Mucoepidermoid carcinoma of the salivary glands in Brazil: clinicopathological outcomes
Carcinoma mucoepidermoide de glándulas salivales en Brasil: relación clinicopatológica
]]>
Lucinei Roberto Oliveira,I Danilo Figueiredo Soave,II João Paulo Oliveira-Costa,II Miguel Angel Sala Di Matteo,II Alfredo Ribeiro-SilvaII
I Vale do Rio Verde University, Brazil.
II University of Sao Paulo, Brazil.
ABSTRACT
]]>
The biological features and clinical behavior of mucoepidermoid carcinomas are widely variable and poorly understood. This study aimed to investigate prognostic factors that may affect survival in patients with a primary diagnosis of head and neck mucoepidermoid carcinomas. The effects of age, gender, anatomic localization, tumor size, clinical stage, histological grade, recurrence, metastasis, compromised surgical margins and treatment on clinicopathological outcomes were investigated. Survival curves were generated using the Kaplan-Meier method and analyses were performed using the log rank test. A total of 16 cases were analyzed over a period of 18 years; males were 68.7 %, with ages ranging from 13 to 83 years. The 75 % of the tumors developed in the major salivary glands, 56.3 % in the parotid gland and they were predominantly classified as stage II 37.5 % and low-grade lesions 37.5 % at diagnosis. Surgical resection was performed in all patients. The follow-up period in this study ranged from 6 to 217 months. The 5 and 10-year overall survival rates were both 85.6 %. Disease-free survival rates were 81.8 % (5 years) and 68.2 % (10 years). There were statistically significant effects of tumor size (p= 0.05), metastasis (p= 0.04) and primary anatomic localization (p= 0.04) on disease-free survival rates. Through a long follow-up period in present study we could highlight the relevance of primary anatomical site, tumor size and metastasis as useful prognostic factors that may affect survival in patients with a primary diagnosis of head and neck mucoepidermoid carcinomas.
Key words: Salivary gland neoplasms, mucoepidermoid carcinoma, disease-free survival.
RESUMEN
Las características biológicas y el comportamiento clínico del carcinoma mucoepidermoide son muy variados y aún poco conocidos. El propósito de este estudio fue investigar los factores pronósticos que puedan afectar la supervivencia de los pacientes con diagnóstico primario de carcinoma mucoepidermoide de cabeza y cuello. Se estudiaron la edad, el sexo, la localización anatómica, el tamaño del tumor, el estadio clínico, el grado histológico, la recidiva, la metástasis, los bordes quirúrgicos comprometidos y el tratamiento, sobre los resultados clínico-patológicos. Las curvas de supervivencia fueron construidas con el método de Kaplan-Meier y el análisis estadístico fue realizado mediante la prueba del log-rank. Fueron analizados 16 casos durante un periodo de 18 años. Se constató un 68,7 % de pacientes del sexo masculino y de edades comprendidas entre los 13 y los 83 años. El 75 % de los tumores se localizó en las glándulas salivales mayores, el 56,3 % en parótida y las clasificaciones predominantes en el momento del diagnóstico fueron lesiones de bajo grado y estadio II con un 37,5 %. La resección quirúrgica fue realizada en todos los pacientes. El periodo de seguimiento en este estudio varió entre 6 y 217 meses. La tasa general de supervivencia, tanto a los 5 como a los 10 años fue de 85,6 %, mientras que las tasas de supervivencia libre de enfermedad fueron de 81,8 % a los 5 años y de 68,2 % a los 10 años. Se demostró la influencia estadísticamente significativa del tamaño del tumor (p= 0,05), la presencia de metástasis (p= 0,04) y de la localización anatómica primaria (p= 0,04) sobre las tasas de supervivencia libre de enfermedad. Los resultados obtenidos demostraron la importancia de la localización anatómica primaria del tumor, de su tamaño y de la presencia de metástasis, en la supervivencia de los pacientes con diagnóstico primario de carcinoma mucoepidermoide.
Palabras clave: neoplasias de las glándulas salivales, carcinoma mucoepidermoide, supervivencia libre de enfermedad.
]]>
INTRODUCTION
Primary malignant salivary gland tumors represent less than 3 % of head and neck cancers and 10-15 % of all glandular tumors. There is a wide variation in these malignant neoplasms over different geographic areas and ethnic groups. Due to the singularity and diverse histology of these tumors, prognostic factors have been difficult to elucidate.1
The establishment and description of mucoepidermoid carcinoma (MEC) as a distinct salivary gland tumor was originally credited to Stewart and others2 (1945). Since then MEC has been described as the most common malignant salivary gland tumor, accounting for close to 10 % of all salivary gland neoplasms.3,4 The clinical behavior of MEC is widely variable, but it seems to correlate with tumor stage and grade.
The mucoepidermoid carcinoma generally shows an extremely aggressive pattern for high-grade tumors, whereas its respectivee low-grade counterpart is often indolent and slow-growing.5,6 However metastases have been described in some cases of low-grade MEC.7 These discrepancies exist likely because there are several histological graduation systems that have been recommended for MECs,7-10 none of which is universally accepted, which makes the retrospective investigations of clinical outcomes difficult.3 In the same way, although complete resection with free surgical margins is the main treatment for MEC, there is still a lack of consensus on the postoperative use of radio and chemotherapy in some cases.3,4 ]]>
The mechanisms of pathogenesis and progression of salivary gland tumors are still poorly understood and studies of prognostic factors that evaluate only one type of salivary gland tumor are scarce for several countries in the world. This study aimed to investigate prognostic factors that may affect survival in patients with a primary diagnosis of head and neck mucoepidermoid carcinomas.
METHODS
A retrospective study was carried out of patients with a primary diagnosis of head and neck MEC treated between 1990 and 2008 at the General Hospital of Ribeirao Preto School of Medicine-USP, Brazil. The medical and surgical records of all cases were reviewed for clinicopathological factors, such as age, gender, primary tumor location, tumor size, clinical stage, histological grade, treatment, compromised surgical margins, tumor recurrence, metastasis, disease-free survival (DFS) and overall survival (OS). The study protocol was performed with prior approval of the local Human Research Ethics Committee (approval number HC/FMRP-USP 10142/2010).
All cases met the criteria proposed by the World Health Organization for the diagnosis of salivary gland MEC.11 Additional inclusion criteria were documented treatment of primary MEC at our institution and a minimum of six months of follow-up information. MECs were staged according to the TNM classification of malignant tumors,12 and minor salivary gland tumors were staged according to their site of origin in a similar fashion to squamous cell carcinomas. Two oral pathologists reviewed all cases to histopathologically classify these tumors according to the protocol published by Brandwein and others10 (2001), which classifies tumors into low (Grade I), intermediate (Grade II) or high (Grade III) grades. Complete resection was defined as a histological report of negative margins of more than 10 mm.13
Patients' features were summarized through descriptive statistics (mean, range for continuous variables and frequency and percentage for categorical variables). The DFS was calculated as the time interval between the date of first treatment and the date of local disease recurrence or last information for censored observations when the patient was known to be disease-free. The OS was defined as the interval between the beginning of the treatment and the date of death or last information for censored observations. Data concerning survival recurrence and metastasis were evaluated. The Kaplan-Meier method was used to plot survival curves with the log rank test for analysis of cumulative survival rates. Statistical significance was defined as a 2-tailed p value of d £ 0.05. ]]>
RESULTS
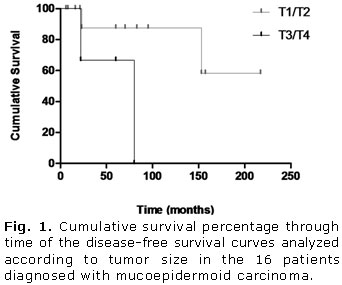
A total of 16 surgically-treated cases of MEC met the inclusion criteria for this survey during the specified period. The clinicopathologic features and results of log rank tests for clinical variables are shown in tables 1 and 2, respectively. The follow-up period in this study ranged from 6 to 217 months (median 65 months), and the 5 and 10-year OS rates were both 85.6 %. The disease-free interval for recurrences and metastases ranged from 22 to 153 months and 22 to 157 months, respectively. Rates of 81.8 % and 68.2 % were found for DFS over a period of 5 and 10 years, respectively.
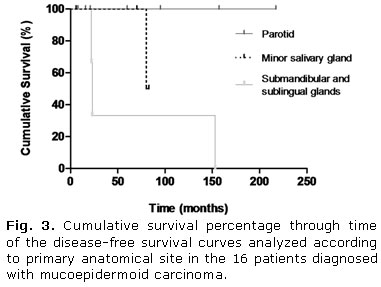
There were no statistically significant differences for any analyzed variable affecting OS curves. However as illustrated in figures 1 and 2, the DFS curves showed significant differences for tumor size (p= 0.05) and metastasis (p= 0.04), respectively. Additionally, a significant influence on prognosis was observed in DFS curves depending on the primary anatomical site. Tumors were stratified into three groups: parotid, minor glands and submandibular/sublingual glands. All tumors diagnosed in the submandibular and sublingual glands had recurrences and metastases (table 1) and consequently, a worse clinical outcome (p= 0.04) (Fig. 3).
]]>
DISCUSSION
The MEC is the most common malignant neoplasm observed in the major and minor salivary glands, comprising about one-third of all patients affected by salivary malignancies.14 Diagnosis can occur over a wide age range but occurs predominantly between the third and sixth decades and affects slightly more women than men (3:2). Almost half of these tumors occur in the major salivary glands, appearing predominantly in the parotid (45 %).10 However, due to its infrequency and histopathological diversity, the epidemiological distribution pattern of primary MECs observed in one country can differ from others and there are still few published studies investigating the behavior of these tumors through long follow-up periods. In the present study, was set out to examine MEC behavior and patient outcomes to provide additional information on potential factors that could significantly affect the prognosis of these tumors.
There were 16 cases of MEC diagnosed over an 18-year period at our institution, which is similar to results reported by Triantafillidou and others14 (2006) who found 16 cases over a 15-year interval. The broad age range observed in our series supports that reported in literature.4,13 Although there are a few studies corroborating our results,13,15 the masculine gender prevalence found differed from commonly reported data that patients diagnosed with MEC are predominantly female.4,16
In agreement with most other studies,4,5,13,15 was found a prevalence of primary tumors diagnosed in the major salivary glands, especially in the parotid gland, followed by intraoral MECs identified in minor salivary glands sited in the hard palate.16,17 In contrast with other investigations,4,13,15 there was an unusual case of a MEC found in the sublingual gland. As in most other studies,4,6,13 Was found a predominance of MECs diagnosed in early clinical stages as T1/T2 and our findings showed a significant influence of tumor size on DFS.4,15 The low rates of recurrence and metastasis found in this study are in agreement with previous reports.4,6 A significant influence of primary anatomical site was observed in DFS curves when there was stratification into three groups because all tumors diagnosed in the submandibular and sublingual glands had recurrences and metastases, which negatively affected the prognosis, this finding confirms previous observations.7,18
Despite several attempts, an established grading system for MEC does not yet exist. The three-level grading system commonly used by pathologists for MEC classification mainly considers the relative proportion of cell types (epidermoid, intermediate and mucinous cells), their respective degrees of atypia and growth patterns (cystic, solid, or infiltrative), together with neural and vascular invasion.7-10 The grading system proposed by Brandwein and others10 (2001) was adopted in this study because it is objective and easy to use and reproduce,3,4 which will help future standardization. Unlike other studies that used this same grading system,4,13 the results demonstrate a balance in distribution among the three tumor grades subtypes. Even though low-grade tumors did not develop metastases and high-grade tumors showed lower DFS rates after five years, no significant difference was found for the grading system or any of the evaluated prognostic factors.
]]>
In contrast to results reported by Nance and others4 (2008) in present study was not observed any association between positive surgical margins and decreased DFS. Although MEC has been described as a radioresistant tumor, postoperative radiotherapy has been associated with decreased recurrence in some reports.13 Conversely, in the present investigation, a trend toward better survival was demonstrated in the group who underwent surgical treatment alone, although this finding was not statistically significant. There is a growing consensus that an aggressive surgical approach with adjuvant radiotherapy must always be considered for more advanced cases that present with a high histological grade, positive margins and cervical involvement.3,4,15,19
The clinical progression of MEC is usually slow and therefore, requires long-term follow-up to establish prognostic factors that could influence clinical outcome. Published works usually lose relevant survival information through time. Although this current investigation was limited by a relatively small sample size, there was a long follow-up period in which we could verify and confirm the influence of some prognostic factors. Further investigation of potential factors that may influence the survival of these patients should be encouraged through longer follow-up periods and larger samples.
Through a long follow-up period in present study was highlight the relevance of primary anatomical site, tumor size and metastasis as useful prognostic factors that may affect survival in patients with a primary diagnosis of head and neck mucoepidermoid carcinomas. Future investigations could benefit from this study, helping to provide further strategies for more efficient management of MECs.
BIBLIOGRAPHIC REFERENCES
]]>
1. Drivas EI, Skoulakis CE, Symvoulakism EK, Bizaki AG, Lachanas VA, Bizakis JG. Pattern of parotid gland tumors on Crete, Greece: a retrospective study of 131 cases. Med Sci Monit. 2007;13(3):136-40.
2. Stewart FW, Foote FW Jr, Becker WF. Mucoepidermoid tumors of the salivary glands. Ann Surg. 1945;122:820-44.
3. Luna MA. Salivary mucoepidermoid carcinoma: revisited. Adv Anat Pathol. 2006;13(6):293-307.
4. Nance MA, Seethala RR, Wang Y, Chiosea SI, Myers EN, Johnson JT, et al. Treatment and survival outcomes based on histologic grading in patients with head and neck mucoepidermoid carcinoma. Cancer. 2008;113(8):2082-9.
5. Guzzo M, Andreola S, Sirizzotti G, Cantu G. Mucoepidermoid carcinoma of the salivary glands: clinicopathologic review of 108 patients treated at the National Cancer Institute of Milan. Ann Surg Oncol. 2002;9(7):688-95.
6. Kokemueller H, Brueggemann N, Swennen G, Eckardt A. Mucoepidermoid carcinoma of the salivary glands clinical review of 42 cases. Oral Oncol. 2005;41(1):3-10.
7. Goode RK, Auclair PL, Ellis GL. Mucoepidermoid carcinoma of the major salivary glands: clinical and histopathologic analysis of 234 cases with evaluation of grading criteria. Cancer. 1998;82(7):1217-24.
8. Batsakis JG, Luna MA. Histopathologic grading of salivary gland neoplasms. Mucoepidermoid carcinomas. Ann Otol Rhinol Laryngol. 1990;99(10 Pt 1):835-8.
9. Auclair PL, Goode RK, Ellis GL. Mucoepidermoid carcinoma of intraoral salivary glands. Evaluation and application of grading criteria in 143 cases. Cancer. 1992;69(8):2021-30.
10. Brandwein MS, Ivanov K, Wallace DI, Hille JJ, Wang B, Fahmy A, et al. Mucoepidermoid carcinoma: a clinicopathologic study of 80 patients with special reference to histological grading. Am J Surg Pathol. 2001;25(7):835-45.
11. Seifert G, Sobin LH. Histological classification of salivary gland tumours. En: World Health Organization. International histological classification of tumours. Berlin: Springer-Verlag; 1991.
12. Wittekind C, Greene FL, Hutter RVP, Klimpfinger M, Sobin LH. TNM Atlas: Illustrated guide to the TNM classification of malignant tumours (UICC). Heidelberg: Springer; 2004.
13. Rapidis AD, Givalos N, Gakiopoulou H, Stavrianos SD, Faratzis G, Lagogiannis GA, et al. Mucoepidermoid carcinoma of the salivary glands. Review of the literature and clinicopathological analysis of 18 patients. Oral Oncol. 2007;43(2):130-6.
14. Triantafillidou K, Dimitrakopoulos J, Iordanidis F, Koufogiannis D. Mucoepidermoid carcinoma of minor salivary glands: a clinical study of 16 cases and review of the literature. Oral Dis. 2006;12(4):364-70.
15. Ozawa H, Tomita T, Sakamoto K, Tagawa T, Fujii R, Kanzaki S, et al. Mucoepidermoid carcinoma of the head and neck: clinical analysis of 43 patients. Jpn J Clin Oncol. 2008;38(6):414-8.
16. Bernardes VF, Ramos-Jorge ML, Vieira Carmo MA, Cardoso SV, Alves Mesquita R, Ferreira Aguiar MC. Intraoral mucoepidermoid carcinoma of salivary glands. Lack of Association Among Clinicopathological Features and Immunoexpression of c-erbB-2 in 29 Cases. Int J Morphol. 2008;26(4):1005-11.
17. Lopes MA, da Cruz Perez DE, de Abreu Alves F, de Almeida OP, Kowalski LP. Clinicopathologic and immunohistochemical study of intraoral mucoepidermoid carcinoma. Otolaryngol Head Neck Surg. 2006;134(4):622-6.
18. Wahlberg P, Anderson H, Biörklund A, Möller T, Perfekt R. Carcinoma of the parotid and submandibular glands a study of survival in 2465 patients. Oral Oncol. 2002;38(7):706-13.
19. García-Roco Pérez O. Tumores de glándulas salivales: su comportamiento en 10 años de trabajo (1993-2002). Rev Cubana Estomatol. 2003;40(3). Disponible en: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S0034-75072003000300001&lng=es&nrm=iso&tlng=es
Recibido: 6 de diciembre de 2011. ]]> Aprobado: 22 de diciembre de 2011.
Dr. Alfredo Ribeiro-Silva. University of Sao Paulo, Brazil. Correo electrónico: arsilva@fmrp.usp.br ]]>

{kind=link}
{kind=link}