ARTÍCULO ORIGINAL
Modelling the evolution of Meningococcal disease in Cuba from 1998-2005
Diseño del modelo de la enfermedad meningocócica en Cuba en el período 1998-2005
]]>
Joke BilckeI; Antonio PérezII; Lizet SanchezIII; Ziv ShkedyIV
I Master of Science, Biostatistician, Center for Statistics, Hasselt University, Agoralaan_building D 3590 Diepenbeek, and Centre for Health Economics Research and Modelling of Infectious Diseases, Antwerp University, Belgium.
II Medical Doctor. PhD, Epidemiologist. Instituto de Medicina Tropical "Pedro Kourí" (IPK). Ciudad de La Habana, Cuba.
III Master of Science. PhD, Epidemiologist. IPK. Ciudad de La Habana, Cuba.
IV Professor. PhD, Applied Mathematics. Center for Statistics, Hasselt University, Belgium.
Key words: Bacterial infection, Haemophilus influenzae, Neisseria meningitidis, season, Generalized Linear Models.
INTRODUCCIÓN: la meningitis bacteriana es una enfermedad letal que se deriva de la infección de las meninges por bacterias. En Cuba, existen alrededor de 500 casos de meningitis bacteriana todos los años. Sin embargo, una pequeña parte de estos casos es provocada por las bacterias Neisseria meningitidis como enfermedad meningocócica (formas clínicas: meningitis, septicemia, o ambas cosas), a pesar de que la enfermedad está comtemplada en el programa de control por vacunación desde 1989.
OBJETIVOS: 1. modelar cómo varía el número de casos nuevos de la enfermedad meningocócica en Cuba en el transcurso del tiempo, 2. investigar si los modelos de evolución de la meningitis con el tiempo pueden mejorarse mediante la adición de predictores.
MÉTODOS: se emplean modelos lineales generales con la distribución de Poisson. ]]>
RESULTADOS: los nuevos casos de la enfermedad aparecen modelados en forma de función cuadrática en el tiempo, con un número elevado de casos en el verano en comparación con los surgidos en el invierno. Por otra parte, la cantidad de casos está en dependencia de la edad. El alto número de casos en la segunda mitad de 1989 podría explicarse parcialmente por el decrecimiento de los casos de meningitis por H. influenzae, tras el programa de inmunización llevado a cabo en ese tiempo.
CONCLUSIONES: el modelo del número de nuevos casos de la enfermedad meningocócica indicó que depende de la estación del año y de la edad. Asimismo deben explorarse con mayor profundidad otras posibles variables predictivas, de manera que pueda mejorarse el modelo a los efectos de un pronóstico.
Palabras clave: infección bacteriana, Haemophilus influenzae, Neisseria meningitidis, estación del año, modelos lineales generalizados.
INTRODUCCIÓN ]]>
Bacterial meningitis is a life-threatening illness resulting from bacterial infection of the meninges, i.e. the membranes which entirely encase the brain and the spinal cord, and/or the fluid between these coverings ("cerebrospinal fluid"). The bacteria reside in the secretions of nose and mouth and are transmitted by air. The number of carriers is often much larger than the number of cases, i.e. more than 25 % of people can be carrier without the presence of the disease. The incidence is about 4.5-10 cases per 100 000 persons a year, most of them being children younger than 5 years.1,2In Cuba there are about 500 cases of bacterial meningitis every year. The three most important bacterias causing meningitis and/or invasive infection are Neisseria meningitidis ("Meningococcal disease"), Streptococcus pneumoniae ("Pneumococcal meningitis") and Haemophilus influenzae ("H. influenzae meningitis").3 Only Pneumococcal meningitis is not yet under vaccination control. A vaccination campaign for Meningococcal disease (only against serogroup B and C) was conducted at 1989. It consisted of vaccinating all people under 20 years old. At 1991 a program started to vaccinate all infants under one year old.4,5 For H. influenzae meningites, a vaccination campaign and program was started at 1999. The campaign consisted of vaccinating one year old children with one dose during year 1999 (full vaccination consists of three doses of the vaccine). The program started with vaccinating younger than one years old with 1, 2 or 3 doses during 1999. From then on, all younger than one year old children are vaccinated with 3 doses.6
The nationwide free health service and the National Epidemiological Surveillance System in Cuba allows that meningitis or septicaemia infections are very accurately reported. The data are sent to the Instituto de Medicina Tropical "Pedro Kourí" (IPK) and have already been used to get a first insight on the impact of the vaccination programs for Meningococcal and H. influenzae meningitis.4-6 However, until now, studies on the temporal aspects of meningitis were predominantly descriptive. Incidence densities are plotted over time, and summary statistics are calculated to test for temporal patterns.4,6-8 Although such exploratory studies provide important information about the disease, there is a need to actually try to describe the process generating the observed meningitis cases over time. In case of Meningococcal disease, such data modelling would provide more detailed insight in how the disease evolves when it is under vaccination control. Therefore the first objective of this study is to model how the number of new cases of Meningococcal disease in Cuba changes over time.
Furthermore there is a need to improve such time model by adding important predictor variables, because this can make future prediction possible. Predicting how the number of Meningococcal disease cases will evolve over time, may allow deciding if for instance new boosters of vaccination are needed. Some evidence already exists that the number of cases is affected by age, with the disease occurring predominantly in young children.1,2 Moreover, Meningococcal disease seems to occur more frequently in fall, winter and spring.1-3,7 Also, the presence of one type of bacterial meningitis might influence the occurrence of another type of bacterial meningitis. It can be insightful to investigate this. Hence, the second objective of this study is to investigate if the model of evolution of Meningococcal disease over time can be improved by adding predictors, such as season, age and number of H. influenzae meningitis cases.
METHODS
Data collection
We used the data on Meningococcal disease reported from 1998 to 2005 by a questionnaire to the National Epidemiological Surveillance System. For each patient, date of disease acquisition, age and agent that caused the meningitis were recorded (i.e. N. meningitidis, H. influenzae or S. pneumoniae). In Cuba medical assistance is free, and hospital admission is necessary for these health problems, which avoid cases not to be reported.6 ]]>
Data analysis
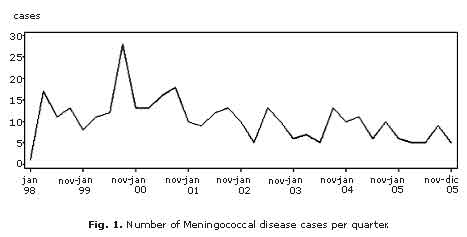
The number of Meningococcal disease cases was grouped per quarter, so that the number of cases per quarter was sufficiently large to be able to model them statistically. Winter was divided in two quarters, with the first group of cases occurring between November and January, and the second group of cases occurring between february and april. Third quarter (may to july) and fourth quarter (august to october) correspond to summer.
For five Meningococcal disease cases, only the year of disease acquisition was reported (which was for all of them 1998), so that these data could not be included in the analysis. This means that the number of cases in 1998 (quarter 1 to 5) was underestimated. The first quarter (january 1998) and the last quarter (november and december 2005) are underestimated, because they contain cases of only one respectively two months, instead of three months.
Five age groups (<1, 1-4, 5-14, 15-64 and >64 years old) were considered in the analysis.
Exploratory data analysis
Descriptive statistics, the means of cases and standard error (SE) were calculated and quarterly number of Meningococcal disease cases were plotted over the different years to explore trends in time. Number of cases were also plotted against time for the five different age groups to investigate differences between these age groups. Finally, quarterly number of Meningococcal disease cases were plotted together with quarterly number of H. influenzae cases to compare differences and similarities of their evolution over time.
Modelling the number of Meningococcal disease cases over time ]]>
The number of new Meningococcal disease cases in Cuba was modelled over time using a linear regression model. The model was fitted with the GENMOD procedure in SAS. Because of count data, a Poisson distribution was specified with a log link. However, for count data, Poisson is often too simplistic: it assumes that the mean is equal to the variance although often the variance is found to be larger (i.e. overdispersion). To explore overdispersion, we looked if the deviance/df value differed substantially from one. If there was some indication for overdispersion, we fitted the same model but specifying a negative binomial distribution.Negative binomial regression is an extension of the Poisson regression model that has an extra parameter (the dispersion parameter k-1) and allows the variance to be different from the mean. Estimating the dispersion parameter also helps to summarize the extent of overdispersion: the greater k-1 the greater the overdispersion compared to the ordinary Poisson regression.9
Models were evaluated using plots of observed and predicted values, and using the deviance statistic G².
The parametric linear regression model was fitted using the time variable as a continuous covariate. The time variable goes from quarter 1 (january 1998) to quarter 33 (november-december 2005). Quadratic and cubic terms of the time variables were added and removed when shown not significant.
To account for the seasonal cycles, a binary variable was added to the model (0= winter and 1= summer).10
Next, the predictor variables "age" and "hicount" (count of H. influenzae cases) were introduced into the model, together with their quadratic terms all possible interactions between the predictors. Then the model was simplified by removing one by one non-significant 3-way interaction terms, next non-significant 2-way interaction terms, and at last non-significant variables, which were not part of significant 2-way interaction terms.
The same procedure was used for modelling the data without the data of the first and last quarter. The numbers of meningitis cases of the first and last quarter are underestimated, and therefore we investigated their impact.
Because of the very low number of cases in the oldest age group, we also repeated the analysis with the two oldest age groups grouped together.
]]>
RESULTS
Exploratory data analysis
The mean number of quarterly Meningococcal disease cases in Cuba is 10.3 + 0.9 (N= 33, variance= 25.1), with minimum 1 and maximum 28. An elevated number of cases in the second half of 1999 and seasonal cycle, more cases in summer, were observed (fig. 1).
The number of Meningococcal disease cases over time differed by age groups (fig. 2). The mean number of cases, the increase in the second half of 1999 and the amplitude of the seasonal oscillations seem to be age dependent. The mean number of Meningococcal disease cases per quarter, per age group is 2.0 + 0.1 [N= 165 (= 33 quarters *5 age groups), variance= 3.4], with minimum 0 and maximum 11.
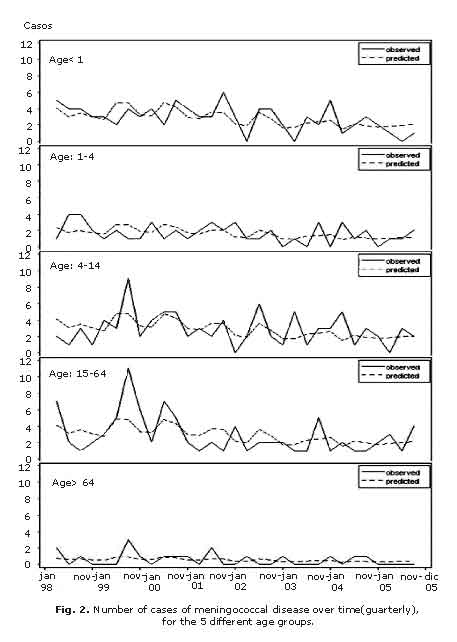
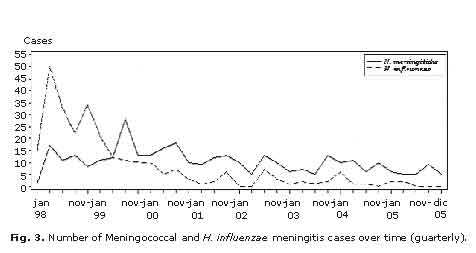
Figure 3 shows that the number of Meningococcal and H. influenzae meningitis change very similarly over time, except for the period 1998-2000, before starting H. influenzae vaccination.
Generalized linear models for the number of Meningococcal disease cases over time ]]>
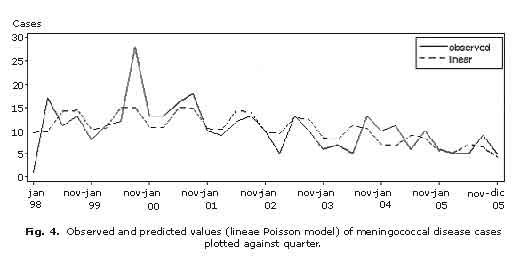
The evolution of Meningococcal disease was modelled by a general linear model with Poisson distribution and log link function, as a quadratic function over time, with an elevated number of cases in summer compared to winter (fig. 4). Let Y (t) be the number of Meningococcal disease cases,
Y (t) ~ Poisson [m (t)],
Here, m (t) is the mean number of Meningococcal disease cases at time t. The mean structure of the model is given by
Log [m (t)]= 2.574 + 0.029 *time -0.002 *time² -0.343 *season,
Here, season is an indicator variable which take the value of 1 in the winter and 0 elsewhere and the time unit is the quarter (the first quarter in 1988 is equal to 1).
 ]]>
]]>
However, the initial model did not fit the data well (G²= 45 df= 29) and therefore the mean structure was adjusted and the quarterly number of new cases of H. influenzae meningitis was added as a covariate to the model. The final model contained the variables time (linear and quadratic terms) quarterly number of new cases of H. influenzae meningitis, (linear and quadratic terms), season (winter or summer) and 2-way interaction between time and quarterly number of new cases of H. influenzae meningitis (G²= 144, df= 144). Table present the parameter estimates for the final model.
The G²/df value of 1.0000 does not indicate overdispersion. The estimated model indicates that the way the number of Meningococcal disease cases changes over time, depends on the number of H. influenzae meningitis cases. The mean number of cases is also different for each age group. The mean number of cases per quarter is lowest for people older than 64, however it is highest (almost 4 cases each quarter) in age groups <1, 5-14 and 15-64. The observed and predicted values for meningococcal cases over time are shown in figure 4.
DISCUSSION
One of the advantages of the generalized linear model with Poisson distribution is that the relationships between the predictors and the number of Meningococcal disease cases are quantified, for instance we get real estimates for mean number of cases in summer compared to winter. Moreover, we get an assessment of goodness-of-fit of the model. This means we get an formal measure about how good the number of Meningococcal disease cases is explained by the predictors we thought to be important, i.e. about how important those predictors really are.
A big disadvantage of our generalized linear model with Poisson distribution, is that it is based on very few cases. Due to adding age (a patient characteristic) as a categorical covariate in the model, the data get stratified, and the number of cases per strata becomes smaller. This is one of the drawbacks of the current dataset. It only consists of data on patients with meningitis, hence each time we want to add a patient characteristic as covariate, the data will be stratified further. The more strata, the less patients per stratum, so that statistical analysis becomes more difficult (models become less powerful) and in the end impossible. An alternative approach to test for an extensive number of possible patient characteristics as predictors, is to do a cross-sectional study and compare the characteristics of meningitis patients with the ones of healthy people.
In contrast with this study, previous studies showed an elevated number of Meningococcal disease cases in fall, winter and spring.1-3,7 It would be interesting to explore more deeply if and which seasonal characteristics cause the elevated number of cases. Moreover, maybe the oscillation pattern seen (fig. 1) is not due to seasonal oscillations. A way to explore this could be to use an alternative approach to model the cycles (without implying a seasonal cycle) such as the use of time series.10
This study is also the first one to show a relationship between meningitis cases caused by different bacteria's. The number of Meningococcal disease cases was quite elevated at august-october 1999. This peak could be partially explained by the decrease in number of H. influenzae meningitis cases at the same time. However, recall that the data we used were scarce, and the model fit was not very satisfactory so that this result should be interpreted with care. From about may-july 2000 the two diseases evolve very similarly. This suggests that the changes in cases over time from then on are not due to bacteria specific characteristics, but rather to more general demographic and/or temporal (e.g. weather) factors. ]]>
For the future, it would be interesting to improve our regression model in order to be able to predict number of new Meningococcal disease cases. At this moment, our model is not suitable because, 1. the goodness-of-fit is to small, suggesting some important predictors are still missing, 2. the model shows first an increasing than a decreasing number of cases in time. This means that eventually, the number of cases will be predicted to be zero, i.e. that the disease dies out. This may not be a good representation of reality. Possibly, a model which models cycles around the same intercept over time could be more realistic, and of more use for prediction purposes compared to our model that fits the existing data from 1998 to 2005.Moreover, our study shows that, when a vaccination program is started for one bacterial type, it might be important to assess its possible impact on other types of bacterial meningitis or invasive clinical forms.
Also, it could be of interest to evaluate the model using data from countries than Cuba (for instance Brazil or African countries with a higher incidence of Meningococcal disease cases).
ACKNOWLEDGEMENT
We thank the department of Epidemiology of (IPK) and the Center for Statistics (Hasselt University) for support and advice. Flemish Interuniversity Council (VLIR) and the Centre for Statistics funded this project.
]]>
REFERENCES
1. Griffiss McL. Meningococcal infections. In: Wilson, editor. Harrison's principles of internal medicine. New York: Mc Graw-Hill; 1991. p. 590-9.
2. Harter DH, Petersdorf RG. Bacterial meningitis and brain abscess. In: Wilson, editor. Harrison's principles of internal medicine. New York: Mc Graw-Hill; 1991. p. 2023-7.
3. Dickinson FO, Pérez AE. Las meningoencefalitis bacterianas en la población infantile cubana: 1998-2000. Rev Cubana Pediatr. 2002;74(2):106-14.
4. Pérez A, Dickinson F, Baly A, Martinez R. The epidemiological impact of antimeningococcal B vaccination in Cuba. Mem Inst Oswaldo Cruz. 1999;94(4):433-40.
5. Pérez A, Dickinson F. Resultados del programa nacional de inmunización antimeningocócica BC en menores de 1 año en Cuba. Rev Cubana Pediatr. 1998;70(3):133-40.
6. Dickinson FO, Pérez AE, Galindo MA, Quintana I. Impacto de la vacunación contra Haemophilus influenzae tipo b en Cuba. Rev Panam Salud Publica. 2001;10(3):169-73.
7. Cordeira OR, Barreras RJ, Colls1 CP, Fernandez AA. La estacionalidad de la enfermedad meningocócica en menores de 1 año. Cuba, 1983-1990. Rev Cubana Med Trop. 1995;47(2):108-13.
8. Dickinson FO, Pérez AE. Bacterial meningitis in children and adolescents: an observational study based on the national surveillance system. BMC Infect Dis. 2005;5:103.
9. Agresti A. Categorical Data Analysis. New York: John Wiley & Sons; 2002.
10. Kuhn L, Davidson, LL, Durkin MS. Use of poisson regression and time series analysis for detecting changes over time in rates of child injury following a prevention program. Am J Epidemiol. 1994;140(10):943-55.
]]>
Recibido: 12 de mayo de 2008.
Aprobado: 25 de agosto de 2008.
M.C. Lizet Sánchez. Instituto de Medicina Tropical "Pedro Kourí". AP 601, CP 11300, Ciudad de La Habana, Cuba. Correo electrónico: lsanchez@ipk.sld.cu ]]>