Hábitos y estilos de vida asociados al síndrome metabólico
Habits and lifestyles associated with the metabolic syndrome
]]>
My. Ángel Arpa GámezI; My. Odalys González SotolongoII; Tte. Cosette Vega FernándezIII
IDoctor en Ciencias Médicas. Especialista de II Grado en Medicina Interna. Profesor Titular. Instituto Superior de Medicina Militar "Dr. Luis Díaz Soto". La Habana, Cuba.
IIEspecialista de II Grado en Endocrinología. Instructora. Instituto Superior de Medicina Militar "Dr. Luis Díaz Soto". La Habana, Cuba.
IIIEspecialista de I Grado en Medicina General Integral. Instituto Superior de Medicina Militar "Dr. Luis Díaz Soto". La Habana, Cuba.
RESUMEN
OBJETIVO: Determinar la posible relación entre los hábitos y estilos de vida y el síndrome metabólico, y a su vez conocer cómo se comporta cada variable que constituye el síndrome con el estilo de vida. ]]>
MÉTODOS: Se diseñó una investigación observacional analítica en la cual se estudia un grupo de 123 oficiales a quienes se les toma las variables que constituyen el síndrome metabólico según los criterios del Adult Treatment Panel III y el IB para evaluar hábitos y estilos de vida. Se relaciona el estilo de vida con el síndrome metabólico y con cada uno de sus criterios diagnósticos.
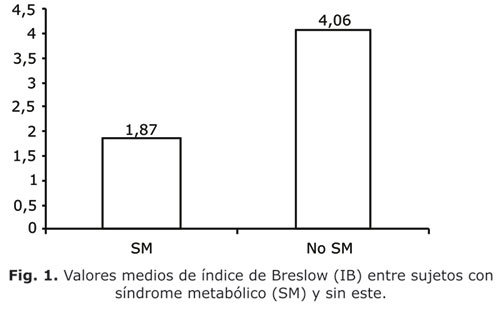
RESULTADOS: El grupo de individuos con síndrome metabólico mostraron un valor medio de IB de 1,87 (desviación estándar [DE]: 0,65), muy inferior a quienes no presentaron el síndrome (4,06; DE: 1,07), con diferencia significativa. Todas las variables que constituyen el síndrome metabólico se deterioraban en la medida que el IB demostraba peores estilos de vida. En la medida que se sumaban en los individuos un mayor número de criterios diagnósticos de síndrome metabólico, la media del puntaje del IB decrecía significativamente, de 4,31 (DE: 1,08) entre quienes no presentaban ningún criterio diagnóstico a 1,00 entre aquellos que reunían los 5 criterios.
CONCLUSIONES: Existe asociación entre los hábitos y estilos de vida y la presencia del síndrome metabólico en general y de cada una de sus variables constituyentes.
Palabras clave: Hábitos y estilos de vida, síndrome metabólico.
ABSTRACT
OBJECTIVE: To determine the possible relation between habits and lifestyles and the metabolic syndrome and at the same time, to know the behavior of each variable that is the syndrome with relation to the lifestyle.
METHODS: An analytical and observational research was designed to study a group of 123 officers whose variables of metabolic syndrome we took according to the criteria of the Adult Treatment Panel II and the Breslow's index to assess the habits and lifestyles. Authors related the lifestyle and the metabolic syndrome and to each of their diagnostic criteria.
RESULTS: The group of subjects presenting metabolic syndrome showed a Breslow's average index of 1.87 (SD): 0.65 very low compared with those without this syndrome (4.06; SD: 1.07) with a significant difference. All variables of metabolic syndrome were deteriorated insofar as that the Breslow's showed the poor lifestyles. In the subjects with a increasing number diagnostic criteria of metabolic criteria the average marks of the Breslow's index decreased significantly from 4.31 (SD: 1.08) among those without diagnostic criterion to 1,00 among those fulfilling the 5 criteria. ]]>
CONCLUSIONS: There is an association between the habits and the lifestyles and the presence of metabolic syndrome in general and of each constituent variable.
Key words: Habits and lifestyles, metabolic syndrome.
INTRODUCCIÓN
El síndrome metabólico (SM) constituye una constelación de alteraciones clínicas y humorales que confluyen en un mismo individuo y relacionadas patogénicamente por diversos mecanismos no totalmente esclarecidos pero donde indudablemente juegan un papel importante ciertos factores genéticos y ambientales.
Dentro de los factores ambientales, los llamados hábitos y estilos de vida tienen una función determinante. ]]>
El estilo de vida es un modo de vida individual. Se relaciona estrechamente con la esfera conductual y motivacional del ser humano.1 Dentro de las múltiples dimensiones que abarca este concepto, dos de ellas se relacionan directamente con el SM: la actividad física y los hábitos de alimentación.La "occidentalización" de los hábitos dietéticos y la "motorización" de la sociedad parecen desempeñar una función importante.2 A medida que la sociedad del llamado Tercer Mundo se "desarrolla y moderniza" cambia su estilo de vida y se asemeja a la del llamado Mundo Occidental: aumenta el sedentarismo, la ingesta de productos ricos en grasa saturada, muy hipercalóricos y elaborados con apenas productos naturales, en un proceso que algunos han nombrado pintorescamente como "coca-colonización"3 y otros "efecto McDonald".
La disminución progresiva de la actividad física que vienen experimentando las sociedades humanas desde hace décadas ha sido claramente asociada al SM, la diabetes mellitus y la morbilidad-mortalidad por enfermedades cardiovasculares.4-8 Esto se explica por el incremento en el transporte motorizado, el advenimiento de la televisión,9,10 la computación y los videojuegos. En particular la población infantil y juvenil parece ser la más afectada;11-13 se reporta una prevalencia cada vez más elevada del SM en estos grupos de edades.
Conocer tales hábitos y estilos de vida en una población determinada contribuiría a detectar factores de riesgo modificables, que a través de los trastornos metabólicos que implican, propiciarían la alta incidencia y prevalencia de las enfermedades cardiovasculares.
El índice de Breslow (IB) constituye una forma sencilla y práctica de valorar algunos de estos hábitos y estilos de vida, ya validada en las publicaciones internacionales, por lo que se decide emplear en el estudio de una población de oficiales con el objetivo de determinar su relación con el SM y por tanto, su utilidad para valorar el riesgo en estas personas y consecuentemente, recomendar modificaciones en los mismos.
MÉTODOS
Se diseñó un estudio observacional analítico, de tipo retrospectivo y corte transversal, para el cual se escogió como población a estudiar los oficiales activos de una unidad militar en el período de marzo 2008 a febrero 2009. A todos los oficiales se les tomaron los datos generales y las variables clínicas y humorales que constituyen el SM, según los criterios del ATP III (anexo 1) y se les aplicó el cuestionario que constituye el IB (anexo 2).
Para algunos análisis se dividieron en 2 grupos: aquellos con SM según los criterios señalados y los que no presentaban el síndrome. Se relacionaron las diferentes variables que constituyen el SM con el IB. Se emplearon métodos estadísticos descriptivos y comparación de medias entre grupos, con significación de alfa < 0,05. ]]>
RESULTADOS
De los 123 sujetos estudiados, 16 cumplían los criterios diagnósticos del ATP III para el SM, lo cual constituye el 13 % de la población analizada.
Cuando se comparan ambos grupos, es decir, pacientes con SM y sin este (Fig. 1), se observa que el valor medio del IB fue muy inferior en el primero (1,87, desviación estándar [DE]: 0,65) que en el segundo (4,06; DE: 1,07), con diferencia significativa.
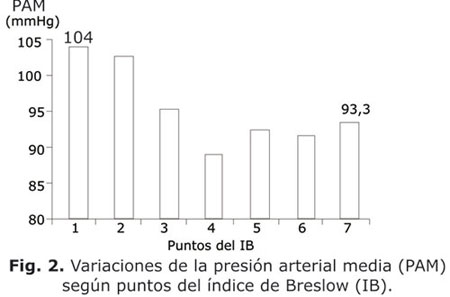
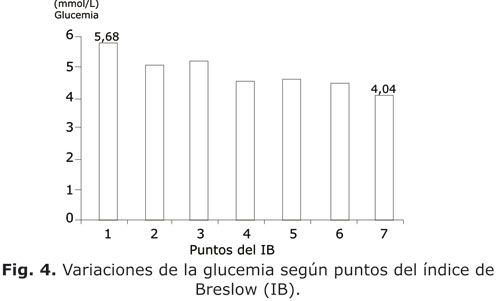
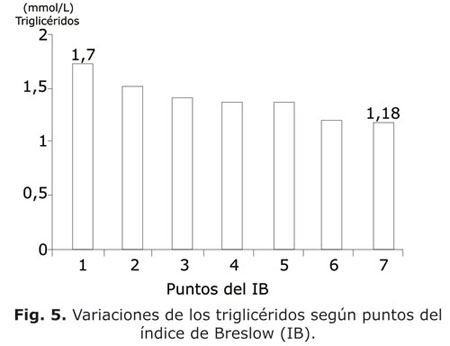
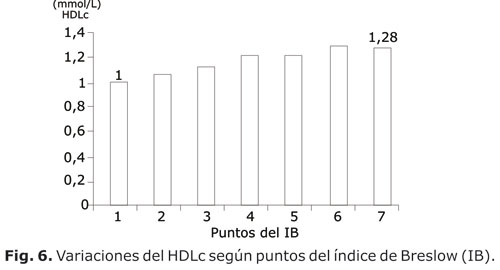
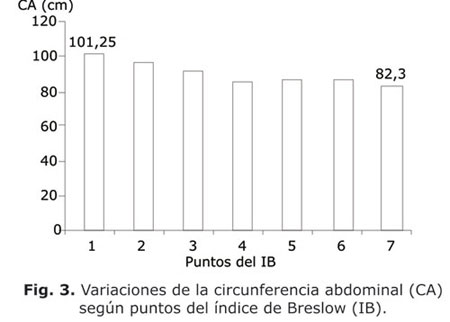
En las figuras 2, 3, 4, 5 y 6 se presenta el comportamiento de las medias de las variables que constituyen criterios diagnósticos del SM en su relación con el puntaje del IB entre todos los sujetos estudiados. En todas las figuras es evidente como las medias de las variables del SM (tensión arterial, circunferencia abdominal, glucemia, triglicéridos y HDLc) variaban en la medida que el puntaje alcanzado en el IB aumentaba de 1 a 7 puntos. En todos los casos ocurrió una tendencia a la disminución de estas medias, excepto con el HDLc en que hubo un incremento. Al comparar las medias entre el grupo con puntaje 1 y el grupo con puntaje 7, hubo siempre diferencias significativas (p< 0,05).
]]>
DISCUSIÓN
En los resultados presentados se han tratado de relacionar los hábitos y estilos de vida con el SM en su conjunto y con los criterios diagnósticos que lo constituyen. Para este fin se utilizó el IB, un sistema de preguntas sencillas que tratan de evaluar diversos aspectos relacionados con hábitos y estilos de vida que tienen que ver con el riesgo vascular. Este índice, validado desde hace más de 30 años de edad14 se caracteriza por su sencillez y demostrada utilidad en los problemas de salud de que se ocupa este trabajo.15 ]]>
La población estudiada de oficiales presentó una prevalencia del SM de 13 %. Aunque no se pretende establecer tasas de prevalencia del SM en este estudio, ya que la población analizada no lo permite, la cifra obtenida es semejante pero ligeramente superior a la reportada en una investigación más amplia efectuada por uno de los autores de este trabajo, también en una población militar, quien encontró un 10,4 %. Cifra semejante se obtuvo en una investigación en una población civil laboralmente activa16 y en personal militar.17Estos porcentajes pueden parecer muy inferiores a los reportados en la literatura internacional,18-20 pero se explican por proceder en este caso de una población laboralmente activa, con límites de edades estrechos y porque las consecuencias del SM (cardiopatía isquémica, enfermedad cerebrovascular, diabetes mellitus, etc.) constituyen muchas veces causa de bajas médicas entre los oficiales.
En la figura 1 se hace evidente que entre los sujetos con diagnóstico de SM se reportan los peores hábitos y estilos de vida, con diferencias significativas de los valores medios de puntos de IB entre ambos grupos (con SM o sin este). Esta figura destaca la importancia de los hábitos y estilos de vida saludables en la génesis del SM, lo cual ha sido reiteradamente señalado en otros estudios.9-11
Tal análisis se refuerza en las figuras 2, 3, 4, 5 y 6, en las cuales se individualizan las diferentes variables que constituyen el SM.
La figura 2 permite asociar los hábitos y estilos de vida no saludables con un deterioro de las cifras de tensión arterial medias y resalta la importancia de mejorar los primeros como terapéutica no medicamentosa en el control de la hipertensión arterial, lo cual es indicado en todas las guías de hipertensión y señalado reiteradamente por diversos autores21,22 con respecto, principalmente a los hábitos dietéticos y la actividad física.
La figura 3 muestra un hecho importante: el vínculo innegable entre los estilos de vida y la grasa corporal. Si se reconoce, como han hecho muchos,23-25 la función del tejido adiposo en la serie de acontecimientos que llevan a la insulinorresistencia, al estado inflamatorio y protrombótico crónicos que constituyen el SM, entonces no hay duda que el estilo de vida es un determinante de primer orden en el desarrollo del síndrome.
La glucemia fue otra variable que se asoció al estilo de vida, aunque moviéndose siempre en valores medios normales. La glucemia es una variable poco confiable para detectar el trastorno subyacente en estos sujetos, ya que la hiperinsulinemia compensadora logra mantener un equilibrio en el metabolismo glucídico hasta etapas más avanzadas. La población estudiada tenía una edad media de 34 años (dato no presentado), es decir, la reserva pancreática para vencer la insulinorresistencia estaba aún intacta. De todas maneras, desde etapas tempranas ya comienzan a existir indicios de un deterioro del metabolismo glucídico que llevará, inexorablemente, a la diabetes mellitus de no corregirse a tiempo los hábitos y estilos de vida nocivos para el funcionamiento endocrino del páncreas.
Los triglicéridos se movieron también acorde con el estilo de vida. Esto es otro hallazgo coherente con los mecanismos fisiopatológicos invocados en el SM muy relacionados con la acumulación central de la grasa y la insulinorresistencia. El sedentarismo y los malos hábitos dietéticos, medidos a través del IB permiten la acumulación de grasa visceral, la cual provoca un aflujo aumentado de ácidos grasos al hígado, con el consiguiente incremento de la síntesis hepática de VLDL ricas en triglicéridos.26 La insulinorresistencia puede favorecer esta hiperproducción de triglicéridos, ya que se conoce que en condiciones fisiológicas, la insulina inhibe la síntesis de VLDL27 al degradar a las apo B.28 Además, la insulinorresistencia disminuye la concentración de la lipoproteínlipasa del tejido adiposo y muscular, impidiendo el aclaramiento de los triglicéridos de la circulación.29 Por tanto, la hipertrigliceridemia es un buen marcador de resistencia a la insulina y uno de los criterios importantes para el diagnóstico del SM.30
Las HDL muestran la progresión inversa esperada, es decir, a medida que mejoran los estilos de vida hay un incremento en sus valores, reforzando la función protectora de un estilo de vida sano. La función protectora de las HDL ha sido reiteradamente señalada. En el SM se halla una disminución de los niveles de HDL. En presencia de hipertrigliceridemia, las HDL disminuyen su contenido en ésteres de colesterol e incrementan su concentración de triglicéridos, lo que las hace más pequeñas y densas. Estos cambios en su composición facilitan que sean retiradas de la circulación, disminuyendo sus niveles.31,32
En la asociación de causalidad entre los hábitos y estilos de vida y el SM puede inferirse que la expresividad clínica del SM y el riesgo vascular (definidos a través del número de criterios diagnósticos que se agrupan en un individuo) se incrementan en la medida que se deterioran los estilos de vida. ]]>
Este estudio presenta algunas limitaciones en su concepción. La ventaja que se le señaló al IB (su sencillez) constituye, a su vez, su principal debilidad ya que puede dudarse que un sistema constituido por solo 7 preguntas que admiten solamente respuestas categóricas (sí o no) mida con precisión algo tan complejo y multidimensional como los estilos de vida saludables. En segundo lugar, hay preguntas que pueden parecer algo ambiguas, por ejemplo, "comer entre comidas", se refiere a la ingestión desordenada de alimentos sin horarios establecidos o pude incluir las meriendas que, en realidad, son recomendadas en los regimenes dietéticos saludables.Sin embargo, los resultados obtenidos son muy coherentes con lo esperado de acuerdo con el estado del conocimiento alrededor del objeto de estudio y permiten concluir que existe asociación entre los hábitos y estilos de vida y la presencia del SM en general y de cada una de sus variables constituyentes, con una evidente relación "dosis-respuesta" entre ambos.
Anexo 1. Criterios diagnósticos de síndrome metabólico según el Adult Treatment Panel III (ATP III)
]]>1. Circunferencia abdominal: > 102 cm (hombres), > 88 cm (mujeres)
2. Presión arterial: > 130/ 85 mmHg.
3. Glucemia: > 6,0 mml/L
4. Triglicéridos: > 1,7 mmol/L
5. HDL: < 1,0 mmol/L (hombres), < 1,3 mmol/L (mujeres)
Anexo 2. Índice de Breslow
1. ¿Ud. desayuna casi todos los días?
2. ¿Ud. participa en actividades deportivas al menos 3 veces por semana?
3. ¿Ud. duerme de 7 a 8 h casi todos los días?
4. ¿Ud. toma bebidas alcohólicas en cantidades menores de 8 oz. a la semana?
5. ¿Ud. evita comer entre comidas?
]]> 6. ¿Ud. evita fumar?7. ¿Ud. mantiene su peso corporal controlado?
Se obtiene un punto por cada respuesta afirmativa (sí) y cero punto por cada respuesta negativa (no). La pregunta 6 significa "fuma o no fuma". La pregunta 7 se responde de acuerdo con el índice de masa corporal: "sí": IMC< 25 kg/m2; "no": IMC= 25 kg/m2.
REFERENCIAS BIBLIOGRÁFICAS
1. de la LLera Suárez E. Modo y estilo de vida. En: Alvarez Sintes R. Temas de Medicina General Integral. Vol I. Salud y Medicina. La Habana: Ed. Ciencias Médicas; 2001. p. 39-41.
2. Yazaki Y, Kadowaki T. Combating diabetes and obesity in Japan. Nature Med. 2006;12:73-4.
3. Martínez Calatrava M, Martínez Larrat MT, Serrano Ríos M. Síndrome de resistencia a la insulina y síndrome metabólico: similitudes y diferencias. Síndrome metabólico: concepto, fisiopatología y epidemiología. Cardiovascular Risk Factors. 2003;12(2):89-95.
4. Helmrich SP, Ragland DR, Leung, RW. Physical activity and reduced occurrence of non-insulin-dependent diabetes mellitus. N Engl J Med. 1991;325:147-52. Available from: http://content.nejm.org/cgi/content/abstract/325/3/147
5. Hu FB, Leitzmann MF, Stampfer MJ. Physical activity and television watching in relation to risk for type 2 diabetes mellitus in men. Arch Intern Med. 2001;161:1542-8. Available from: http://archinte.ama-assn.org/cgi/content/abstract/161/12/1542
6. Manson JE, Nathan DM, Krolewski AS. A prospective study of exercise and incidence of diabetes among US male physicians. JAMA. 1992;268:63-7. Available from: http://jama.ama-assn.org/cgi/content/abstract/268/1/63
7. Laaksonen DE, Lakka HM, Salonen JT. Low levels of leisure-time physical activity and cardiorespiratory fitness predict development of the metabolic syndrome. Diabetes Care. 2002;25:1612-8. Available from: http://care.diabetesjournals.org/content/25/9/1612.full
8. Graff-Iversen S, Skurtveit S, Nybo A, Ross GB. Trends when it comes to occupational physical activity among Norwegians aged 40.42 years during the period 1974-94. Tidsskr Nor Laegeforen. 2001;121:2584-8.
9. Ekelund U, Brage S, Froberg K. TV Viewing and Physical Activity Are Independently Associated with Metabolic Risk in Children: The European Youth Heart Study. PLoS Med. 2006;3(12):e488.
10. Pei-Chia Chang, Tsai-Chung Li, Ming-Tsang Wu. Association between television viewing and the risk of metabolic syndrome in a community-based population BMC Public Health. 2008;8:93.
11. Marshall, SJ; Biddle, SJ; Gorely T. Relationships between media use, body fatness and physical activity in children and youth: A meta-analysis. Int J Obes Relat Metab Disord. 2004;28:1238-46.
12. Hancox RJ, Milne BJ, Poulton R. Association between child and adolescent television viewing and adult health: A longitudinal birth cohort study. Lancet. 2004;364:257-62.
13. Berkey CS, Rockett HR, Gillman MW, Colditz GA. One-year changes in activity and in inactivity among 10- to 15-year-old boys and girls: Relationship to change in body mass index. Pediatrics. 2003;111:836-43.
14. Belloc NB, Brewlow I. Relationship of physical health status and health practices. Prev Med. 1972;1:409-21.
15. Yokohama H, Hirose H, Ohgo H. Associations among lifestyle status, serum adiponectin and insulin resistance. Internal Medicine. 2004;43(6):453-7.
16. del Río A, Ferreira IJ, Casanovas JA. Temas de actualidad en Cardiología preventiva: el síndrome metabólico. Rev Esp Cardiol. 2005;5:13-23.
17. Banduceau B, Gaigts F, Bordier L. Epidemiology of the metabolic syndrome in 2045 French Military personnel (EPIMIL study). Diabetes Metab. 2005;31:353-9.
18. Ford ES, Giles WH, Mokdad AH. Increasing prevalence of the metabolic syndrome among US adults. Diabetes Care. 2004;27:2444-9.
19. Rielly MP, Rider DJ. The metabolic syndrome: more than the sum of its parts? Circulation. 2003;108:1546-51.
20. Balkau BJ, Vernay M, Mhamdi L. The frequency and incidence of the NCEP metabolic syndrome in the French DESIR study. The European Association for the Study of Diabetes. Abstract Volume of 38th Annual Meeting 2002;A15:37.
21. Apple L, Brands M, Daniels S, et al. Approaches to prevent and treat hypertension: A scientific statement from the American Heart Association. Hypertension. 2006;47:296-308.
22. Sarma S, Schulze P. Exercise as a physiologic intervention to counteract hypertension: Can a good idea go bad? Hypertension. 2007;50:294-6.
23. Grundy SM. What is the contribution of obesity to the metabolic syndrome? Endocrinol Metab Clin North Am. 2004;33:267-82.
24. Nakamura H, Ito H, Egam Y et al. Waist circumference is the main determinant of elevated C-reactive protein in metabolic syndrome. Diabetes Res Clin Pract. 2008;79:330-6.
25. Goodpaster BH, Krishanaswami S, Harris TB. Obesity, regional body fat distribution, and the metabolic syndrome in older men and women Arch Intern Med. 2005;165:777-83.
26. Lewis GF, Uffelman KD, Szeto LW, et al. Interaction between free fatty acids and insulin in the acute control of very low density lipoprotein production in humans. J Clin Invest. 1995;95:158-66.
27. Lewis GF, Steiner G. Acute effects of insulin in the control of state. Diabetes Care. 1996;19:390-3.
28. Taghibiglou C, Rashid-Kolvear F, Van Iderstine SC. Hepatic very low density lipoprotein-ApoB overproduction is associated with attenuated hepatic insulin signaling and overexpression of protein-tyrosine phosphatase 1B in a fructosefed hamster model of insulin resistance. J Biol Chem. 2002;277:793-803.
29. Eckel RH, Yost TJ, Jensen DR. Alterations in lipoprotein lipase in insulin resistance. Int J Obes Relat Metab Disrod. 1995;19:S16-S21.
30. Eckel RH, Grundy SM, Zimmet PZ. The metabolic syndrome. Lancet. 2005;365:1415-28.
31. Murakami T, Michelagnoli S, Longhi R. Triglycerides are major determinants of cholesterol esterification/transfer and HDL remodeling in human plasma. Arterioscler Trhomb Vasc Biol. 1995;15:1819-28.
32. Brinton EA, Eisenberg S, Breslow JL. Increased apo A-I and apo A-II lipoprotein-cholesterol levels with or without hypertriglyceridemia. J Clin Invest. 1991;87:536-44.
]]>
Recibido: 22 de octubre de 2009.
Aprobado: 26 de noviembre de 2009.
Tte. Cor. Tomás Ariel Lombardo Vaillant. Instituto Superior de Medicina Militar "Dr. Luis Díaz Soto". Ave Monumental y Carretera de Asilo. Habana del Este. La Habana, Cuba. Correo electrónico: tomariel@infomed.sld.cu ]]>