Primary and secondary impaction of four primary molar teeth in a single patient
Retención primaria y secundaria de los cuatro primeros molares en un paciente
Bruno Ramos ChrcanovicI; Ana Cristina Rodrigues Antunes SouzaII; Ricardo Mascarenhas PaixãoIII; Leandro Napier SouzaIV ]]>
IDoctor in Dental Surgery. Private practice in General Dentistry, Belo Horizonte, Minas Gerais, Brazil.
IIMaster in Sciences. Doctor in Dental Surgery. Adjunct professor of Head and Neck Anatomy and Orthodontics. Centro Universitário Newton Paiva, Belo Horizonte, Minas Gerais, Brazil.
IIIDoctor in Dental Surgery. Private practice in Orthodontics, Belo Horizonte, Minas Gerais, Brazil.
IVMaster in Sciences. Doctor in Dental Surgery. Adjunct professor of Oral and Maxillofacial Surgery. Centro Universitário Newton Paiva, Belo Horizonte, Minas Gerais, Brazil.
ABSTRACT
The lack of eruption of a primary tooth can be considered rare. In primary impaction, the primary tooth not only has never appeared in the oral cavity, but also is always covered by a more or less thick layer of bone. Secondary impaction, which is relatively more common, denotes teeth that at one time erupted into the mouth, but subsequently clinically appear to have receded from this position. The purpose of this paper is to present a case of primary and secondary impaction of four primary molar teeth in a single patient. ]]>
Key words: Tooth ankylosis, impacted tooth, unerupted tooth, primary dentition.
RESUMEN
La falta de erupción de un diente temporal puede ser considerada una situación rara. En la retención primaria, no sólo el diente temporal nunca ha aparecido en la cavidad bucal, sino que también está cubierto por una capa más o menos gruesa del hueso. La retención secundaria, que es relativamente más común, se refiere a los dientes que inició su erupción en la boca, pero clínicamente quedan atrapados en esta posición. El propósito de este trabajo es presentar un caso de retención primaria y secundaria de cuatro molares primarios en un paciente.
Palabras clave: anquilosis del diente, impacción, diente no erupcionado, la dentición primaria.
]]>
INTRODUCTION
Eruption failure may affect one or a number of teeth, in either the primary or the permanent dentition, and can be partial or complete, depending upon the underlying etiology. The majority of unerupted teeth are permanent teeth, and they may fail to erupt either as a result of mechanical obstruction, being it from idiopathic or pathological origin, or because of disruption to the eruptive mechanism itself.1
The lack of eruption of a primary tooth can be considered rare. Despite of, primary teeth are ankylosed much more frequently than permanent ones. The tooth in question is almost always a molar and frequently in the mandible.2-5 Extraction has been widely recommended as treatment, in order to prevent complications.
Primary impaction is rare: in primary impaction, the primary tooth not only has never appeared in the oral cavity, but is also always covered by a more or less thick layer of bone.6 Primary impaction has been defined as the prevention (often by a physical barrier) of the eruption of a tooth at the expected times. This obstacle could be a bud of a tooth, an odontoma, a cyst, a tumor, or a dento-maxillo disharmony or malposition and/or malformation of the bud of the tooth itself.4
The following are criteria for a correct diagnosis of primary impaction of primary teeth:6 (a) Deep retention into the bone; (b) Absence of caries or restorations of the crown; (c) No resorption of the roots; (d) Frequent passing of the corresponding permanent tooth; and (e) Possible retention and malposition of the corresponding adjacent permanent tooth.
Secondary impaction: which is relatively more common, denotes teeth which at one time erupted into the mouth, but subsequently clinically appear to have receded from this position (Albers, 1986), i.e., the cessation of further eruption after a tooth has penetrated the oral mucosa.1
Although the tooth submerges and appears to move apically, there is no evidence whatsoever to demonstrate any actual apical displacement of a submerged tooth. So, this can be discarded as a cause. The submersion must be due to occlusal movement of the neighbouring teeth while the affected tooth moves less or not at all. This may be caused by: (a) failure or reduction of the eruptive force; (b) obstruction of the erupting tooth or (c) fixation of the tooth to the surrounding tissue so that it cannot move.7 In case of severe submersion, clinical disturbance may include incomplete alveolar process development, lack of normal mesial drift, non-response to orthodontic forces, retained primary teeth with or without a successor and impaction of the successor, a depressed tooth with tipping adjacent teeth, supra-eruption of opposing teeth, lateral open bite and higher frequency of crossbites.8-9
The exact factor of primary teeth submersion has not yet determined. Suggested factors are ankylosis, congenitally missing permanent teeth, defects in the periodontal membrane, trauma, injury of the periodontal ligament, precocious eruption of the first permanent molar, defective eruptive force, or a combination of these factors. From all of the cited etiological factors, ankylosis seems to be involved in the majority of cases or at least as a coexisting factor.10
The purpose of this paper is to present a case with primary and secondary impaction of four primary second molars in the same patient. ]]>
CASE REPORT
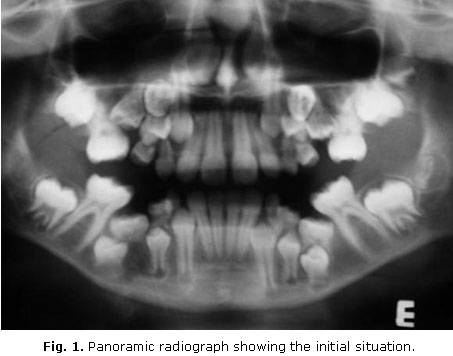
A 10-year-old girl was referred to an Orthodontic Clinic for evaluation. Clinical examination revealed that the two superior second primary molars were missing, and the two inferior second primary molars were submerged and ankylosed. A panoramic radiograph, taken on that occasion, disclosed the presence of the "missing" two superior second primary molars near the maxillary sinus. It also showed impaction of the two superior second pre-molars by the first superior permanent molars. There was no dental agenesis (figure 1). The parents discarded a familiar history. So, the patient was referred to an oral and maxillofacial surgeon to perform a surgical treatment as first phase of the treatment. At the first surgical treatment, the inferior second primary molars were removed.
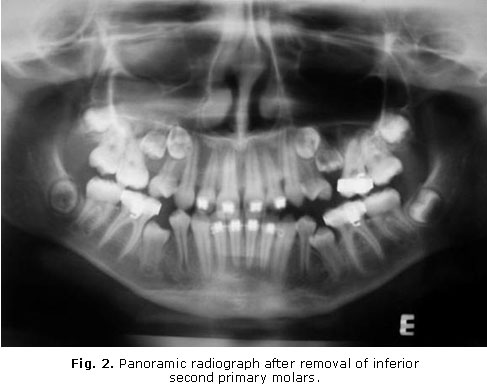
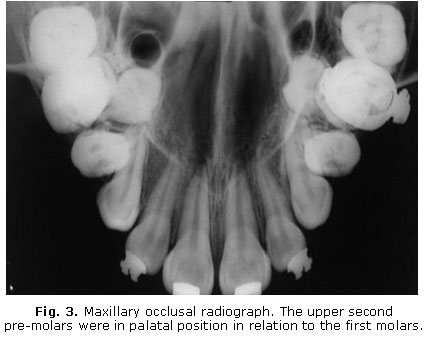
Figure 2 shows the patient at the age of 12. The inferior canines and first pre-molars were already at the occlusal plane and the second pre-molars in their normal path. At this age an occlusal radiograph of maxilla was made (figure 3). The upper second pre-molars were in palatal position in relation to the first molars. So, it was accomplished the extraction of the upper second primary molars and upper second pre-molars as recommended by her orthodontist. After removal of the four ankylosed primary second molars and four second premolars the patient is under current orthodontic treatment.
]]>
DISCUSSION
The malposition of the permanent tooth, sometimes noticed, can by no means be the cause of the primary impaction, if anything is the result of it. The primary tooth in fact is never originally located in a deeper position than the permanent tooth, but beside it, on the palatal or lingual side, slightly closer to the occlusal plane.11 This fact occurred in the present case report. As shown in figure 3, the permanent superior second pre-molars are on the palatal side of the impacted primary second molars. In primary impaction, the permanent tooth passes the corresponding primary tooth, probably prematurely ankylosed, and may lose its correct expected position,11 though this really not happened in the present case (figure 1).
It is not reasonable to suggest that the force of eruption should be affected in such a localized manner when the force is adequate elsewhere in the jaws, nor does a locally less effective force explain why two, three or four quadrants of the same dentition should be affected. It is likely that the obstruction/impaction occurs only after submersion has taken place and results from the tilting of the neighbouring teeth into the gap so created. Ankylosis provides an excellent reason for the teeth being held back and prevented from erupting. No other explanation can do this.6-7 Submersion of deciduous teeth is caused by ankylosis which prevents further eruption, so that the neighboring teeth continue to erupt past them, carrying with them the soft tissue and bone, to submerge the ankylosed tooth.4-7 Spontaneous reactivation of the eruption of ankylosed molars occurs occasionally, as a consequence of resorption of the area of ankylosis.7 It is likely that ankylosis also plays a leading role in primary impaction. The only difference is that occurs very early, always before the emergence of the tooth.5,11
Tooth ankylosis is defined as a fusion of the cementum and/or dentin with alveolar bone, with obliteration of the periodontal membrane, with occurs either before or after tooth eruption.3,12 Several conditions have been proposed as causes of ankylosis: (a) Genetic tendency;13 (b) Traumatic injury to the bone and/or periodontal ligament;12 (c) Development disturbances in the periodontium;14 (d) Deficient local vertical bone growth;15 and (e) Disturbed local metabolism with disorder in the process of normal resorption and hard tissue repair.2 Congenital absence of permanent teeth has also been proposed as the cause of primary tooth ankylosis, but it cannot be accepted as sufficient, because such absence is not always associated with ankylosis of the corresponding primary molars.3
The dental, medical and familial history of our patient did not contribute to explain the reasons of submergence. Therefore, only the development disturbances in the periodontium14 and/or the disturbed local metabolism with disorder in the process of normal resorption and hard tissue repair2 might explain the impactions in the present case.
Radiographically, obliteration of the periodontal ligament space is noted in ankylosis, as also noted here, especially with the inferior primary molars (figure 1). The roots are less radio-opaque and as the ankylosis progresses they are less distinguished from surrounding bone.
Submerged primary molars may cause several problems in dental arch such as space loss, tipping of adjacent teeth, supra-eruption of the antagonists and dislocations of permanent teeth lying under the primary tooth.9 According to Kurol and Thilander,16 these disturbances have no long-term effects on occlusion. On other hand, Becker and Shochat17 have detected a significant deviation of the dental inter-incisor midline toward the affected side. In the present case, there was no deviation of the dental inter-incisor midline, probably due to the bilateral and symmetrical occurrence, but a mild malocclusion occurred.
Diagnostic criteria of impacted primary teeth include the age of the patient, condition and occlusal status of the infraoccluded tooth, root resorption and adjacent alveolar bone levels.18 The treatment plan of a submerged primary tooth depends on degree of abnormality, the present of its successor permanent teeth and time of onset.8-9 Distinguishing between lack of eruption due to some external interference and primary failure of eruption is important clinically, because the latter condition does not respond to the application of orthodontic force.19
Early tooth extraction for the treatment of submerged teeth is recommended. In previous research it was found that no primary molars in infraocclusion with agenesis of the successor exfoliated spontaneously, in contrast to primary molars for which the successor was present, in which its exfoliation occurs by the erupting successor resorbing the area of fusion.8 Considering this affirmation, the teeth was removed in the present case because extensive bony ankylosis might have prevented normal exfoliation, causing future alignment problems,8,16 and also because early extraction provides more time for spontaneous mesial drift, and also a more favorable age for the orthodontic treatment that is usually necessary.20 Active orthodontic force will most likely result in localized ankylosis and failure to extrude an affected tooth into occlusion, a finding that is essentially diagnostic.21 ]]>
In the presented case the impacted upper second premolars and primary molars teeth were removed because of the deeper location inside bone and great lack of arch perimeter. The preferable treatment option for the inferior impacted teeth was extraction only of the primary molars because the submerged deciduous mandibular second molars probably inhibited movement of the teeth germ of the second premolars, which were in the correct position of eruption. Therefore, the mandibular second pre-molar erupted correctly with orthodontic traction. If this therapy were not performed, the patient could have experienced future problems with the definitive orthodontic treatment.Alternatively, a localized bony osteotomy and orthodontic extrusion of the whole segment would seem to be the only option if an occlusal position of the tooth or teeth is to be obtained. If some eruption of the tooth has occurred, a coronal build-up may be the treatment of choice, in this case accepting the vertical position of the affected tooth but achieving occlusion via the restoration. Cases where multiple teeth are involved are more difficult to manage; the only available method of bringing them into occlusion is a segmental osteotomy.21 Careful planning in these cases is essential to ensure that no damage is caused to adjacent teeth. While surgical repositioning may not move teeth into an entirely acceptable position, it will certainly aid prosthetic management.
The management of a tooth eruption failure is difficult, not least because diagnosis of this condition relies principally upon exclusion, where all possible causative factors have been considered and eliminated. The possibility of a number of complications resulting from infra-occlusion/impaction of primary molars (tipping of the neighboring teeth, loss of space, and over-eruption of the antagonist),16 may indicate a need for early intervention by extracting the submerged/impacted tooth and the institution of a comprehensive orthodontic treatment. If this is not undertaken, periodical observation is mandatory. The treatment options should always be discussed with the parents, and the possible complications clearly explained, if the condition is left unattended.19
BIBLIOGRAPHIC REFERENCES
1. Raghoebar GM, Boering G, Vissink A, Stegenga B. Eruption disturbances of permanent olars: a review. J Oral Pathol Med. 1991;20:159-66.
2. Biederman W. The problem of the ankylosed tooth. Dent Clinic North Am. 1968;409-24.
3. Brearley LJ, McKibben DH. Ankylosis of primary molar teeth. I. Prevalence and Characteristics. ASDC J Dent Child 1973;40:54-63.
4. Bordais P, Gineste P, Grant J, Marchand J. Les dents incluses. Encycl Méd Chir. Paris: Ed Stomatologie; 1980. p. 10-2.
5. Albers DD. Ankylosis of teeth in the developing dentition. Quintessence Int. 1986;17:303-8.
6. Bianchi SD, Roccuzzo M. Primary impaction of primary teeth: a review and report of three cases. J Clin Pediatric Dent. 1991;15:165-8.
7. Darling AI, Levers BG. Submerged human deciduous molars and ankylosis. Arch Oral Biol. 1973;18:1021-40.
8. Ekim SL, Hatibovic-Kofman S. A treatment decision-making model for infraoccluded primary molars. Int J Paediatr Dent. 2001;11:340-6.
9. Altay N, Cengiz SB. Space-regaining treatment for a submerged primary molar: a case report. Int J Paediatr Dent. 2002;12:286-9.
10. Antoniades K, Kavadia S, Milioti K, Antoniades V, Markovitsi E. Submerged teeth. J Clin Pediatr Dent. 2002;26:239-42.
11. Jameson GD, Burke PH. Inversion of second deciduous molar and second premolar. Br Dent J. 1987;162:265-6.
12. Henderson HZ. Ankylosis of primary molars: a clinical, radiographic, and histologic study. ASDC J Dent Child. 1979;46:117-22.
13. Via WF. Submerged deciduous molars: familial tendencies. JADA. 1964;69:127-9.
14. Kurol J, Magnusson BC. Infraocclusion of primary molars: an epidemiological study. Scand J Dent Res. 1984;92:564-76.
15. Glucksman DD. Localized vertical growth disturbance. JADA. 1942;29:184-7.
16. Kurol J, Thilander B. Infra-occlusion of primary molars and the effect on occlusal development. A longitudinal study. Eur J Orthod. 1984;6:277-93.
17. Becker A, Shochat S. Submergence of a decisuous tooth: its ramifications on the dentition and treatment of the resulting malocclusion. Am J Orthod. 1982;81:240-4.
18. Sidhu HK, Ali A. Hypodontia, ankylosis and infraocclusion: report of a case restored with a fibre-reinforced ceromeric bridge. Br Dent J. 2001;191:613-6.
19. Ben-Bassat Y, Brin I, Fuks AB. Occlusal disturbances resulting from neglected submerged primary molars. ASDC J Dent Child. 1991;58:129-33.
20. Steiner-Oliveira C, Gavião MB, dos Santos MN. Steiner-Oliveira C, Gavião MB, dos Santos MN. Congenital agenesis of premolars associated with submerged primary molars and a peg-shaped lateral incisor: a case report. Quintessence Int. 2007;38:435-8.
21. Proffit WR, Vig KWL. Primary failure of eruption: a possible cause of posterior open-bite. Am J Orthod. 1981;80:173-80.
Recibido: 15 de junio de 2010. ]]> Aprobado: 20 de septiembre de 2010.
Dr. Leandro Napier Souza. Centro Universitário Newton Paiva, Belo Horizonte, Minas Gerais, Brazil. E-mail: leandronapierdesouza@gmail.com ]]>