrants was related to the unsatisfactory evolution due to the severity of the infection which led to the need for invasive ventilation and showed independence in the multivariate study, for which it was included in a predictive model of the evolution of these patients. Toussie et al,15 Celine et al,16 obtained similar results.
Reviewed studies validated the use of C-reactive protein, lactate dehydrogenase, D-dimer, and leukogram as predictors of poor outcome.1,3,10,15,16,18,20,21,22,23,24 In the present work, the value of the leukogram was used in its calculations. Its selection was based on the cost and the proven predictive efficacy validated by studies related to its wide availability in the centers that receive infected patients and the limited availability of others. It is concluded that the worst evolution was related to the abnormal leukogram in the bivariate analysis; similar results were obtained by other authors.1,3,10,15,16,18,20,21,22,23,24 The accompanying leukopenia of these viral infections and/or leukocytosis has been demonstrated when the process progresses or there is superinfection. The variable showed independence in the unsatisfactory evolution due to the severity of the infection when its values were abnormal.
Conclusions
Older age, female sex, suffering from arterial hypertension and/or diabetes mellitus, were the factors related to the unsatisfactory evolution in the presented work; however, care must be taken when using them to determine prognosis in patients between 20-65 years infected with COVID-19 since they themselves did not show a significant influence on the unsatisfactory evolution for the severity of the infection, although their combination with other studied factors can guide in this regard. Two predictive models were formulated using the independent variables resulting from the multivariate analysis with the severity index in the first chest X-ray and the leukogram that demonstrate their validity as the alternative hypothesis and the null hypothesis is discarded. The results of the present investigation are considered valid since the biases were duly controlled with the selection of a robust methodological model.

