Ameloblastic fibrosarcoma arising in the mandible*
Fibrosarcoma ameloblástico en la mandíbula
Marcelo Marcucci, I Karina Cecília Panelli Santos, II Juliane Pirágine Araújo,II Décio Santos Pinto Junior, II Jefferson Xavier OliveiraII
I Department of Stomatology. Heliópolis Hospital, São Paulo. SP, Brazil.
II Department of Stomatology. School of Dentistry. University of São Paulo. SP, Brazil.
ABSTRACT
Ameloblastic fibrosarcoma is a rare odontogenic neoplasm and is considered the malignant counterpart of ameloblastic fibroma. The diagnosis is made by histopathological and immunohistochemical evaluation, since the epithelial component remains benign and the mesenchymal component becomes malignant. Until 2012, only 72 cases were published in English-literature. This article presents a case of intraoral mass at the posterior mandible of a 23 year-old female patient. Panoramic radiography showed a multilocular radiolucent lesion with ill-defined borders and tooth involvement. The mandibular canal presented loss of architecture also. The computed tomography images (bone window) showed hypodense lesion leading to expansion, tapering and irregular destruction of cortical, and tooth involvement. Incisional biopsy was performed for histopathological evaluation. The results revealed a mixed lesion with epithelial and mesenchymal cellular proliferation. At immunohistochemical analysis, the mesenchymal portion was vimentin positive and the epithelial component was positive for cytokeratin AE1-AE3. It also showed p53 intense labeling in all tumorous cells. The final diagnosis was ameloblastic fibrosarcoma. The lesion was surgically excised with clear margins. The radiographic appearance, even imperative for treatment planning, poorly contributed to final diagnosis, which was reached by histopathological and immunohistochemical evaluations. The treatment is still controversial, without a definition regarding chemotherapy and radiotherapy as coadjutant treatment.
Keywords: oral cancer; odontogenic tumor; maxillary neoplasms.
RESUMEN
El fibrosarcoma ameloblástico es una neoplasia odontogénica poco frecuente y es considerada la contraparte maligna del fibroma ameloblástico. El diagnóstico se realiza mediante la evaluación histopatológica e inmunohistoquímica, ya que el componente epitelial sigue siendo benigno y el componente mesenquimal se convierte en maligno. Hasta 2012, solo 72 casos fueron publicados en la literatura inglesa. En este artículo se presenta un caso de masa intraoral en la mandíbula parte posterior, de una paciente de 23 años de edad. La radiografía panorámica mostró una lesión radiolúcida multilocular con bordes mal definidos y con un diente incluso en la lesión. El canal mandibular también presentaba pérdida de la arquitectura. La tomografía computarizada (TC) (ventana de hueso) presentó lesión hipodensa que provocaba una expansión que se estrechaba y destruía irregularmente la cortical, además envolvía la pieza dentaria. Se realizó biopsia incisional para evaluación histopatológica. Los resultados revelaron una lesión mixta con proliferación celular epitelial y mesenquimal. En el análisis inmunohistoquímico, la porción mesenquimal fue positivo para vimentina y el componente epitelial fue positivo para citoqueratina AE1-AE3. También mostró marcación intensa para p53 en todas las células tumorales. El diagnóstico final fue de fibrosarcoma ameloblástico. La lesión fue extirpada quirúrgicamente con márgenes de seguridad. El aspecto radiológico, aunque imprescindible para la planificación del tratamiento, poco contribuyó al diagnóstico final, que fue alcanzado por las evaluaciones histopatológicas e inmunohistoquímicas. El tratamiento sigue siendo controvertido, sin una definición respecto de la quimioterapia y la radioterapia como tratamiento coadyuvante.
Palabras clave: cáncer bucal; tumor odontogénico; neoplasia maxilar.
]]> INTRODUCTION
Ameloblastic Fibrosarcoma (AFS) is a rare odontogenic neoplasm and is considered the malignant counterpart of Ameloblastic Fibroma (AF). Histologically, AFS' mesenchymal portion shows malignant features of sarcoma, which is mixed to a benign ameloblastomatous epithelial component. This tumor either presents de novo or arises from a pre-existing AF.1-7
There is a predilection for males between 26 and 27 years, and posterior mandible area as the most frequent site of occurrence, being locally aggressive.1,6-11 Until 2012, only 72 cases were published in English-literature, which indicate strong tendency to recur but rare metastases of AFS.1
The objective of this report is to present a rare case of Ameloblastic Fibrosarcoma.
CASE REPORT
23-year-old female patient was refered to Heliópolis Hospital (São Paulo-Brazil presenting painful intraoral mass at the posterior left side of the mandible (Fig. 1A). She couldn't explain when she first noticed the lesion and how fast it grew, but she reported it has grown fast.
Patient's medical and dental histories were unremarkable, except for the absence of the first and second molars in the left side of the mandible. At clinical examination the mass was found to be a necrotic tissue added to an erythematous covering mucosa (Fig. 1A). Extraoral examination revealed a painful lymph node at left submandibular area.
Panoramic radiography showed a multilocular radiolucent lesion with ill-defined borders, tooth involvement, and loss of the architecture of the mandibular canal (Fig. 1B). The computed tomography (CT) images (bone window) showed hypodense and expansive lesion involving an irrupted element. Destruction of cortical was detectable (Fig. 1C, 1D). The CT images (soft tissue window) highlighted hypodense areas within an infiltrative lesion. Moreover, contrast-enhanced images presented low contrast penetration, and, in some areas, it overflows the lesion (Fig. 1E, 1F).
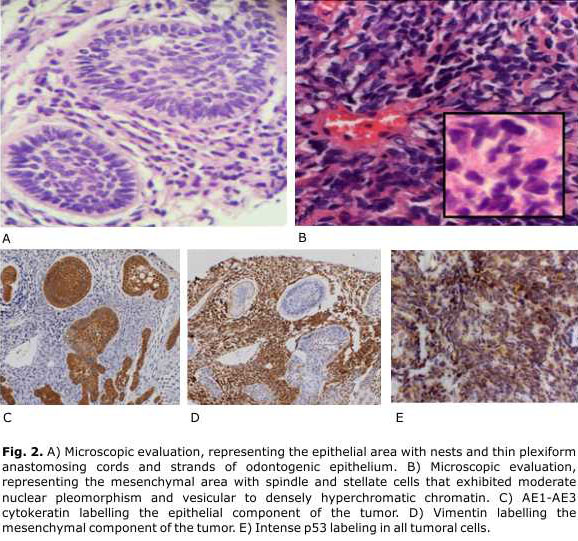
]]>By immunohistoquemical analisys, vimentin and cytokeratin AE1-AE3 were positive in mesenchymal and epithelial components, respectively. Tumoral cells showed intense labeling by p53 (Fig. 2C, 2D, 2E) The final diagnosis was ameloblastic fibrosarcoma.
The treatment consisted in surgical excision followed by area reconstruction. The lesion was accessed through submandibular approach under general anesthesia, and hemimandibulectomy and selective neck dissection (level I) were preformed. A titanium plate was placed for mandibular reconstruction. One month after surgery, the patient returned for routine evaluation. Eight months after surgery, patient presented a good recover without complications or recurrence signals (Fig. 3).
DISCUSSION
]]> Head and neck sarcoma are rare tumors, corresponding to 4 %-10 % of all sarcoma. In maxillofacial area, these tumors are even rarer, representing less than 5 % of all odontogenic tumors, and AFS is the less frequent from all types of sarcoma 9,12-14. Only a third of currently published cases of AFS have originated from a recurrent AF, and this may be the cause of doubtful etiology.8,10,11Clinically, the tumor presents painful swelling and fast growth as.8-11 The case hereby presented seems to be even rarer, since the patient is a woman. However, except for paresthesia, all clinical symptoms were observed.
A substantial number of conditions affecting the jaws may present tumor radiographic appearance. The differential diagnosis includes other odontogenic sarcomas, specifically those entities that present similar histological features, such as ameloblastic fibrodentinosarcoma and fibro-odontosarcoma.13 Because of the rapid growth, and intraoral and images aspects the lesion was thought to be a malignant odontogenic tumor. These entities are rare as primary head and neck lesions arising within the jaws, less than 2-3% of all oral and maxillofacial specimens sent for diagnosis to oral pathology services and 0.002-0.003 % is the estimate rate comparing to hole body tumors.15,16 This rarity makes the specific diagnosis really challenging.15
Radiographically, AFS appear as a radiolucent lesion with ill-defined borders.2,3,5,13,14 Cortical may be eroded.2,3,9 Images from CT exam usually present an invasive mass with cortical expansion and perforation.2,3,11 CT is the method of choice for AFS evaluation, since it allows the observation of lesion's real expansion and adjacent structures involvement without image superimposition or distortions.11 The panoramic radiography from the patient revealed the same features described in the literature. Besides that, CT images clearly showed cortical expansion and destruction, tooth involvement and loss of architecture of mandibular canal. Moreover, the low penetration of contrast during CT exam emphasizes the solid aspect of the lesion.
The microscopic features can be divided into two parts: the benign epithelial part, similar to ameloblastic lesion, and malignant mesenchymal part, with sarcomatous aspects.5,6,8-11,14 The epithelium presents columnar cells, with hyperchromatic nucleus. At mesenchymal tissue the cells are fusiform, with marked pleomorphism, hyperchromatism and abnormal mitotic figures.5,8-11,13 The importance and relevance of imunohistochemical analysis was also addressed, especially in cases of recurrence, with mitotic activity increased at mesenchyme and decreased epithelial evidences 17. Despite the fact that there was no previous lesion, we have decided to investigate the lesion by imunohistochemical approach. The evaluation included vimentin and citokeratins AE1-AE3, and the results revealed the mixed outline of the lesion. The p53 evaluation also proved the alterations are well noticed at sarcomatous lesion.
The treatment of choice is surgical excision with clear margins, because AFS is a very invasive and recurrent lesion.1,3,4,6-11,13 Some authors also include a combination of chemotherapy, radiotherapy.4,7,14 In the current case, the surgical excision was performed, without any recommendations of chemotherapy or radiotherapy as coadjutant treatment. After eight months from surgery, the patient didn't show any evidence of recurrence.
In conclusion, a rare case of an AFS is presented. The radiographic appearance, even imperative for treatment planning, poorly contributed to final diagnosis, which was reached by histopathological and immunohistochemical evaluations. The treatment is still controversial, without a definition regarding chemotherapy and radiotherapy as coadjutant treatment.
Conflictos de intereses
BIBLIOGRAPHIC REFERENCES
1. Noordhoek R, Pizer ME, Laskin DM. Ameloblastic fibrosarcoma of the mandible: treatment, long-term follow-up, and subsequent reconstruction of a case. J Oral Maxillofac Surg. 2012 Dec;70(12):2930-5.
2. Khalili M, Shakib PA. Ameloblastic fibrosarcoma of the upper jaw: Report of a rare case with long-term follow-up. Dent Res J (Isfahan). 2013 Jan;10(1):112-5.
3. Wang BY. Head and neck pathology: SS13-1 Ameloblastic fibrosarcoma of mandible. Pathology. 2014 Oct;46 Suppl 2:S18.
4. Hu YY, Deng MH, Yuan LL, Niu YM. Ameloblastic fibrosarcoma of the mandible: A case report and mini review. Exp Ther Med. 2014 Nov;8(5):1463-6.
5. Loya-Solis A, González-Colunga KJ, Pérez-Rodríguez CM, Ramírez-Ochoa NS, Ceceñas-Falcón L, Barboza-Quintana O. Ameloblastic fibrosarcoma of the mandible: a case report and brief review of the literature. Case Rep Pathol. 2015;2015:245026. doi: 10.1155/2015/245026. Epub 2015 Mar 10.
6. Al Shetawi H, Alpert EH, Buchbinder D, Urken ML. Ameloblastic Fibrosarcoma of the Mandible: A Case Report and a Review of the Literature. J Oral Maxillofac Surg. 2015 Aug;73(8):1661.e1-7.
7. Pourdanesh F, Mohamadi M, Moshref M, Soltaninia O. Ameloblastic Fibrosarcoma of the Mandible With Distant Metastases. J Oral Maxillofac Surg. 2015 Jul 11.
8. Barnes L, Eveson JW, Reichart P, Sidransky D (Eds.): World Health Organization Classification of Tumours. Pathology and Genetics of Head and Neck Tumours. Lyon: IARC Press; 2005.
9. Kousar A, Hosein MM, Ahmed Z, Minhas K. Rapid sarcomatous transformation of an ameloblastic fibroma of the mandible: case report and literature review. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009 Sep;108(3):e80-5.
10. Kobayashi K, Murakami R, Fujii T, Hirano A. Malignant transformation of ameloblastic fibroma to ameloblastic fibrosarcoma: case report and review of the literature. J Craniomaxillofac Surg. 2005 Oct;33(5):352-5.
11. Zabolinejad N, Hiradfar M, Anvari K, Razavi AS. Ameloblastic fibrosarcoma of the maxillary sinus in an infant: a case report with long-term follow-up. J Pediatr Surg. 2008 Feb;43(2):e5-8.
12. Yamaguchi S, Nagasawa H, Suzuki T, Fujii E, Iwaki H, Takagi M, et al. Sarcomas of the oral and maxillofacial region: a review of 32 cases in 25 years. Clin Oral Investig. 2004 Jun;8(2):52-5.
13. Chaisuparat R, Sawangarun W, Scheper MA. A clinicopathological study of malignant odontogenic tumours. Histopathology. 2012 Jul;61(1):107-12.
14. Philipsen HP, Reichart PA. Classification of odontogenic tumours. A historical review. J Oral Pathol Med. 2006 Oct;35(9):525-9.
15. Gupta N, Barwad A, Kumar R, Rijuneeta, Vaiphei K. Ameloblastic fibrosarcoma: A cytologist's perspective. Diagn Cytopathol. 2011 Aug;39(8):598-602.
16. Gilani SM, Raza A, Al-Khafaji BM. Ameloblastic fibrosarcoma: a rare malignant odontogenic tumor. Eur Ann Otorhinolaryngol Head Neck Dis. 2014 Feb;131(1):53-6.
17. Akinyamoju AO, Olusanya AA, Adeyemi BF, Kolude B. Ameloblastic fibrosarcoma: Report of a case. J Oral Maxillofac Pathol. 2013 Sep;17(3):424-6.
Recibido: 3 de diciembre de 2012. ]]>
Aprobado: 4 de febrero de 2016.
Marcelo Marcucci. Department of Stomatology, Heliópolis Hospital, São Paulo, SP, Brazil.
Correo electrónico: marcucci21@gmail.com
__________________________
* This case was presented at 59th Annual Session of the American Academy of Oral and Maxillofacial Radiology (Pittsburgh, PA/USA - 2008) as an Oral Presentation.
]]>