










 Serviços customizados
Serviços customizados
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Introduction
The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) was first reported in December 2019 as a very aggressive type of pneumonia. It was named like this by the International Committee on Taxonomy of Viruses (ICTV)1 and counts with a single-stranded, a positive-sense RNA genome (29 903 pair of bases in length)2 that causes the coronavirus disease 2019 (COVID-19)3 which was declared an international health emergency as it is highly contagious and spreads rapidly throughout the world.4,5
On 22 September 2020, the number of infected people confirmed exceeded 30 million, with more than 1 million deaths.5 The most frequent symptoms observed in patients were fever above 38 0C, dry cough, fatigue, dyspnea, and myalgia and to a lesser extent, headache, abdominal pain, nausea, vomiting, and diarrhea.6
The COVID-19 diagnosis is a high priority for public health in order to minimize the spread of pandemic effects and to get transmission control; in this regard, the most sensitive method for the diagnosis of patients with COVID-19 is the chest computed tomography (CT),7,8,9 however, for mass diagnostics, it is not suitable for the investigation of suspected cases.
Another way to diagnose patients infected with SARS-CoV-2 is the real-time reverse transcription-polymerase chain reaction (RT-PCR), a highly sensitive method that detects SARS-CoV-2 RNA and is highly recommended by the World Health Organization (WHO) and the Center for Disease Control and Prevention (CDC) to diagnose COVID-19 cases since this technique amplifies the unique viral RNA sequences present in suspicious swabs samples.5,10,11
Swabs are devices used for the collection of nasopharyngeal and oropharyngeal samples in the context of SARS-CoV-2 detection using RT-PCR, consisting of a long, thin body of flexible polystyrene and a rolled synthetic fiber head that allows the adhesion of viral particles during scraping of the anatomical area.10
Different companies produce hyssops and the main difference between them is the material of the head, which influences the quality of the final product given that the type of hyssop employed is of great importance because it is one of the factors that contributes to the reliability of COVID-19 diagnosis.10
Nasopharyngeal or oropharyngeal swabs are the most commonly used specimens to diagnose suspicious cases, but the virus can also be detected in throat swabs, nasal swabs, sputum, saliva, blood, feces, urine, and bronchoalveolar lavage fluid specimens, although respiratory tract samples tend to test positive for the virus more often.12,13,14
The decrease of RNA detection Sentitivity by RT-PCR can be due to several factors, including sample collection,15 a fact of growing importance if taking into account that the occurrence of false-negative RT-PCR results implies the hospital discharge decision for SARS-CoV-2 positive patients, resulting in possible transmission events.16
This objective of this paper was to evaluate the reliability of CNUERO hyssops for sample collection for SARS-CoV-2 diagnosis versus IMPROSWAB hyssops.
Material and Methods
An exploratory study was made during May-June 2020 in 136 positive patients for COVID-19 from Havana province who were admitted to the General Hospital "Dr. Luis Diaz Soto".17 Each patient included in the study signed an informed consent in accordance with good practices.
During the period in which the study was framed, the incidence of COVID-19 in Cuba was low, therefore, the decision was made to include in the study samples of patients already admitted in the Hospital with a positive SARS-CoV-2 diagnosis. Samples were taken on the 5th day of hospital admission of positive patients to have a statistically comparable number of positive and negative cases to carry out the study. All patients were treated following the same protocol.18
Ethical approval
The Institutional Ethics and Research Board of General Hospital “Dr. Luis Díaz Soto” approved this study that followed the principles of the Declaration of Helsinki.19 The National Expert Group on the management of COVID-19 patients approved this study as well. Furthermore, an informed consent was given by all the patients included in the study.
Hyssops details
IMPROSWAB hyssops were the first hyssops used in Cuba for sample taking for COVID-19 diagnosis. These hyssops were certificated internationally and were taken as a reference to evaluate the Sentitivity of a hyssop of national production.
Two different types of hyssops were used: one of national manufacturing (CNEURO Center) and the other one was imported from Germany (IMPROVE®, IMPROSWAB: Microbial Transport swab for oropharyngeal and nasopharyngeal use).
IMPROSWAB Hyssops
The IMPROSWAB Hyssops (Germany) are ABS, with an external diameter of 2,5 mm, and a length of 150(10 mm with a cut point of 80 mm, a Flocked length of 25(5 mm and flocked diameter of 2,0(5 mm and a fiber of polyamide (Nylon) that covers this section. These hyssops are sterilized using radiation.20
CNEURO Center Hyssops
The CNEURO Center Hyssops are Edistir SR 550 Polystyrene, with an external diameter of 2,5 mm, an internal diameter of 1,7 mm, and a length of 149,5 mm with a precut at one end of 93 mm (this part is used to collect samples). The fiber that covers this section is polyester threads. Once assembled the parts, the hyssops are sent to the ENSUME Packaging Plant where they are packed and sterilized using ethylene oxide.
Sample collection process
The sample collection process employing hyssops was carried out following international guidelines.21
A nasopharyngeal sample was taken from each patient with each type of hyssop. Each type of hyssop was placed in an individual container filled with IMPROVIRAL NAT MEDIUM according to which, the following set of samples was obtained per patient:
Sample 1: Nasopharyngeal swab using CNUERO hyssop
Sample 2: Nasopharyngeal swab using IMPROSWAB hyssop.
In addition, double swab samples were taken with IMPROSWAB swabs and were considered the gold standard (true positive cases) of this study.
Double swab method
Sampling was done with IMPROSWAB hyssops with which a nasopharyngeal and an oropharyngeal swab were performed, each sample was taken with a single hyssop, thus each sample per patient consisted of two hyssops (double swabs), one for nasopharyngeal swab and another for oropharyngeal swab, which are kept in the same container to increase the usefulness and reliability of the samples. This container was transported at 4 degrees and sent to the biosafety laboratory level 2 of the Center for Genetic Engineering and Biotechnology (CIGB), Havana, for the detection of SARS-CoV-2 genetic material by RT-PCR assay.
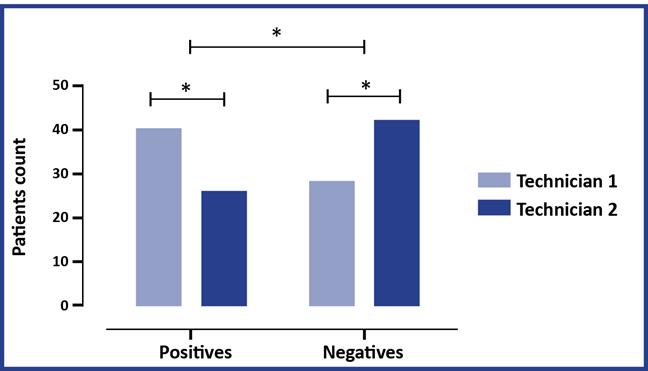
The samples were taken by two technicians who collected samples from 68 patients at random, keeping their data anonymously according to good practices.
SARS-CoV-2 RNA detection
The samples were collected at the hospital following standard procedures and transported to a Biosecurity Laboratory Level 2 for the SARS-CoV-2 viral nucleic acid detection by Reverse Transcription - Polymerase Chain Reaction (RT-PCR), the swabs were placed into a collection tube with a virus preservation solution, and total RNA was extracted with QIAamp® Viral RNA Mini kit using QIAcube automated system (Qiagen, USA).
A 70 bp long fragment from the Equine Arteritis Virus (EAV) genome (LightMix® Modular EAV RNA Extraction Control, TIB MOLBIOL Syntheselabor GmbH, Berlin, Germany) was added before purification as an internal extraction control, amplified with specific primers, and detected with an LC670 labeled hydrolysis probe in the qPCR. A 20 μL qPCR reaction was set up containing 5 μL of RNA and 15 μL with the components of LightCycler Multiplex RNA Virus Master (Roche, USA) and LightMix® Modular Sarbecovirus E-gene or Wuhan CoV RdRP-gene primer and probes systems (TIB MOLBIOL Syntheselabor GmbH, Berlin, Germany).
A real-time one-step RT-qPCR analysis of viral RNA was performed in a LightCycler® 480 II system, with thermal cycling at 50 0C for 10 min for reverse transcription, followed by 95 °C preincubation for 30 seconds and then 45 cycles of 95 °C for 5 s, 60 °C for 30 seconds. Multiplex detection was carried out according to the manufacturer's instructions. Negative and positive controls (≈ Ct 30) were included. The criteria for the success of qPCR detection were the EAV internal control amplification (Ct 27-33) and the amplification of E or RdRP genes at Ct ≤40.
Statistical procedures
All positive samples identified by the gold standard method (double swabs) were considered truly positive, the percentage of positive samples detected for each hyssops type was calculated, as well as the coincidences between them; these data were shown in a table in which the detections were compared using Fisher’s exact test and A p value < 0.05 was considered statistically significant. The SARS-CoV-2 RT-PCR results of each swab brand were analyzed individually and then compared with each other using a ROC curve analysis in the MedCalc statistical software version 13.3 and Graph Pad 8.0.
Results
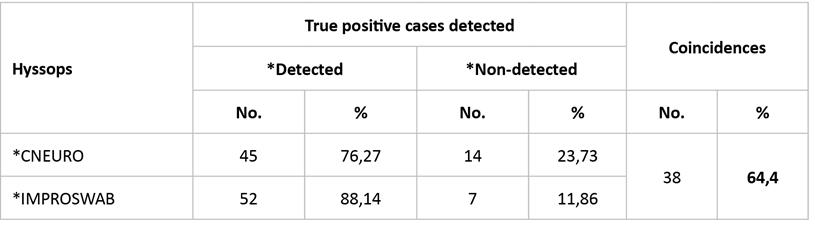
The sample size of the patients studied was 136 and none of the patients showed complications related to the swab sampling process, nevertheless, the true positive diagnosis group obtained with gold standard had a sample size of 59 (43,4 %) and the negative diagnosis group had a sample size of 77, which represents a negativization rate of 56,6 % according to gold standard.
Forty-five positive cases were detected by CNEURO hyssops, while 52 of 59 true positive cases were detected using IMPROSWAB hyssops. Thirty-eight cases were detected simultaneously by using both types of hyssops, for a 64,4 % of coincidence. Non-significant differences were identified between the positive cases detected for each hyssop type. (Table 1).
Regarding sensitivity, it is important to highlight that the samples taken with IMPROSWAB hyssops showed a higher percentage of detected cases over the CNEURO hyssops. (Table 1).
The samples taken with each hyssop type were useful and reliable for diagnosis when compared using individual ROC curve analysis and the gold standard test. The area under curve was statistically different from an area value of 0,5 in each hyssop type (Table 2), which guarantees the reliability of the swab.
Table 2 ROC curves analysis for two hyssop types

A: Area under curve (the area under curve must be significantly different from 0.5 to ensure reliability and usefulness of samples); CI: confidence intervals.
The pairwise comparison of ROC curves between both hyssops (CNEURO vs. IMPROSWAB) showed that there were non-significant differences between the detection sensitivity of each hyssop type (difference between areas: 0,059; standard error: 0,037; confidence intervals: 95 %: -0,014 to 0,133; level of statistical significance in the comparison between the two areas under curve: p = 0,112).
Differences between the detection results with the two hyssop types were shown and evaluated, showing that this behavior was indistinct for both hyssops between them and in relation to the gold standard.
The rate of positive detection between each technician showed a significant difference, as well as in the case of negative results (Figure), in addition, a significant difference was obtained in the positive/negative relationship of each technician, which indicates a variability not linked to the quality of the hyssops but to the sampling process and the skills of the technicians.
Discussion
The RT-PCR technique is the most sensitive and specific molecular method for the detection of SARS-CoV-2 RNA and diagnosis of suspicious cases; its high specificity lies in the molecular basis of this method, which consists in the amplification of a fragment of the viral genome and in another very important characteristic, that is the sufficiency of a small sample, taking into account that a small quantity is amplified repeatedly.2,18
Despite the high level of sensitivity and specificity of this method, it is not infallible since numerous factors can affect the result, namely the moment of the natural cycle of the disease where the samples are taken, the sample collection process, the transport of samples, etc.15 Therefore, the loss of sensitivity in RT-PCR can be the result of several factors including inherent insensitivity to the detection method, variation in the types of detection method used, mutation on target virus genes, low initial viral load, types of specimen, and improper clinical sampling.5,10,15
Samples of nasopharyngeal secretions for the detection of SARS-CoV-2 genetic material by RT-PCR are obtained by nasopharyngeal scraping using sterile swabs certified for use in microbiology.5,10
Nasopharyngeal swabs should follow technical recommendations in terms of design, manufacture and materials. The swab body is recommended to be made of flexible plastic and the region that interacts with the fabrics of synthetic material as polyester.10
The swabbing methodology, despite the invasiveness, is the most effective way to obtain the samples since the detection of genetic material of the virus in saliva or sputum is less sensitive than swabbing10,21 and other procedures such as endotracheal or bronchial sampling are highly invasive and require more care as well as trained personnel and equipment, which represents an inconvenience in times of pandemic.10,11,12
Since the detection of the first cases of COVID-19 in Cuba, the diagnosis was conducted following the WHO recommendations for sample collection using nasopharyngeal and oropharyngeal swabs and RNA detection by RT-PCR.5
The Center for Disease Control and Prevention (CDC) recommends taking samples for molecular diagnosis through nasopharyngeal or oropharyngeal swabs. The reason for this recommendation is that nasopharyngeal swabs are more suitable than the oropharyngeal swabs for the sample taking process, owing to the presence of a higher concentration of the virus in the nasopharyngeal zone and to a lesser extent active replication from the quantitative point of view.10
Multiple studies have been conducted to identify the ideal sample to diagnose COVID-19 and to optimize the process of sample collection, hence, comparisons regarding the sensitivity of nasopharyngeal and oropharyngeal swabs have been carried out, as well as several ways of swab collection processes,18,19,20,21,22,23,24 however, even guaranteeing a swab from one of the best localization where the virus can be found in the body (oropharynx or nasopharyngeal swabs), false negatives cases might arise.19,20 This way, the double swab method increases test sensitivity, and the likelihood of obtaining a false-negative result in a patient with the virus is reduced.22
The combined oropharyngeal and nasopharyngeal swabs were taken at the same time and preserved together in the same container with the same medium, therefore, this is recommended in order to increase the amount of viral material (optimal collection)21,23 and the Cuban protocol against COVID-19 has adopted this methodology due to its efficacy.
Because of these elements, the double swabbing with IMPROSWAB swabs was considered as the gold standard for the diagnosis of COVD-19 in the present study. Against the result of these determinations, the nasopharyngeal exudate samples taken with each type of swab were compared in a comparative study between oropharyngeal and nasopharyngeal swabs, and the nasopharyngeal swabs are superior in terms of sensitivity.21,24,25
The results of this study showed a superiority in the detection of the double swabs in relation to the nasopharyngeal swabs, even despite the latter being the most widely recommended for diagnosis.5,10,19,20,21
A negative qPCR result does not necessarily mean the absence of the virus or a problem with the analytic method; a negative result can be due to the technique, the swabbing area, the type of sample, the swabs quality, the transportation media, and even the transportation itself, thus, the training of health personal becomes essential, as well as a specialized structure.
Every swab sample must be taken by a trained health professional,10,11,18,22 however, there may be still variability associated with the personnel taking the sample. For this study, the same team composed of two graduated microbiologists and experts in sample taking (in accordance with international guidelines),10,22 oversaw the collection of samples.
The time when the samples are collected is very important because the amount of virus present in the nasopharyngeal zone varies over the course of infection, this is why the recommendation is to take samples near the moment of the onset of symptoms to achieve the highest test sensitivity.19
The medium and transport conditions are important too. The samples should be kept refrigerated at 4 0C and sent to the molecular biology lab to be processed in a period not exceeding 24 hours. If it is not possible to send them in less than 24 hours, the samples should be frozen at -80 0C.23
In this study, the same medium was employed for all samples, which were transported under the same refrigeration conditions to limit the inherent variability in this factor.
The factor influencing the result of diagnosis is the manufacture of the hyssop employed;16 according to the CDC guidelines, samples are recommended to be collected employing swabs with a synthetic tip, similar to nylon or Dacron® (polyethylene terephthalate) and an aluminum or plastic handle,16 this is why in the case of the swabs produced in Cuba by CNEURO, polyester fibers were used in an Edistir SR 550 Polystyrene handle. This new variant bears special similitude to the indications of the DCD, only varying the use of polyester threads in the portion used for taking samples.
The Fisher´s exact test and pairwise comparison of ROC curves between CNUERO Hyssops and IMPROSWAB Hyssops showed non-significant differences in the samples taken.
This result is understandable if we consider that the transportation media and the RT-PCR technique were the same to reduce variability and that the only two variables that changed within the study were the hyssops (evaluated product) and the process of sample collection.
The absence of significant differences in the detection of the presence of the virus among hyssops suggests that the variability of the present study was not subjected to the evaluated product but to the process of sample collection.
The main limitation of the present study was the small number of positive cases included; a larger sample would make this study more robust.
Conclusion
It can be concluded that CNEURO hyssops are safe and reliable to be used for nasopharyngeal samples taking of COVID-19 patients. On the other hand, the sample collection process by oropharyngeal swab affects the detection sensitivity of the SARS-CoV-2 virus genetic material through RT-PCR.

