Results of the Electrolysis Percutaneous Intratissue in the shoulder pain: infraspinatus, A Randomized Controlled Trial
Resultados de la electrólisis percutánea intratisular en el dolor en el hombro: infraespinoso, un ensayo controlado aleatorio
Résultats de l'Électrolyse Percutanée Intra-tissulaire contre la douleur de l'épaule : Muscle sous-épineux. Une étude contrôlée et randomisée
María Dolores R-Moreno
]]> Universidad de Alcalá. Madrid, España.
ABSTRACT
Background: The Electrolysis Percutaneous Intratissue (EPI®) is a novel technique that provokes a local inflammatory process, allowing the phagocytises and affected tissue to repair.
Objectives: The work is aimed to: a) verify the effectiveness of the EPI® when there is shoulder pain, b) locate where the EPI® should be applied, c) and find the possible interaction between the trigger points and the tendon pain.
Design: Randomized controlled trial.
Setting: Institute of Physiotherapy and Sports.
Method: A double randomized experimental longitudinal study was conducted on four groups of 10 people aged 34-47 years with pain in the shoulder. In the first study there were three intervention groups and a control group. In the second study, the group with the best results in the first study served as a control group.
Measurements: The variables measured were the perceived pain and the restriction for abduction, internal and external rotation.
Results: Although the three intervention groups improved respect to the control group when the EPI® was applied, the results show that the EPI® is more effective when it is applied in all detected trigger points and to tendon pain.
Conclusions: The EPI® is more effective if applied in the infraspinatus muscle and the tendon than applied only to one of the two structures, when both structures have pain.
Limitations: The study could have tested the involvement of different structures and its related biomechanical implications. It could have also considered more variables.
Keywords: EPI®; muscle-tendon complex infraspinatus; trigger points; tendon pain; mobility restrictions; randomized trial.
RESUMEN
Introducción: la electrólisis percutánea intratisular (EPI®) es una novedosa técnica que provoca un proceso inflamatorio local, que permite la fagocitosis y la reparación del tejido afectado. ]]>
Objetivos: verificar la efectividad de la EPI® cuando hay dolor del hombro, b) localizar dónde debería ser aplicada la EPI® y C) y determinar la interacción entre los posibles puntos de activación y el dolor del tendón.
Diseño: estudio controlado aleatorio.
Ubicación: Instituto de Fisioterapia y el Deporte.
Método: se realizó un estudio longitudinal experimental aleatorizado doble en cuatro grupos de 10 personas con edades entre 34-47 años que sufrían dolor en el hombro. En el primer estudio hubo tres grupos de intervención y un grupo de control. En el segundo estudio, el grupo que tuvo mejores resultados en el primer estudio sirvió como grupo de control.
Mediciones: las variables que se midieron fueron dolor percibido y la restricción de la abducción, rotación interna y rotación externa.
Resultados: aunque los tres grupos de intervención mejoraron respecto al grupo de control cuando se aplicó la EPI®, los resultados muestran que la EPI® es más eficaz cuando se aplica en todos los puntos de activación detectados y donde hay dolor en los tendones.
Conclusiones: la EPI® es más eficaz si se aplica en el músculo infraespinoso y el tendón que si se aplica solo a una de las dos estructuras, cuando ambas presentan dolor.
Limitaciones: el estudio podría haber probado la participación de diferentes estructuras y sus implicaciones biomecánicas relacionadas. Podría también haber tenido en cuenta más variables.
Palabras clave: EPI®; músculo-tendón infraespinoso complejo; puntos de activación; dolor en los tendones; restricciones a la movilidad; estudio aleatorio.
RÉSUMÉ
Mots clés: EPI®; complexe musculo-tendineux sous-épineux; points de stimulation; douleur tendineuse; limitations de la mobilit; étude randomisée.
INTRODUCTION
Shoulder pain is one of the most frequent pains in humans. Generally, the patient points to a wide area that can go from the cervical spine, and the scapular-thoracic region reaching the upper limb. In general, muscle and tendon structures contribute to the maintenance of bone segments.1 Then, the initial anamnesis is very important to clarify what the patient means when s/he speaks of shoulder pain and, fundamentally, what is the range of possible pathologies that would define the diagnostic, therapeutic and preventive procedures.
In general, studying and analyzing all possible causes of the onset of shoulder pain and the different procedures for therapeutic-palliative approach is quasi-infinite.
The first author of the article has been the Physiotherapist for the National handball team for several years. His experience and his concern in shoulder injuries has shown him that ailments in the infraspinatus muscle was one of the main causes that prevented the athletes from practicing sports.
Also, outside the sport arena, we have observed that the muscle-tendon complex infraspinatus is frequently the origin of pain, and there is little published work despite its incidence and prevalence in clinical practice. These facts have aroused the curiosity of testing the muscle-tendon complex infraspinatus, and we have tried to discover the level of involvement and possible interaction in the muscle-tendon pain when the patient lies on his/her shoulder and/or back.
The infraspinatus muscle-tendon complex is determined by the position of the scapula, which in turn influences the direction of the lever arm in execution of its functions. The tendon is a fundamental element of the musculoskeletal system, and once the injury is produced, the tendon enters an initial healing phase-repair process that if prolonged enters a progressive degradation process called tendinosis.2-4 The muscle tissue is another key part of the locomotor system and a metabolic reservoir formed by contractile cells that specializes in carrying out the work of the interactions of contractile proteins actin and myosin from chemical energy.
It is common to listen to the muscle-contract designation, but in recent years we are also getting used to the trigger point term. By examining various related segments, we note that there are a number of points called trigger points in the infraspinatus muscle that sometimes produce referred pain in the examination and sometimes not.
The trigger point is defined as an irritable area located in a tense band of muscle fibers. When we press it, the pain perception increases, which may or may not produce referred pain.
]]> The work done by Shah5 shows that in the trigger points there is a high level of concentration of substances such as P substance, interleucina1-β, serotonin, bradykinin, glutamate, among others, and that the dry needle puncture of these trigger points decreases the concentration level of these substances.In general, professionals in the field assign the cause of pain to the tendon due to a tendinopathy, or to the muscle due to the trigger points, and we proceed to address it in isolation or together when we know that the muscle and tendon structures contribute in a relationship between origin and insertion.1
Recently, it has been proved that the Electrolysis Percutaneous Intratissue (EPI®) can stimulate the tendon biology, initiate an inflammatory response, and promote wound healing in tendons of rats.6 Some studies show the efficacy in chronic lateral elbow epicondylitis.7 It is emerging as the great therapeutic alternative to the lack of evidence with other therapies. In particular the lack of evidence reflected in conservative therapies.8-10
The EPI® consists of applying a galvanic current through puncture needles that acts as a negative electrode (cathode), causing an electrochemical reaction in the tissue. This reaction provokes a local inflammatory process, allowing the phagocytises and affected tissue to be repaired.
It mobilizes and attracts cells involved in regeneration-healing, opening calcium channels11,12 DNA synthesis, and collagen produced.13,14
Then, in this study we want to test the EPI® in patients with shoulder pain and analyse where it should be applied.
Objective
The purpose of the study was threefold. First, it aimed to verify the effectiveness of the EPI® when there is shoulder pain. Second, it located where the EPI® should be applied. Third, it identified the possible interaction between the trigger points and the tendon pain, and its bidirectionality.
METHOD
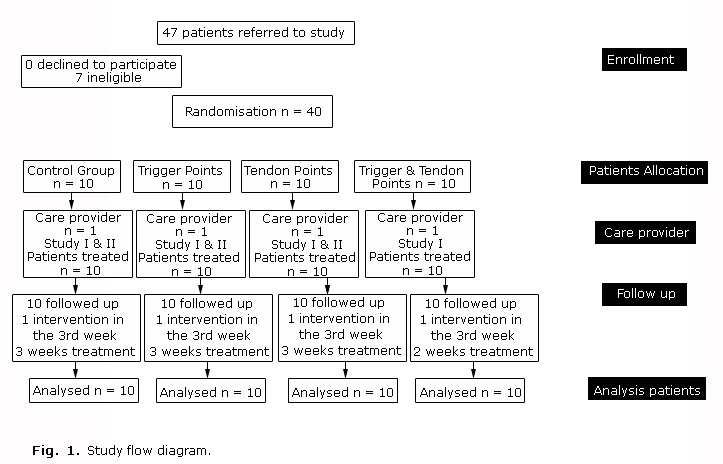
]]> Design OverviewWe have performed a longitudinal parallel study consisting of 40 subjects randomly divided into 4 groups of 10, each group with a balanced distribution by gender (5 males and 5 females). The sample size was selected following the criteria: 1) a homogeneous balance between the groups 2) a size that guarantied the statistical significance and that could be collected by the institute within a reasonable time.
The trial was divided into two parts: in the first part there was three intervention groups and a control group. In the second one, the group with the best results in the first study served as a control group.
Participants
The age limit was set in a decade that would have allowed the development of the disease between 34 to 47 years. Some authors7 consider that the inflammatory process is what sets the acute phase of the injury, and it lasts approximately 3 weeks.
The exclusion criterion was being operated and/or suffering systemic diseases. We have discarded 7 patients under this criterion (2 with systemic diseases and 5 for being operated).
The inclusion criterion in the study was the presence of trigger points in the infraspinatus muscle and pain in the tendon of at least a 3 month duration. The mobility of the shoulder in abduction, internal rotation and external rotation, was limited by the appearance of pain while performing the movement. The level of pain could not be less than 65 in the Visual Analogue Scale (VAS).
Settings
We have used the following to carry out the experimental work:
]]> - The facilities of the Institute of Physiotherapy and Sports.- Electric current by the apparatus with marked EPI® EEC Cesmar manufactured by serial number 114, power supply voltage 12v. DC; maximum current output of 330 mA and maximum output voltage of 30V. Electrical protection type BF Class IIa.
- The application of EPI® was 6 mA intensity, 4 seconds duration and 3 impacts.
- Physiotherapy invasive needles CE 0197. The dimensions of the needles depended on the estimation of anthropometry of the subject and the estimation of the depth we wanted to access.
- The Visual Analogue Scale (VAS) brand Uniphy (www.uniphy.nl) for measuring the pain variable perceived. The range of values is from 0 to 100, being 100 the highest pain value.
- Goniometer provided by Gidotti-Farma (Menarini Group) for measuring the range of movement and establishing the joint limitation for onset of pain during abduction, internal rotation and external rotation of the shoulder. The values were measured in degrees.
Randomization and Interventions
In order to assess the effects of the treatment, we have compared the results with patients who did not receive it.15 In previous published studies7 a control group was not included.
The features of each group are:
]]> 1. Control group that continued with their daily activities (CT).2. Intervention group where the EPI® was applied only in all detected trigger points (TP).
3. Intervention group where the EPI® was applied only in the tendon of the infraspinatus (T).
4. Intervention group where the EPI® was applied in all detected trigger points and the tendon (TTP).
An Ethic Committee at the Institute of Physiotherapy and Sports was formed on 15th January 2013 to approve the trial. It verified the results on 2nd July 2013. The randomized controlled trial started at the end of March 2013 and concluded during the second week of June 2013. Each patient that arrived to the facilities and met the inclusion criteria was randomly allocated to a group depending on sex. That is, the first man and the first woman to the first group, and the second man and the second woman to the next group, and so on until the first's participants of the 4 groups were completed. Then, we repeated the same process for the second participants and so on, until we collected ten persons in each group. All the patients knew that they were enrolled in a trial, but they never knew what group they belonged to nor the existence of any other group. All the patients signed a consent document.
Outcomes and Follow-up
In total we performed four measurements: an initial one before initiating the treatment and three subsequent ones performed after application of a weekly treatment.[a] We measured the level of pain, the limit of abduction, internal rotation and external rotation. We divided the study into two parts according to the evolution of the variables. The first study corresponds to the first three measurements, and the second one to the fourth measurement. None of the enrolled participants gave up the trial, and there were no changes in the trial after it commenced. Finally there was no harm or unintended effects on any of the intervention groups. Figure 1 summarizes the participant flow diagram.
RESULTS
Tables 1 and 2 show the values for the different variables measured for the 4 groups under study. The rows represent the mean and the standard deviation of each group, while the columns represent first the age, and then the initial pain value (VASi) followed by the pain value measured after one week after the treatment, and the same sequence for the abduction limits, internal and external rotation limits. Figure 2 represents graphically the VAS values for the 4 measurements for each group.
]]>
Table 3 represents the statistic significance for all the variables under study (p-values and confidence intervals).
From table 3, we can see that there was changes between VASi with VAS1 in the three intervention groups (p<0.001) and between VAS i & VAS2 and VAS1 & VAS2(p<0.001) in T and TTP but in TP(p<0.05). There were no significant differences in the level of perceived pain in relation to age (p>0.05). There were also no significance differences in the level of perceived pain in relation to sex (p>0.05).
In the comparison between the VASi with VAS1 and VAS2, the CT group did not decrease the perception of pain at any time (p> 0.05), and there were significance differences with the rest of the groups (p<0.001). The best results were for the TTP group followed by the T group and in last place, the TP group. The comparison between the VAS1 and VAS2 is similar to the results between VASi and VAS2.
In the descriptive analysis of the restriction of mobility for abduction (Abd.Limit), we observed changes (p<0.001). In the Abduction limits comparison between Abd.Limiti & Abd.Limit1, Abd.Limiti & Abd.Limit2, and Abd.Limit1 with Abd.Limit 2, there was interaction of our interventions and variations were obtained for the 3 groups (p<0.001). There were no significant differences in the level of restriction of mobility for abduction in relation to age (p>0.05) or in relation to sex (p>0.05).
In the comparison between the Abd.Limiti & Abd.Limit1, Abd.Limiti & Abd.Limit2, and Abd.Limit 1 & Abd.Limit2 the CT group did not improve its level of mobility restriction at any time (p>0.05). But all intervention groups improved (p<0.001) with significant differences respect to the CT group, except for the comparison between the TP and T groups (p>0.05). The TTP group obtained the best result compared to the other groups (p<0.001).
Related to the Internal Rotation limits comparison between Int.Roti & Int.Rot1, Int.Roti & Int.Rot2, and Int.Rot1 & Int.Rot2 there was interaction of our interventions and variations that were obtained for the 3 groups (p<0.001). There were no significant differences in the level of restriction of internal rotation limits in relation to age (p>0.05), nor in relation to sex (p>0.05).
In the comparison between the Int.Roti & Int.Rot1, Int.Roti & Int.Rot2 and Int.Rot1 & Int.Rot2the CT group did not improve its level of mobility restriction at any time (p>0.05); however, all intervention groups improved (p<0.001) with significant differences with respect to the CT group, but the T and TP groups did not present differences between them (p>0.05).
Finally, we present the results for the External Rotation Limits. In the comparison between Ext.Roti & Ext.Rot1 and Ext.Rot i & Ext.Rot2, and Ext.Rot1& Ext.Rot2 there was interaction of our interventions and variations that were obtained for the 3 groups (p<0.001). There were no statistic differences in the level of restriction of mobility for external rotation in relation to age (p>0.05) and not also in relation to sex (p>0.05).
In the comparison between the Ext.Roti and the Ext.Rot1 the CT group did not improve its level of mobility restriction at any time (p>0.05); however, all intervention groups improved (p<0.001) with significant differences with respect to the CT group, except for the T and TP groups without differences between them (p>0.05). But there were differences of the TTP group in relation to the T and TP groups.
]]> For the second study, we started from the 3 measures already collected and performed a final measurement. As mentioned before, the TTP group served as a control group since it was the group with the best results: the pain perception was almost null and the mobility was recovered (then, any treatment was applied for the TTP group). In the fourth measurement, we observed that there were changes (p<0.001) in all the variables measured. The Post Hoc shows significant differences between all groups (p<0.001) after the EPI® application in all the trigger points and in the tendon.
CONCLUSIONS
According to the results, we can infer that our intervention could introduce variations in the pain perception in the three groups under study and no improvement in the control group. Furthermore, we observed that the degree of improvement was increasing in our successive interventions. Besides, during our interventions, we did not reach significant differences to lower the pain perception between the TP and T groups, despite the large decreased in pain perception between the two groups.
In summary, we found that our interventions decreased the scale pain perception from our first intervention for the TTP and T groups, and in the second intervention for the 3 intervention groups. The TTP group presented the best results, and the positive response of the T group was earlier than the TP group. Then, we can say that:
1. The application of the EPI® in the trigger points and the tendon of the infraspinatus muscle (together or alone) is effective in reducing the pain and the mobility restriction in abduction, internal rotation and external rotation limits when there is pain in the tendon and trigger points below the infraspinatus muscle.
2. The EPI® is more effective if applied in the infraspinatus muscle and the tendon than applied only in one of the two structures, when both structures have pain.
3. In the case of comparing the application of the EPI® in the muscle or the tendon, there were no differences after two applications, but the perception of the pain diminishes in the first application in the tendon, and its application in the muscle required two applications to arise the same effect.
4. The application of two sessions of EPI® together in the tendon and the muscle with an interval of one week was enough for a quasi-full recovery, while the isolated application of EPI® on two sessions in the tendon or muscle did not produce the similar recovery, leaving pain and partial limitations.
]]> 5. The significant improvement in the CT group and the TP and T groups with the third EPI® when applied together in the tendon and the muscle, once again confirmed the efficiency of the treatment in both structures.6. The tendon and muscle can interact in mutual damage.
Limitations of the Study
The study could have been more ambitious by testing the involvement of different structures and its related biomechanical implications, and it could have considered more variables.
Conflict of Interest
None declared.
What this study adds?
The study has shown that when there are trigger points in the muscle and pain in the tendon of the infraspinatus:
]]>1) The EPI® is an effective treatment that helps to lower the pain and mobility limits values.
2) The EPI® is more effective when it is applied together in the trigger points and the tendon, although improvements are appreciated when it is applied in isolation. These findings suggest the existence of interaction on both structures.
What is already known on this topic?
This novel treatment obtains excellent results in a short period of time compared to existing treatments. We believe is going to have a big impact, in the short term, of the clinical practice.
BIBLIOGRAPHIC REFERENCES
1. Stoller DW. MRI, Arthroscopy, and Surgical Anatomy of the Joints. Philadelphia: Lippincott-Raven; 1999. ISBN-13: 978-0781715805.
]]>2. Cook JL, Purdam CR. Is tendon pathology a continuum? A pathology model to explain the clinical presentation of load-induced tendinopathy. Br J Sport Med. 2009;43:409-16.
3. Khan KM, Cook JL, Kannus P, Maffulli N, Bonar SF. Time to abandon the "tendinitis" myth. BMJ. 2002;324:626-7.
4. Fu SC, Rolf C, Cheuk YC, Lui PP, Chan KM. Deciphering the pathogenesis of tendinopathy: a three-stages process. Sports Med Arthros Rehabil Ther Technol. 2010 Dec 13;2:30. doi: 10.1186/1758-2555-2-30.
5. Shah JP, Phillips TM, Danoff JV, Gerber LH. An in vivo microanalytical technique for measuring the local biochemical milieu of human skeletal muscle. J Appl Physiol. 2005;99:1977-84.
6. Valera-Garrido F, Minaya-Muñoz F, Sánchez-Ibáñez JM, García-Palencia P, Valderrama-Canales F, Medina-Mirapeix F, et al. Comparison of the acute inflammatory response and proliferation of dry needling and Electrolysis Percutaneous Intratissue (EPI) in healthy rat Achilles tendons. Br J Sports Med. 2013;47:32. doi: 10.1136/bjsports-2013-092459.56
7. Valera-Garrido F, Minaya-Muñoz F, Sánchez-Ibáñez JM, Medina-Mirapeix F, Polidori F. Short- and long-term outcomes of electrolysis percutaneous intratissue (EPI) in chronic lateral elbow epicondylitis. Br J Sports Med. 2013;47:3. DOI:10.1136/bjsports-2013-092459.38
8. Maffulli N, Longo UG. Conservative management for tendinopathy; is there enough scientific evidence? Rheumatology. 2008;47:390-1.
9. Fredberg U, Bolvig L. Jumper´s knee. Review of the literature. Scand J Med Sci Sports. 1999;9:66-73.
10. Peers KH1, Lysens RJ. Pattelar tendinopathy in athletes; current diagnostic and therapeutic recommendations. Sports Med. 2005;35:71-87.
11. Huttenlocher A, Horwitz AR. Wound healing with healing with electrical potential. N Engl J Med. 2007;356:303-4.
12. Jaffe LF, Vanable JW Jr. Electric fields and wound healing. Clin Dermatol. 1984;2:34-44.
]]>13. Cheng N, Van Hoof H, Bockx E, Hoogmartens MJ, Mulier JC, De Dijcker FJ, et al. The effects of electric currents on ATP generation, protein synthesis and membrane transport of rat skin. Clin Orthop Relat Res. 1982;(171):264-72.
14. Bourguignon GJ, Jy W, Bourguignon LYW. Electric stimulation of human fibroblasts causes an increase in Ca2+ influx and the exposure of additional insulin in receptors. J Cell Physiol. 1989;379-85.
15. Hancock M, Herbert RD, Maher CG. A guide to interpretation of studies investigating subgroups of responders to physical therapy interventions. Phys Ther. 2009;89(7):698-704. doi: 10.2522/ptj.20080351.
Recibido: 16 de noviembre de 2015.
Aprobado: 18 de enero de 2016.
María Dolores R-Moreno. Departamento de Automática, E-318. Escuela Politécnica Superior. Carretera Madrid-Barcelona, Km. 33,6. Universidad de Alcalá 28805, Alcalá de Henares. Madrid, España.
Phone: +34 91 885 6607 Fax: +34 91 885 6641 E-mail: mdolores@aut.uah.es malola.rmoreno@uah.es URL: http://atc1.aut.uah.es/~mdolores/
a) The CT group did not receive any treatment until the second study, that is, the third scheduled week of the study.
{kind=link}
{kind=link}
{kind=link}
{kind=link}