PRESENTACIÓN DE CASO
Escleritis posterior: a propósito de un caso
Posterior scleritis: a propos of a case
Dra. Isabel Ambou Frutos,I Dra. Ángeles Valdés Petitón,II Dra. Carmen de Prada Sánchez,II Dra. Lisette Pérez Sotolongo,I Dra. Sandra Carvajal ReyesI
]]>
I Instituto Cubano de Oftalmología "Ramón Pando Ferrer". La Habana, Cuba.
II Facultad de Ciencias Médicas "Calixto García". La Habana, Cuba.
RESUMEN
Las enfermedades inflamatorias de la esclera son infrecuentes. Involucran tanto la esclera como la epiesclera y se caracterizan por su cronicidad, dolor y por ser una causa potencial de ceguera. Su asociación con enfermedades sistémicas, frecuentemente de causa autoinmune, y la aparición de graves complicaciones oculares, conllevan una terapia sistémica agresiva con antinflamatorios no esteroideos, corticoesteroides y agentes inmunosupresores, los cuales se pueden utilizar solos o combinados. Presentamos el caso de un paciente masculino de 37 años de edad quien acudió al Cuerpo de Guardia por dolor ocular intenso, asociado a ojo rojo, disminución de la agudeza visual y cifras elevadas de tensión ocular del ojo derecho, a quien le fue diagnosticada una escleritis posterior.
Palabras clave: antinflamatorios no esteroideos, escleritis, epiescleritis.
The inflammatory diseases of the sclera are uncommon. They involve both the sclera and the episclera and are characterized by chronic nature, pain and potential cause of blindness. Their association with systemic diseases, frequently autoimmune ones, and the occurrence of serious ocular complications lead to applying aggressive systemic therapy with non-steroid antinflammatory drugs, corticosteroids and immunosuppressive agents, which can be administered alone or combined. This is a 37 years-old patient who went to the emergency service because he suffered intense ocular pain associated to red eyes, reduction of visual acuity and high ocular pressure values in his right eye. He was finally diagnosed with posterior scleritis.
Key words: non-steroidal anti-inflammatory drugs, scleritis, episcleritis.
INTRODUCCIÓN
La escleritis se define como un proceso inflamatorio que afecta a la esclera. Se caracteriza por ser generalmente crónico, doloroso, destructivo y causante potencial de ceguera. Está frecuentemente asociado a enfermedades sistémicas, y requiere tratamiento general para controlar la inflamación subyacente. No obstante, formas leves de escleritis deben ser diferenciadas de las episcleritis. Esta entidad envuelve a la esclera anterior en un 85-90 %; sin embargo, también puede afectar a la esclera posterior, de manera aislada o en conjunción con una escleritis anterior.1 La escleritis posterior se define como la inflamación de la esclera posterior a la ora serrata.2 Se puede presentar en cualquier grupo etario, aunque es frecuentemente diagnosticada entre los 30 y los 60 años. Asimismo, existe una leve predilección por el sexo femenino.1 Es bilateral en más del 50 % de los pacientes, pero generalmente comienza por un solo ojo.2 Al contrario que en las episcleritis, existe una común asociación con enfermedades sistémicas. La más frecuente es la artritis reumatoide, con el 33 % de pacientes afectos. La patogenia de la escleritis viene caracterizada por una vasculitis mediada inmunológicamente, en la que las células inflamatorias son activadas por inmunocomplejos depositados o por antígenos locales aún desconocido. Por ejemplo, en la escleritis necrotizante, existe una evidencia consistente que indica que el depósito de inmunocomplejos en la pared vascular da lugar a una necrosis fibrinoide de esta, oclusión trombótica de los vasos junto con una respuesta inflamatoria crónica en el tejido escleral.3,4 Nos proponemos presentar este caso, ya que las escleritis tienen una baja incidencia entre las enfermedades oculares, sobre todo al tratarse de un paciente masculino y estar asociada a una enfermedad sistémica como la toxoplasmosis.
CASO CLÍNICO
Se presenta el caso de un paciente varón de 37 años de edad con antecedentes patológicos personales de hipertensión arterial descompensada, quien acude a nuestro servicio por dolor ocular punzante en ojo derecho, que se asocia a ojo rojo y disminución de la agudeza visual. Al examen oftalmológico se constata:
Medios
- No celularidad en el humor acuoso ni en el vítreo.
Fondo de ojo por oftalmoscopia binocular indirecta
Ojo derecho: disco óptico con excavación 0,5 hiperémico, con rechazo nasal vascular, con capilares dilatados y discreto borramiento hacia los polos y nasal, ingurgitación venosa con cruces arteriovenosos con depresión intensa, signo de gunn, edema retinal con pliegues en la limitante interna en polo posterior, pérdida del brillo foveal, no se aprecian ni exudados ni hemorragias, hacia temporal inferior se observa área de retina con mayor edema retinal sugestivo de desprendimiento seroso de retina.
Días después, aún sin comenzar el tratamiento con esteroides sistémicos, aparecen en el fondo de ojo hemorragias profundas en número de 5 de aproximadamente de medio y un diámetro papilar en los cuadrantes superiores:
Ojo izquierdo: disco óptico con excavación 0,4, con rechazo nasal vascular, cruces arteriovenoso patológico y signo de gunn. Se le indican complementarios que incluyen: ]]>
- Hemograma completo: Hb 13,9; leucocitos totales 12,0 x 10 L con 0,87 polimorfonucleares y 0,13 linfocitos; conteo de plaquetas: 322 x 10/L.
- Eritrosedimentación: 18 mm.
- Glicemia: 5,3 mmol/L.
- Creatinina: 100 mmol/L.
- células LE: negativas. ]]>
- ANA: negativo.
- PPD: 4 mm.
- Serología: negativa.
- VIH: negativo.
- Rx AP y lateral: negativos. ]]>
- Antígeno de superficie: negativo.
- IFI/ELISA para toxoplasma: pendiente de resultado.
- TAC de órbita ojo derecho, cortes axiales y coronales: informa lesión polipoidea en seno maxilar de base de 17 mm; no otras alteraciones.
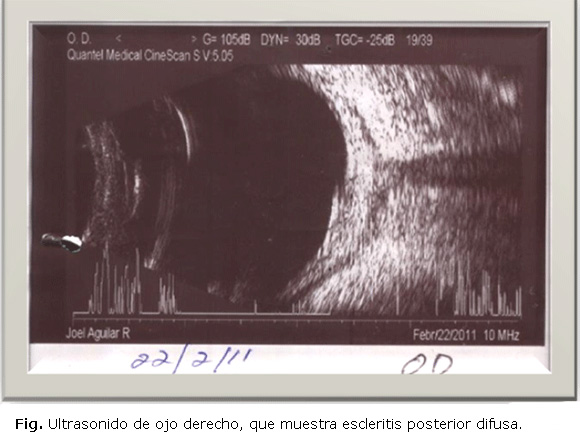
- Ultrasonido ojo derecho: se observa engrosamiento del complejo retina coroides, aumento de la reflectividad del espacio de la tenon por infiltración, y también el signo característico en "T". Vítreo libre de ecos. Cristalino in situ. Se informa como una escleritis posterior difusa (Fig.).
- Ultrasonido abdominal: Normal.
Se interconsulta con los servicios de Medicina Interna, Reumatología y Otorrinolaringología, y no se encuentran elementos positivos de enfermedad sistémica asociada. Se decidió entonces, previo control medicamentoso de la tensión arterial, imponer tratamiento con esteroides sistémicos y tópicos, asociados a hipotensores oculares, y se observó entonces una respuesta favorable al tratamiento impuesto. Durante el seguimiento hubo una evolución satisfactoria con una disminución lenta y progresiva de los esteroides, hasta llegar a los 30 mg de prednisona oral, en que presentó una recaída del cuadro, que coincidió con la llegada del resultado del IFI para toxoplasma,el cual arrojó títulos de 1:256. Se decidió entonces asociar el tratamiento antitoxoplásmico (sulfaprim y azitromicina), y elevar nuevamente la dosis de esteroides orales a la dosis previa efectiva. Hasta el momento la evolución ha sido muy favorable, y no se han presentado nuevas recaídas.
La escleritis posterior se define como la inflamación de la esclera posterior a la ora serrata, la cual puede comprometer estructuras oculares contiguas, incluyendo la coroides, la retina, el nervio óptico, los músculos extraoculares y los tejidos orbitarios.5 Diversos estudios previos sobre series de pacientes con escleritis afirman que de 40-50 % de estos pacientes presentarán una enfermedad sistémica infecciosa o reumatológica asociada (aproximadamente el 5-10 % tendrán una enfermedad infecciosa y el 30-40 % será reumática). Vitale y Sainz de la Maza describen que infecciones por protozoos, como la Acanthamoeba, el Microsporidium y el Toxoplasma gondii, también han sido identificados como agentes causales en pacientes con severa escleroqueratitis, esclerouveítis con desprendimiento de retina y escleritis posterior respectivamente.5 A menudo el diagnóstico de una enfermedad sistémica asociada a escleritis, dicta su tratamiento. Así pues, una escleritis infecciosa requeriría terapia con agentes antibióticos o antivirales; sin embargo, una escleritis asociada a una vasculitis sistémica se trataría con fármacos inmunosupresores para intentar solucionarla. Por tanto, el diagnóstico de patología sistémica asociada se convierte en un aspecto crucial en el manejo de un paciente con escleritis. Aunque algunas series documentan la presencia de una enfermedad sistémica, ninguna evalúa la aparición de las patologías sistémica y ocular ni documentan los resultados de la evaluación diagnóstica inicial de estos pacientes.6-12 En un estudio reciente se estudiaron 243 pacientes con escleritis. Se presentó un amplio rango etario (5 a 93 años, con una media de 52 años). Se afirmó que la enfermedad infecciosa más comúnmente asociada fue el herpes zoster oftálmico y la afectación reumática más frecuente fue la artritis reumatoide. La vasculitis sistémica fue la segunda causa sistémica asociada a escleritis y se diagnosticaron todos los tipos de vasculitis en los pacientes evaluados. La media de seguimiento fue 1,7 años con un rango de 0 a 16,6 años.13 Asimismo se apreciaron diversos aspectos clínicos que conferían mayor riesgo de padecer una enfermedad sistémica asociada a la patología ocular, de modo que los varones eran más susceptibles que las mujeres de padecer una enfermedad infecciosa (OR= 0,34; p= 0,035), mientras que las mujeres presentaban mayor predisposición a enfermedades reumáticas (OR= 1,98, p= 0,027). El único tipo de escleritis claramente asociada a patología sistémica fue la escleritis nodular anterior (OR= 3,08; p= 0,037). La queratitis intersticial se objetivó principalmente en pacientes con una enfermedad infecciosa (OR= 4,80; p= 0,004), así como la uveítis (OR= 3,75; p= 0,010). La escleritis bilateral se asoció fundamentalmente con enfermedades reumatológicas (OR= 1,78; p= 0,032).13 En algunos casos en que exista positividad de pruebas diagnósticas para una determinada entidad, pensamos que es adecuado instaurar tratamientos empíricos, a pesar de que no exista evidencia clínica o un diagnóstico de certeza, ya que es fundamental un control adecuado del cuadro escleral por el riesgo ocular que conllevan y las graves complicaciones de algunos subtipos.14
REFERENCIAS BIBLIOGRÁFICAS
1. Benson WE. Posterior scleritis. Survey Ophthalmol. 1988;32(5):297-316.
2. Whitcup SM. Scleritis. In: Nussenblatt RB, Whitcup SM, editors. Uveitis fundamental and clinical practice. Elsevier: Mosby; 2004. p. 287-90.
3. Meyer PA, Watson PG, Franks W, Dubard P. Pulse inmunosupresive therapy in the treatment of inmunologically induced corneal and scleral disease. Eye. 1987;1:487-95.
4. Watson PG. The nature and treatment of scleral inflammation. Trans Ophthalmol Soc UK. 1982;99:257.
10.Tuft SJ, Watson PG. Progression of scleral disease. Ophthalmology. 1991; 98:467-71.
11. Mc Clusky PJ. Posterior scleritis: clinical features, systemis associations and outcome in a large series of patients. Ophthalmology. 1999;166:2380-6.
12. Sainz de la Maza M, Foster CS. Scleritis associated with systemic vasculitis diseases. Ophthalmology. 1995;102:687-92.
13. Karamursel E, Thorne J. Evaluation of patients with scleritis for systemic disease. Ophthalmology. 2004;111:501-5.
14. Fernández-Baca G, Losada Castillo MJ, Pérez Barreto L, Martin Barrera F. Escleritis asociadas a enfermedades sistémicas. Arch Soc Canar Oftal. 2005 [citado 16 de mayo de 2014]. Disponible en: http://www.oftalmo.com/sco/revista-16/16sco17.htm
]]>
Recibido: 5 de febrero de 2014.
Aprobado: 19 de junio de 2014.
Dra. Isabel Ambou Frutos. Instituto Cubano de Oftalmología "Ramón Pando Ferrer". Ave. 76 No. 3104 entre 31 y 41 Marianao, La Habana, Cuba. Correo Electrónico: Isabel.ambou@infomed.sld.cu