Dra. Mary Brenda Manteiga Rodríguez, Dra. Judith Falcón Caballero, Dra. Isis Montesino Álvarez y Dra. Gladys Soto Rodríguez
Se incluyeron en el estudio 35 pacientes con una edad comprendida entre 13 y 78 años. La pérdida del globo ocular es traumatizante para el paciente y constituye un fracaso para el oftalmólogo. Tras la evisceración, el implante de hidroxiapatita con la colocación de una prótesis ocular, aporta beneficios estéticos para el paciente. En todos ellos, se practicó la cuadrisección con doble cobertura escleral, que es una de las técnicas quirúrgicas de mayor difusión en la actualidad, con un tiempo de seguimiento de 2 a 30 meses, permitiendo colocar implantes independientemente del tamaño de la cavidad y disminuyendo el riesgo de exposición de estos.
Palabras clave: Evisceración, implante de hidroxiapatita y cobertura escleral.
La pérdida del globo ocular producida por traumas, enfermedades, o como secuelas quirúrgicas en el tratamiento de tumores y otras afecciones es un problema que afecta a una parte considerable de la población. La restauración de estos defectos ha merecido la atención de investigadores, médicos y especialistas dedicados a este campo desde tiempos remotos, por lo que se ha prestado especial interés al desarrollo tanto de biomateriales como de procederes quirúrgicos y de otro tipo que permitan la adecuada rehabilitación.1
Hace más de 100 años que comenzaron a utilizarse los implantes orbitarios para tratar de lograr una mejoría cosmética en los pacientes que perdían el globo ocular, al restablecer en ellos el volumen de la cavidad y proporcionarles una mayor motilidad a las prótesis; los primeros consistían en esferas huecas de cristal y las utilizó Mülles en 1884.2
Desde entonces, la forma y su composición han variado mucho, entre los materiales utilizados en su confección se han tenido sustancias orgánicas (cartílagos, esclera, hueso de cabeza de fémur de recién nacido) e inorgánicas (cristal, tantalio, plástico, silicona y recientemente la hidroxiapatita y el pórex).
Para conseguir un buen resultado estético se debe colocar un implante del tamaño adecuado para que la proyección anteroposterior del contenido orbitario sea unos 3 mm menos que el ojo contralateral, de manera que queden iguales al colocar una prótesis del grosor óptimo.3 Esto es difícil de conseguir cuando la cavidad escleral del ojo eviscerado es pequeña. Hace 2 años, en el Centro de Investigaciones Médico-Quirúrgicas se comenzó a realizar la evisceración con implante de hidroxiapatita mediante la técnica de cuadrisección con doble cobertura escleral.
A continuación se describe la técnica, con la que, además de poder colocar un implante del tamaño deseado, se cubre la parte anterior con 2 capas de esclera, intentando disminuir aún mas las posibilidades de exposición.
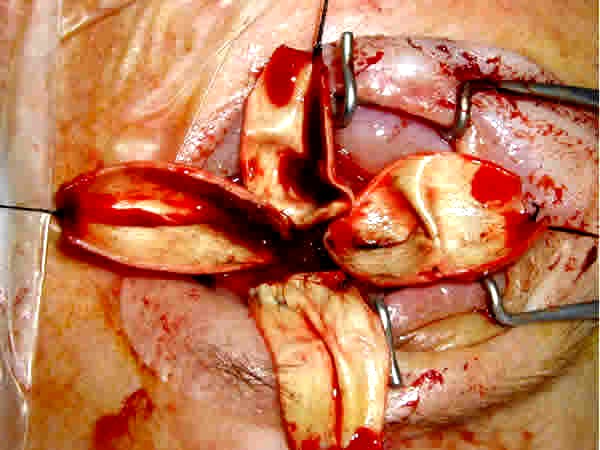
La técnica quirúrgica se hizo mediante anestesia general (fig.).
Fig. Técnica quirúrgica.
En primer lugar, se hace una peritomía conjuntival en limbo. Se separa mediante disección roma la Tennon y conjuntiva del globo ocular, llegando lo más atrás posible. Se individualizan con ganchos de estrabismo los 4 músculos rectos, y se liberan las uniones fibrosas entre ellos y entre cada uno y la cápsula de Tennon, para luego poder desplazar hacia delante los fragmentos esclerales con su músculo correspondiente sin dificultad. Se realiza una queratectomía completa, posteriormente se hacen 4 incisiones en dirección anteroposterior, que parten del borde anterior de la esclera justo en los vértices de los 4 cuadrantes. Estas incisiones se unen unas con otras lo más cerca posible del nervio óptico, de manera que se deja dividida la esclera en 4 pétalos, cada uno de los cuales lleva insertado su músculo recto. Se introduce el implante del tamaño deseado. Se colocan los 4 fragmentos esclerales sobre el implante, traccionando de ellos hacia delante, ayudándonos con pinzas sin dientes que presionen el implante y eviten que se venga hacia delante.
Se suturó con Vicryl 5/0, en primer lugar los pétalos que llevan los músculos verticales y a continuación los que llevan los músculos horizontales, de esta manera se produce primero una herida horizontal, sobre ella una vertical y, por último, otra horizontal del cierre de la Tennon y conjuntiva, disminuyendo las posibilidades de exposición. Se hace una buena disección entre Tennon y conjuntiva, suturando siempre los 2 planos por separado, con Vicryl 6/0 sutura continua. Al finalizar la cirugía se coloca un conformador.
Para la recolección de la información se tomaron los datos de las historias clínicas. Como medidas de resumen se utilizaron porcentajes.
En este estudio se incluyen 35 pacientes a los que se les ha realizado una evisceración, 14 mujeres (40 %) y 21 hombres (60 %).
Las indicaciones para la cirugía fueron ojos ciegos, dolorosos o que producían alteración estética.
La patología previa que condujo a su situación actual fue:
]]> Traumatismos: 26 (74,28 %).Durante el seguimiento (entre 2 y 30 meses) no ha habido ninguna complicación derivada de la cirugía. En ningún caso hubo exposición ni desplazamiento del implante. El resultado cosmético ha sido bueno sin enoftalmos ni hundimiento del surco palpebral superior significativos.
Desde que en 1985, Perry comenzó a utilizar hidroxiapatita como implante que sustituye al globo ocular en evisceraciones y enucleaciones, se han utilizado diferentes materiales4-12 y diferentes técnicas quirúrgicas encaminadas a colocar un implante que produzca pocas complicaciones y con el que se consigan buenos resultados estéticos.
Cuando se realiza una evisceración en ojos con ptisis bulbi se ha de modificar y ampliar la cavidad escleral disponible porque si la prótesis colocada es muy pequeña se producirá un enoftalmos, un hundimiento del surco palpebral superior y una ptosis palpebral por falta de apoyo, y el resultado estético no será nada satisfactorio para el paciente.13 Cuando el volumen del implante es muy pequeño, el protesista intenta compensarlo utilizando una prótesis más grande, pero esto produce por un lado una disminución importante en su movilidad, y a largo plazo una pérdida del fondo de saco inferior y una ptosis del párpado inferior debido al traumatismo producido por el exceso de peso de esta.
La complicación más temible es la erosión de los tejidos que cubren el implante con la consiguiente exposición de este y, si no se soluciona pronto, puede producirse una infección que obliga a su retirada.14,15
La causa de esta complicación, generalmente, es una cobertura del implante a tensión o una erosión de la misma por un roce traumático.16,17
Se han descrito diferentes técnicas de evisceración para poder colocar prótesis grandes sin que los tejidos que cubren la prótesis estén suturados a tensión. Se han descrito esclerotomías de descarga, esclerotomías posteriores completas que permiten avanzar la esclera todo lo necesario y secciones esclerales en 2 o en 4 fragmentos,18,19 como en este caso. Pero esta técnica quirúrgica, igual que las anteriores, permite colocar un implante del tamaño deseado sin tensión en los tejidos que la cubren, además, se consigue una doble cobertura escleral del implante, de manera que es muy poco probable que la superficie del implante llegue a erosionar por roce las 2 capas de esclera que le cubren.20,21
Se concluye que la evisceración con doble cobertura escleral es una técnica quirúrgica que permite colocar implantes biointegrables del tamaño deseado, independientemente de la cavidad escleral de que se disponga, y disminuye las posibilidades de exposición.
Key words: Evisceration, hydroxyapatite implant and scleral coverage.
1. Pérez G, González R, Acosta L, Solano M, Oliva J, Rodríguez J. Hidroxiapatita porosa HAP-200 como bioimplante esférico integrado en el anoftalmos quirúrgico. Rev Cubana Oftalmol 1998;11(1):5-13.
2. Martínez N, Falcón I, Herrera M, Gómez C, Agramonte I, Samara A, et al. Implantes orbitarios de HAP-200. Experiencia en 100 casos. Rev Cubana Oftalmol 2002;15(1):10-9.
3. Jordon DR, Allen LH, Ells A, Gilberg S, Browasteins S, Munro S. The use of vycril mesh (poliglacten 910) for implantation of hydroxyapatite orbital implants. Ophthalmol Plast Reconstr Surg 1991;11(2):95-9.
4. lapper SR,
5. Kao LY. Polytetrafluoroethylene as a wrapping material for a hydroxyapatite orbital implant. Ophthal Plast Reconstr Surg 2000;16:286-8.
6. Kaltreider SA. The ideal ocular prosthesis: analysis of prosthetic volume. Ophtal Plast Reconstr Surg 2000;16:388-92.
7. Long JA, Tann III TM, Girkin CA. Evisceration: a new technique of trans-scleral implant placement. Ophthal Plast Reconsr Surg 2000;16:322-5.
8. Custer PL, Reistad CE. Enucleation of blind, painful eyes. Ophthal Plast Reconstr Surg 2000;16:326-9. 9. Jordan DR, Klapper SR. A new titanium peg system for hydroxyapatite o orbital implants. Ophthal Plast Reconstr Surg 2000;16:380-7.
10. Hsu WC, Green JP, Spilker MH, Rubin PA. Primary placement of a titanium motility post in a porous polyethylene orbital implant: animal model with quantitative assessment of fibrovascular ingrowth and vascular density. Ophthal Plast Reconstr Surg 2000;16:370-9.
11. Choi JC, Iwamoto MA, Bstandig S, Rubin PA, Shore JW. Medpor Motility Coupling Post: a rabbit model. Ophthal Plast Reconstr Surg 1999;15:190-201.
12. Mules PH. Evisceration of the globe with artificial vitreous. Tr
13. Button R. A buried type of integrated orbital implant. Am J Ophthalmol 1956;41(2):313-5.
14. Soll DB. A new type of evisceration implant. Am J Ophthalmol 1971;71(3):763.
15. llis OH, Levy R. A new magnetic orbital implant. Am Arch Ophthalmol 1956;56(3):352-60.
16. Prizvbyla VA, Piana FG la. Complications associated with use of tantalum mesh covered implants. Ophthalmology 1982;89:121-3.
17. Oonin JF, Henderson JW, Grindlay JH. Evisceration of the eye with implantation of polyvinyl sponge. Am Arch Ophthalmol 1955;54(3):373-80.
18. Perry CA. Advances in enucleation. Ophthalmic plastic and reconstructive surgery. Ophthalmol Clin North Am 1991;4(1):173-82.
19. Kostick DA, Linberg JV. Evisceration with hydroxyapatite implant.Surgical tecnique and review of 31 case reports. Ophthalmology 1995;102:1542-8.
20. Yang JG, Khwarg SI, Wee WR, Kim DM, Lee JH. Hydroxyapatite implantation with scleral quadrisection after evisceration. Ophthalmic Surg Lasers 1997;28:915-9.
21. Toledano N, Prada C. Manejo de la cavidad anoftálmica. Madrid:Digi-Art; 2002. p.31-42.
Recibido: 28 de octubre de 2005. Aprobado: 23 de marzo de 2006.
Dra. Mary Brenda Manteiga Rodríguez. Centro de Investigaciones Médico-Quirúrgicas. Ave 216 y 11-B, Siboney, municipio Playa, Ciudad de La Habana,Cuba. Teléf.:2715022