










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkPodium. Revista de Ciencia y Tecnología en la Cultura Física
versión On-line ISSN 1996-2452
Rev Podium vol.17 no.3 Pinar del Río sept.-dic. 2022 Epub 02-Sep-2022
Original article
Exercise program for transfers and gait in spinal cord injured patients
1Centro Internacional de Restauración Neurológica (CIREN), Cuba
2Universidad de las Ciencias de la Cultura Física y el Deporte "Manuel Fajardo". La Habana, Cuba.
Introduction:
Spinal cord injury is considered a trauma that influences all aspects of life, reduces physical abilities and restricts the person in their daily work. One of the main consequences derived from spinal cord injury is the limitation at the level of mobility, which includes walking and transfers.
Objective:
To describe how the CIREN physical exercise program influences gait and transfers in spinal cord injured patients.
Materials and methods:
According to the methodological design, the type of study is experimental, according to the study method, it is observational taking into account the time of occurrence of the events and the recording of the information. For the development of the research, a sample of 15 patients with injury levels between T1 and T6 who met the inclusion criteria was selected.
Results:
Statistically significant changes in gait and transfers were observed in the group; by injury levels, injuries between T1 and T6 did not present changes in stair management and transfers from the floor to the chair; by sex, both men and women did not show statistically significant changes in stair handling and floor-to-chair transfers.
Conclusions:
The exercise program used in the rehabilitation of patients is effective in being able to produce changes in the activities related to walking and transfers. Rehabilitation time should be increased for injuries above T6.
Key words: Spinal cord injury; Gait; Transfers; Physical Therapy and Physical Rehabilitation
INTRODUCTION
Spinal cord injury (SCI) is a devastating health condition, which is associated with permanent disability and reduced life expectancy. Global data show a high incidence between 12.11 and 57.8 per million inhabitants, with a prevalence ranging between 239 and 1009 per million inhabitants (Gaspar, Padula, Freitas, de Oliveira, & Torriani-Pasin, 2019).
The life expectancy of people with SCI has been increasing in recent decades, thanks to technological and scientific advances in aspects of prevention, prehospital care, and management of complications during the course of the disease. This requires providing this population with interdisciplinary care and rehabilitation processes that transcend functional aspects and allow true processes of social inclusion to be achieved.
Various physical therapies have been used in the rehabilitation of people with spinal cord injuries. Physical therapy includes exercises to improve muscle function (strength and endurance) or reduce secondary problems such as pain, fatigue. Among the most prominent interventions are those related to endurance training (Bye et al., 2017; Maher, Anderson, Gant, & Cowan, 2021), electrical stimulation (Abualait & Ibrahim, 2020; Albuquerque et al., 2018), Scivoletto et al. (2014) therapies aimed at improving gait (Harvey, Elsner, Mehrholz, & Thomas, 2017; Mardomingo-Medialdea, Fernández-González, & Molina-Rueda, 2018) balance (Liu et al., 2019; Okawara et al., 2020) and transfers (Ditunno et al., 2013; You, Kim, & Lee, 2017).
The International Classification of Disability and Health Functioning defines transfers as the capacity to transfer the body, which means moving while sitting or lying in bed, from one seat to another, on the same or different level, as well as moving from the wheelchair to the bed. Also called transfer: moving from the wheelchair to another seat, such as a toilet seat or even moving to a vehicle seat. Therefore, their learning and subsequent training is a key point in the rehabilitation process during the acute phase (World Health Organization, 2001).
Among the great motivations of patients with SCI, are achieving walking and achieving transfers to reduce the burden on the family and be able to be more independent and improve the quality of life, which makes constant evaluation of these aspects necessary to achieve a greater satisfaction of patients and relatives. The achievement of these motivations will be conditioned by the intensity of the injury and adequate training of residual capacities.
In the International Center for Neurological Restoration since its inception, there has been an exercise program to recover, restore or replace lost functions in spinal cord injuries that, although it has shown significant results in general, has not been fully detailed. for transfers and walking, so the research aims to describe the influence of the physical exercise program on walking and transfers in spinal cord injured patients.
MATERIALS AND METHODS
The physical exercise program carried out by patients with SCI at the International Center for Neurological Restoration was developed based on three stages of work, with specific objectives by stages. In the first stage (General Preparation), the patients were physically conditioned, the strength and endurance of the supralesional muscles were developed, as well as the residual capacity of the infralesional muscles was stimulated, joint amplitude was improved and contributed to normalize muscle tone.
In the second stage (Special preparation), motor skills training began, highlighting transfers due to the importance that they require for the patient's autonomy.
In the third stage (Functional), the work of gaiting was fundamentally carried out.
Type of study
According to the methodological design, the type of study is experimental, according to the study method it is observational, according to the time of occurrence of the events and the recording of the information, the study is retrospective.
Population and sample: from a population of 40 patients on the date of data collection, a sample of 15 patients was selected who met the following criteria
Study inclusion criteria:
Patients with spinal cord injuries.
Patients who do not have joint limitations that prevent them from standing.
Patients with orthoses.
Patients in rehabilitation treatment for more than two months.
Research exclusion criteria:
Information sources
The information was collected from secondary sources: Clinical file of the patient diagnosed with spinal cord injury who received rehabilitation treatment during the study period.
Information collection method
The information was obtained through a previously designed data collection form, which was completed from the data recorded in the clinical file as a source of information.
Data collection technique
A file containing each of the variables of the present study was made. The total number of patients with a diagnosis of spinal cord injury was obtained from the registry book of the CIREN Department of Statistics, and the clinical records that met the inclusion criteria were requested.
Information collection instrument
Data obtained were processed using the statistical software SPSS, v. 26 for Windows. The information obtained was presented in frequency tables.
Study variables
The following variables were included in the study:
The age variable was expressed in years completed by the patient at the time of admission, it is a continuous variable.
The sex variable corresponded to the gender to which each individual corresponds and was classified as male and female and is nominal.
The variable time of evolution was determined in the years between the spinal cord injury and the time of data collection, it was determined in years and it is continuous.
The level of injury variable expressed the level of the injury according to the affected vertebral level and can be D1, D2, D3, D4, D5, D6, D7, D8, D9, D10, D11, D12 and is ordinal.
The variable classification by level of injury was classified from T1 to T6 in high dorsal and from T7 to T12 in low dorsal, it is ordinal.
Walking Spinal Cord Injury (WSCI) Walking Index for Spinal Cord Injury scoring from 0 to 20, is ordinal.
Spinal Cord Independence Measure, measure of independence for the spinal cord, only the mobility and transfer items were used and scores from 0 to 40, it is ordinal.
Analytical-synthetic, historical-logical and inductive-deductive methods were used. For empirical inquiries, measurement, experiment, interview, observation, and document analysis were used. Among the statistical methods used to process the information susceptible to measurement, the following were used: descriptive measures of position and variation such as the median, the maximum and minimum value and the standard deviation. To statistically corroborate the differences between measurement moments, the Wilcoxon non-parametric test was used, which calculated the degree of significance of the difference between the initial and the final test.
To carry out the experiment, the patients were evaluated with specific scales for patients with spinal cord injury, such as the Walking Index for spinal cord injury. The measure of independence for the spinal cord was also used, from which the items related to mobility and transfers to evaluate them. The evaluation scales were applied to the patients in the morning one week before starting and at the end of the two-month rehabilitation period. All evaluations were carried out by an external evaluator.
The exercise program is designed for two months of rehabilitation with a frequency of two sessions, with an average of five hours per day, designed in three stages of work.
The exercises were dosed in series of ten and the repetitions between 10 and 30 for the trunk muscles and between 10 and 15 for the other muscle groups, the rest between series was established after two minutes and was adjusted depending on the individual characteristics of each patient. The maximum strength was determined from the 10 maximum repetitions and the work weight was established from 60% of the 10 maximum repetitions, which was reassessed weekly and the necessary changes were introduced according to the evolution of the therapy.
There were no differences in training according to the variables of age, sex or level of injury since it was based on an initial physiatry evaluation together with the initial evaluation of the specialist, who is in charge of establishing the starting point of rehabilitation.
The dumbbells and overweights to be used in the program are in all formats from 0.5 kg to 10 kg. For the development of the exercise program, there are 3 gyms distributed in one of functional training that has ergometric bicycles, stair climbers, Robowalk System Expander, Thera E-GO walker, Theratrainer, Balance trainer, Standing table and a mattress area; another gym with a mobilization and massage area and a third gym for strength development with a set for sequential circuit therapy training, wall pulleys, multi-force equipment and horizontal press.
In the area of the gyms, there is a place with a full-time nurse for any inconvenience that may arise in therapy.
The exercise program, being part of a multifactorial and intensive rehabilitation system, headed by a neurologist, who constantly supervises the treatment and, depending on the daily clinical evaluation and together with the specialists, makes the precise decisions to introduce changes that favor rehabilitation to avoid complications.
Exercise program
First stage (General preparation)
Objectives:
Improve joint mobility.
Modulate muscle tone.
Increase muscle strength in the muscle groups above the injury.
Activities:
Passive, assisted and resisted mobilizations of the upper and lower limbs.
Shoulder abduction with dumbbells.
Shoulder adduction with dumbells.
Shoulder horizontal adduction with dumbells.
Elbow flexion with dumbells.
Elbow extension with dumbells.
Trunk flexion.
Trunk extension.
Overweight hip flexion and overweight hip extension.
Hip abduction with overweight.
Hip adduction with overweight.
Overweight knee flexion.
Overweight knee extension.
Mechanotherapy:
Horizontal press.
Multistrength (flexion and extension to strengthen the muscles of the pectorals and shoulders and paravertebral).
High pulley (pulley will be performed in front and behind).
Quadriceps bench (Knee Extension).
Biceps femoris bench (knee flexion).
Multifunctional muscle trainer (For training of the thigh and gluteal muscles, especially anterior thigh, m. Glutaeusmaximus and gastrocnemius).
Back stabilizer/arm trainer (dual function) For training back extensor muscles, shoulder, arm flexors, pectorals and arm extensors.
Leg flexion/extension equipment (double function) Knee flexion and extension.
Flexion / extension of the trunk. Trunk extension / flexion equipment (straight abdominals and upper laterals, dorsal).
Hip flexion/extension unit (dual function) For hip flexion/extension and standing adductors /abductors training.
Explosive pulley system. For universal use and training of the shoulder girdle, upper and lower extremities.
Climber. For training the muscles of the lower limbs.
Balance trainer. For balance and equilibrium training.
Dual function bike. THERA-vital bike and trainer for upper limbs.
Second stage (Special preparation)
Objectives:
Neuromuscular re-education of muscle groups affected by paralysis that have recovery potential
Make the transfers
Develop endurance capacity.
Activities:
Training of all transfers to and from the chair.
Work on the mattress (turns and additions).
Four-point work patterns.
Third stage (Functional preparation)
Objectives:
Achieve independent gait or with the help of gaiting aids (walker, canes, cane) and with or without technical aids.
Activities:
Static and dynamic patterns of gaiting within parallel bars.
Training with the walker or Canadian canes.
Up and down stairs.
Gait with alternate leg raises in place.
Stationary bicycle.
Climber.
Tread mill.
Gait without sticks.
Gait on uneven terrain.
Sample characterization
In the sample studied, there was a predominance of males very similar to that observed by Robles Ortiz (2012) and a greater presence of lower back injuries.
In the descriptive statistics of the sample as a whole, it was obtained that the average age for the sample is approximately 31.67 years and that 95 % of the sample had an age between 21.199 and 34.37 years and that the average age of the sample with a 95 % probability was between 28.96 and 34.37 years. In relation to the average evolution time, it was approximately 3.73 years and that 95 % of the sample had an evolution time that ranged between 1.57 and 5,889 years, that the average evolution time of the sample with 95 % probability was between 3.17 and 4.3 years (Table 1).
Table 1. - Descriptive statistics of the age and evolution time of the sample distributed by sex
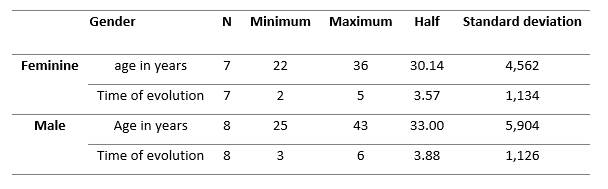
Source: Clinical file.
If a comparative analysis is carried out, it can be seen that in table 1 the mean values, as well as the standard deviation, are higher in males. If the values obtained are compared with the group as a whole, it is observed that the values of the mean age and evolution time in the female decrease and increase in the male, also decreasing the standard deviation for the female case. and increasing for men, slightly decreasing the standard deviation for both men and women.
Table 2. - Descriptive statistics of the age and evolution time of the sample distributed by injury levels (high and low dorsal)
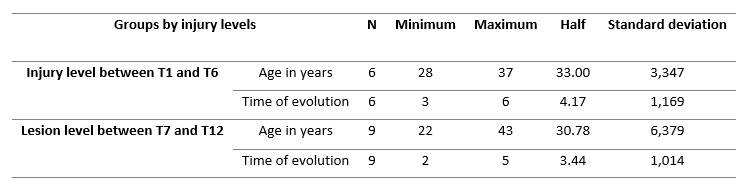
Source: Clinical file
In Table 2, it can be seen that patients with lesions between T1 and T6 had a higher average age than those with lesions between T7 and T12 and a smaller dispersion of ages in relation to the sample as a whole; if the evolution time of the same group is analyzed, we see that the average evolution time increased, which caused a greater dispersion of the data in the evolution time.
In the case of patients with lesions between T7 and T12, it can be said that the average age decreased, however, there was an increase in the dispersion of the data and the average evolution time and dispersion also decreased (Table 2).
RESULTS AND DISCUSSION
Table 3 shows the Wilcoxon signed rank test for the entire sample analyzed, in which it is observed that all the tests reflected statistically significant changes. What was achieved corresponds in part to what was observed by (Kim et al., 2014) when they submitted 60 patients to a two-month rehabilitation program and obtained significant results in WISCI, but not in the mobility items of the SCMI III scale and this could be determined because in their study it was analyzed the scale as a whole and in our analysis only the parameters that evaluated mobility and transfers were addressed (Table 3) .
Table 3. - Wilcoxon signed rank test of the sample
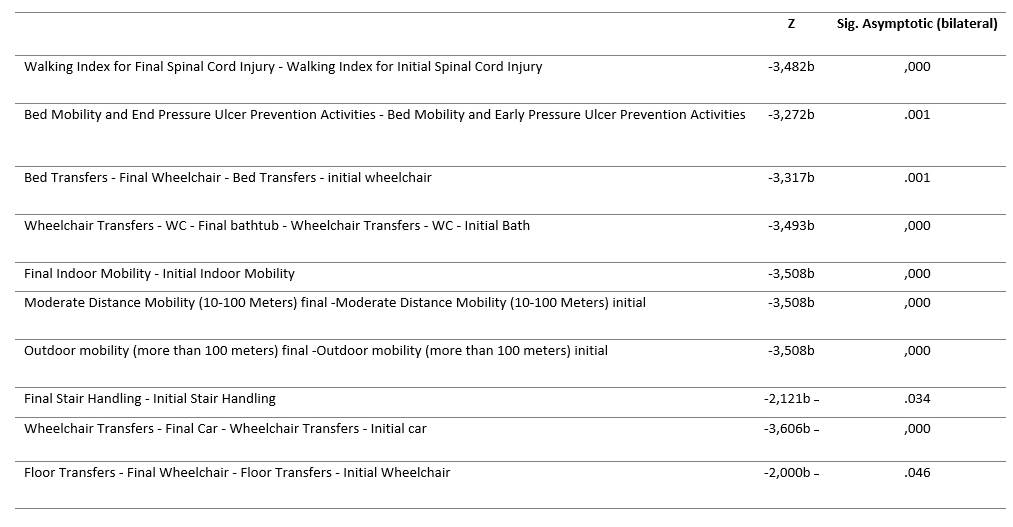
Test statistics. Research Source. a. Wilcoxon signed rank test. b. It is based on negative ranges.
Table 4 reflects the average divided by gender, in which it is observed that there were only no statistically significant changes in the case of handling stairs and transfers from the floor to the chair, which could be attributed to the level of injury of the patients. Similar results were also obtained in the study by (Chang et al., 2020), carried out in Shanghai sunshine Rehabilitation Center with 130 patients to evaluate basic skills and their application in the social aspect in which statistically significant changes were observed in transfer skills, but no changes in walking and stair-climbing activities were observed (Table 4).
Table 4. - Wilcoxon signed rank test of the sample by sex
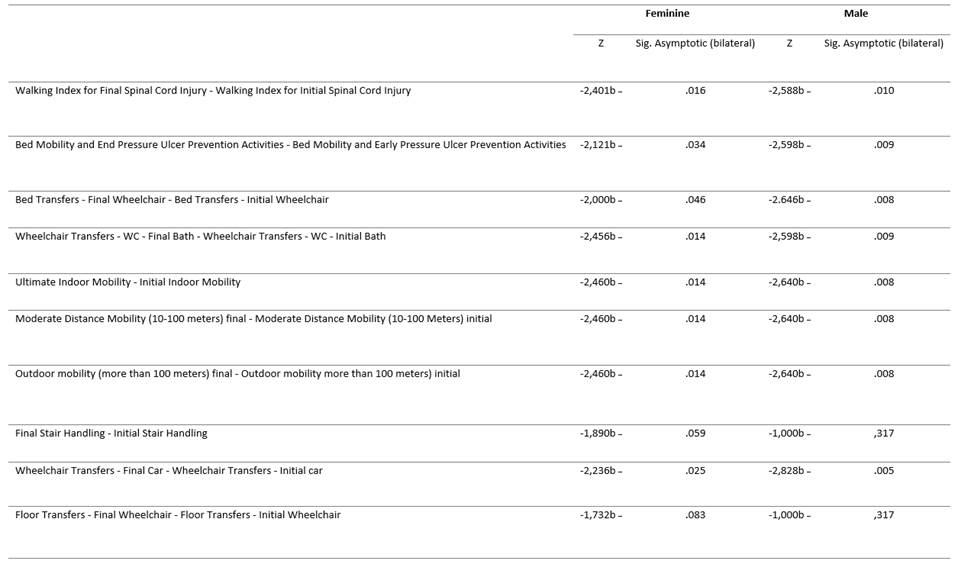
a. Wilcoxon signed rank test. b. It is based on negative ranges. Test statistics a . Research Source.
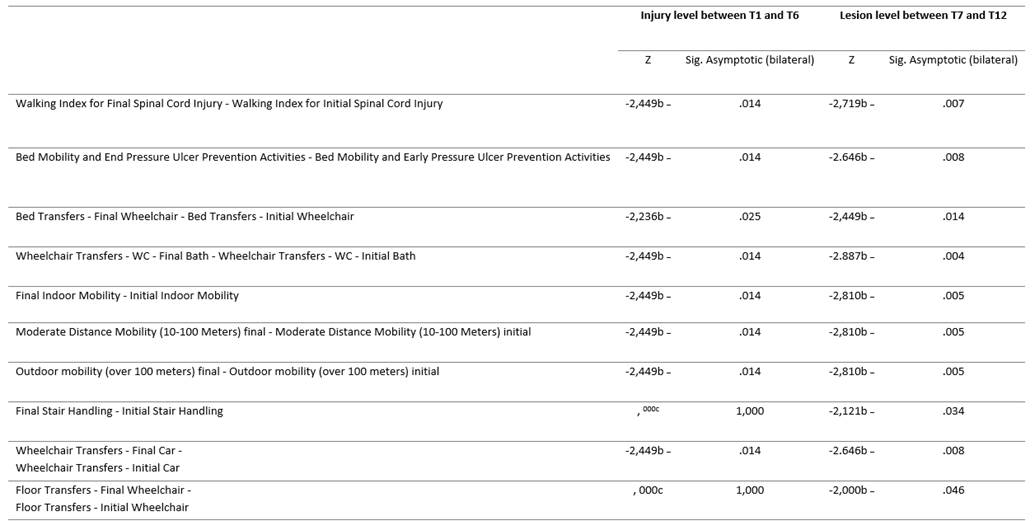
If Table 5 is analyzed, a behavior equal to table 4 can be seen for the case of injuries between T1 and T6 in which there are only no statistically significant changes in handling stairs and transfers from the floor to the chair, and since these patients have less control of the trunk, more time should be spent with these patients to try to achieve the proposed objectives. In the case of lesions between T7 and T12, statistically significant changes were observed in all the parameters analyzed (Table 5).
CONCLUSIONS
The results obtained allowed to determine that the exercise program used in the rehabilitation of patients with spinal cord injuries is effective in being able to produce changes in the activities related to walking and transfers; that the activities of transfers from the floor to the wheelchair and in the management of stairs, in patients with spinal cord injuries between T1 and T6 and by sex with 2 months of work are not enough to obtain statistically significant changes in these parameters.
REFERENCIAS BIBLIOGRÁFICAS
Abualait, T. S., & Ibrahim, A. I. (2020). Spinal direct current stimulation with locomotor training in chronic spinal cord injury. Saudi Medical Journal, 41(1), 88-93. doi:10.15537/smj.2020.1.24818, https://pubmed.ncbi.nlm.nih.gov/31915800/ [ Links ]
Albuquerque, P. L., Campêlo, M., Mendonça, T., Fontes, L. A. M., Brito, R. d. M., & Monte-Silva, K. (2018). Effects of repetitive transcranial magnetic stimulation and trans-spinal direct current stimulation associated with treadmill exercise in spinal cord and cortical excitability of healthy subjects: A triple-blind, randomized and sham-controlled study. PloS one, 13(3), e0195-276. doi:10.1371/journal.pone.0195276, https://pubmed.ncbi.nlm.nih.gov/29596524/ [ Links ]
Bye, E. A., Harvey, L. A., Gambhir, A., Kataria, C., Glinsky, J. V., Bowden, J. L., Gandevia, S. C. (2017). Strength training for partially paralysed muscles in people with recent spinal cord injury: a within-participant randomised controlled trial. Spinal Cord, 55(5), 460-465. doi:10.1038/sc.2016.162, https://pubmed.ncbi.nlm.nih.gov/27922626/ [ Links ]
Chang, F., Zhang, Q., Xie, H., Yang, Y., Shen, C., Shen, X., Lu, J. (2020). The effects of two periods of rehabilitation for people with spinal cord injury from Shanghai, China. Spinal Cord, 58(2), 216-223. doi:10.1038/s41393-019-0349-2, https://www.nature.com/articles/s41393-019-0349-2 [ Links ]
Ditunno, J. F., Ditunno, P. L., Scivoletto, G., Patrick, M., Dijkers, M., Barbeau, H., Schmidt-Read, M. (2013). The Walking Index for Spinal Cord Injury (WISCI/WISCI II): nature, metric properties, use and misuse. Spinal Cord, 51(5), 346-355. doi:10.1038/sc.2013.9, https://pubmed.ncbi.nlm.nih.gov/23459122/ [ Links ]
Gaspar, R., Padula, N., Freitas, T. B., de Oliveira, J. P. J., & Torriani-Pasin, C. (2019). Physical Exercise for Individuals with Spinal Cord Injury: Systematic Review Based on the International Classification of Functioning, Disability, and Health. Journal of Sport Rehabilitation, 28(5), 505-516. doi:10.1123/jsr.2017-0185, https://pubmed.ncbi.nlm.nih.gov/30300056/ [ Links ]
Harvey, L., Elsner, B., Mehrholz, J., & Thomas, S. (2017). Is body-weight-supported treadmill training or robotic-assisted gait training superior to overground gait training and other forms of physiotherapy in people with spinal cord injury? A systematic review. Spinal Cord. doi:10.1038/sc.2017.31, https://pubmed.ncbi.nlm.nih.gov/28398300/ [ Links ]
Kim, H. S., Jeong, H. J., & Kim, M. O. (2014). Changes of Functional Outcomes According to the Degree of Completeness of Spinal Cord Injury. Ann Rehabil Med, 38(3), 335-341. doi:10.5535/arm.2014.38.3.335, https://pubmed.ncbi.nlm.nih.gov/25024956/ [ Links ]
Liu, H., Li, J., Du, L., Yang, M., Yang, D., Gao, F., & Ma, K. (2019). Short-term effects of core stability training on the balance and ambulation function of individuals with chronic spinal cord injury: a pilot randomized controlled trial. Minerva medica, 110(3), 216-223. doi:10.23736/S0026-4806.19.05952-4, https://pubmed.ncbi.nlm.nih.gov/30809995/ [ Links ]
Maher, J. L., Anderson, K. D., Gant, K. L., & Cowan, R. E. (2021). Development and deployment of an at-home strength and conditioning program to support a phase I trial in persons with chronic spinal cord injury. Spinal Cord, 59(1), 44-54. doi:10.1038/s41393-020-0486-7, https://www.nature.com/articles/s41393-020-0486-7 [ Links ]
Mardomingo-Medialdea, H., Fernández-González, P., & Molina-Rueda, F. (2018). Usabilidad y aceptabilidad de los exoesqueletos portables para el entrenamiento de la marcha en sujetos con lesión medular: revisión sistemática. Revista de neurologia, 66(2), 35-44. https://neurologia.com/articulo/2017315 [ Links ]
Okawara, H., Sawada, T., Matsubayashi, K., Sugai, K., Tsuji, O., Nagoshi, N., Nakamura, M. (2020). Gait ability required to achieve therapeutic effect in gait and balance function with the voluntary driven exoskeleton in patients with chronic spinal cord injury: a clinical study. Spinal Cord, 58(5), 520-527. doi:10.1038/s41393-019-0403-0, https://pubmed.ncbi.nlm.nih.gov/31831847 [ Links ]
Organización Mundial de la Salud. (2001). Clasificación Internacional del Funcionamiento, de la Discapacidad y de la Salud: CIF. Madrid: Ministerio de Trabajo y Asuntos Sociales. Secretaría General de Asuntos Sociales. Instituto de Migraciones y Servicios Sociales (IMSERSO). [ Links ]
Robles Ortiz, J., González Roig, J. L., Saborit Oliva, Y., Machado Moreno, L., & Jacas Prado, D. (2012). Epidemiología de la lesión medular traumática. Revista Cubana de Medicina Física y Rehabilitación, 4(2), 85-94. http://www.revrehabilitacion.sld.cu/index.php/reh/article/download/68/48 [ Links ]
Scivoletto, G., Tamburella, F., Laurenza, L., Torre, M., Molinari, M., & Ditunno, J. F. (2014). Walking Index for Spinal Cord Injury version II in acute spinal cord injury: reliability and reproducibility. Spinal Cord, 52(1), 65-69. doi:10.1038/sc.2013.127, https://pubmed.ncbi.nlm.nih.gov/24145685/ [ Links ]
You, J.-S., Kim, Y. L., & Lee, S. M. (2017). Effects of a standard transfer exercise program on transfer quality and activities of daily living for transfer-dependent spinal cord injury patients. Journal of Physical Therapy Science, 29(3), 478-483. doi:10.1589/jpts.29.478, https://pubmed.ncbi.nlm.nih.gov/28356635/ [ Links ]
Received: September 24, 2021; Accepted: June 22, 2022

