PRESENTACIÓN DE CASO
Enfermedad de Vogt-Koyanagi-Harada y rehabilitación visual
Vogt-Koyanagi-Harada disease and visual rehabilitation
MSc. Mayrelis Quintero Busutil, MSc. Daysi Caridad Vilches Lescalle, MSc. Yurania Bueno Arrieta, MSc. Susana Rodríguez Masó, MSc. Carlos Alberto Perea Ruíz, Lic. Miladis Paz Lorenzo
Instituto Cubano de Oftalmología "Ramón Pando Ferrer". La Habana, Cuba.
]]>
RESUMEN
La enfermedad de Vogt-Koyanagi-Harada es una entidad infrecuente, multisistémica, de etiología desconocida, presuntamente autoinmune, caracterizada por panuveítis granulomatosa crónica bilateral y difusa, acompañada de participación tegumentaria, neurológica y auditiva, que afecta con mayor frecuencia la raza no caucasiana y, por lo general, a mujeres. Se presenta generalmente entre los 20-50 años de edad. Su incidencia varía geográficamente. Se estima que el 25 % de los pacientes con esta enfermedad son ciegos legales; que el 25 % puede presentar baja visión y el 50 % agudeza visual mayor de 20/50. Se presenta una paciente de 50 años de edad con antecedentes de enfermedad de Vogt-Koyanagi-Harada, de 8 años de evolución, quien ha llevado tratamiento con antinflamatorios esteroideos sistémicos e inmunosupresores, así como terapia de apoyo con antinflamatorios esteroideos tópicos y ciclopléjicos. Acudió a la consulta de baja visión y se le realizó examen oftalmológico completo, estudios complementarios y se rehabilitó mediante el uso de ayudas ópticas y no ópticas para lograr el mayor aprovechamiento de su resto visual.
Palabras clave: enfermedad de Vogt-Koyanagi-Harada, ayuda óptica, ayuda no óptica, baja visión, ciego legal, rehabilitación visual.
ABSTRACT
Vogt-Koyanagi-Harada (VKH) is a rare, multisystemic, allegedly autoimmune disease of unknown etiology. It is characterized by chronic bilateral granulomatous and diffuse panuveitis, accompanied by tegumentary, neurological and hearing impairments that often affect the non-Caucasians and usually women. It usually occurs in the 20-25 years age group and its incidence varies with the geographic location. It is estimated that 25% of the patients with this disease are legally blind, the other 25% may have low vision and 50% present with visual acuity over 20/50. There is a 50 years-old patient with a history of Vogt - Koyanagi - Harada disease for 8 years. He had been treated with systemic steroid anti-inflammatory drugs and immunosuppressive therapy as well as supporting therapy with topical and cycloplegic steroid anti-inflammatories. The patient had gone to the low vision service looking for rehabilitation. He was performed a complete eye examination, supplementary studies and he was finally rehabilitated through the use of optical and non-optical aids in order to maximize his remaining vision.
Key words: Vogt-Koyanagi-Harada disease, optical aid, non-optical aid, low vision, legally blind, visual rehabilitation.
]]>
INTRODUCCIÓN
Se estima que la uveítis es causa del 10 % del déficit en el mundo occidental y que alrededor del 35 % de los pacientes con uveítis presentan baja visión o ceguera legal.1 La enfermedad de Vogt- Koyanagi-Harada (VKH) es una entidad infrecuente, multisistémica, de etiología desconocida, presuntamente autoinmune, caracterizada por una panuveítis granulomatosa crónica, bilateral y difusa, acompañada de participación tegumentaria, neurológica y auditiva.1-3 Afecta con más frecuencia a grupos étnicos de piel oscura (asiáticos, hispanos, nativos americanos) y es menos común en caucasianos y africanos.1,3 Las mujeres por lo general están más afectadas que los hombres, excepto en Japón.1 Su incidencia varía geográficamente. En EE.UU. se estima que sea del 1-4 % de todas las uveítis que se remiten1,3 y en Japón entre 6,7 y 9,2 %.2,4,5 Se presenta casi siempre entre los 20 y 50 años.3 Se estima que el 25 % de los pacientes con esta enfermedad son ciegos legales; que el 25 % puede presentar baja visión y el 50 % agudeza visual mayor de 20/50.1
La enfermedad presenta 4 formas clínicas:
1. Prodrómico: existe presencia de síntomas neurológicos. LCR + (> 80 % hasta 8 semanas). En el 75 % de los casos existen síntomas del VIII par craneal. Tiene una duración de 3 a 5 días.1,2 ]]>
2. Uveítico: presencia de síntomas oculares (visión borrosa 70 % casos), uveítis anterior o posterior, desprendimiento seroso, edema del nervio óptico por engrosamiento coroideo, que es el primer signo.1,2
3. Crónico/convaleciente: es más frecuente en asiáticos; el tiempo de evolución es entre 2-3 meses; el fondo de ojo en "puesta de sol", presencia de nódulos de Dalen-Fuchs. El primer signo en instalarse es el signo de Sugiura, y existen focos de hiperpigmentación, zonas de atrofia focal y epitelio pigmentario de la retina periféricas, así como instalación de signos tegumentarios (menos frecuentes en hispanos).1,2 ]]>
4. Recurrente: es la forma clínica más frecuente. Se presenta con una uveítis anterior granulomatosa refractaria a tratamiento antinflamatorio esteroideo. Rara vez se presenta como una uveítis posterior con la existencia de nódulos iridianos, atrofia iridiana, cataratas, glaucoma, alteraciones del epitelio pigmentario de la retina y neovascularización coroidea.1,2
El diagnóstico de VKH es esencialmente clínico; pero en pacientes con presentación sin cambios extraoculares, la angiografía fluoresceínica y con indocianina, la tomografía de coherencia óptica, la punción lumbar y la ultrasonografía, pueden ser usados como pruebas confirmatorias.1-6
Los criterios diagnósticos de la enfermedad recientemente revisados,7,8 basados en las características clínicas, definen tres categorías: completo, incompleto y probable.1,8,9 A pesar de la forma de la enfermedad, las características o rasgos esenciales para el diagnóstico incluyen los tres primeros criterios: 1) la ausencia de historia de trauma ocular penetrante, 2) la no evidencia de otra enfermedad ocular o sistémica y 3) la bilateralidad. Los criterios 4 y 5 son los hallazgos neurológicos y auditivos y los tegumentarios. Los pacientes con VKH completo presentan los cinco criterios. Los que tienen VKH incompleto tienen los tres primeros y alguna manifestación extraocular, ya sea neuroauditiva o tegumentaria. Los que presentan VKH probable solo tienen los tres primeros criterios.1,8
El tratamiento debe ser temprano y agresivo con esteroides sistémicos para así disminuir el riesgo de complicaciones oculares causantes de deterioro visual.1,3 Los inmunosupresores son drogas de segunda línea y son muy útiles en los pacientes que no toleran los esteroides o en los casos en que las múltiples recurrencias hayan provocado resistencia a la terapia esteroidea.1 La asociación de ambos medicamentos es igual de efectiva.10,11
Los pacientes discapacitados visuales por enfermedad de Vogt-Koyanagi-Harada presentan afectación de la visión periférica y la central con predominio de una u otra, por lo que su rehabilitación visual constituye un gran reto para enseñarles a aprovechar al máximo su remanente visual.
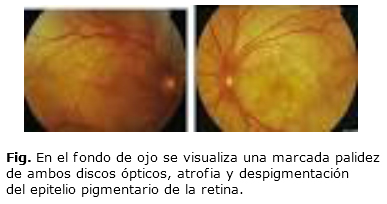
Se presenta una paciente femenina de 50 años de edad, mestiza, ama de casa, con antecedente de enfermedad de Vogt-Koyanagi-Harada de 8 años de evolución y baja visión, quien acudió a la consulta para rehabilitación visual. La paciente ha llevado tratamiento con antinflamatorios esteroideos sistémicos, inmunosupresores, terapia de apoyo con antinflamatorios esteroideos tópicos y ciclopléjicos. Fue atendida en el Servicio de Baja Visión del Instituto Cubano de Oftalmología "Ramón Pando Ferrer" en abril del año 2013, por presentar disminución de la visión en ambos ojos y dificultad para orientarse. Muestra estudios que señalan afectación de sus nervios ópticos y en menor medida del área macular (Fig.).
Su principal motivación es mejorar su orientación y movilidad para realizar las tareas del hogar y la lecto-escritura. Presenta en el ojo derecho (OD) una agudeza visual sin corrección de 0,1 y en ojo izquierdo (OI) de 0,2 y refracción dinámica OD-4,00; OI-4,00, con una agudeza visual mejor corregida de 0,3 en ambos ojos. Teniendo en cuenta sus principales motivaciones desde la primera consulta, se indicó microscopio de +10,00 en ambos ojos que le permitía leer letras de tamaño 0,4 a una distancia de 10 cm; se fatigó rápidamente con una velocidad de lectura de 60 palabras por minutos, además con lupa de apoyo de 3x, que le permitió leer letras tamaño 0,6 a 13 cm. Se recomendó mantener los caminos libres y evitar mover muebles en la casa.
Se indicaron los ejercicios de fijación y localización. Luego de tres sesiones de rehabilitación, con la misma ayuda óptica pero con iluminación y empleo del tiposcopio, se logró una mayor velocidad de lectura (100 palabras por minuto), sin fatiga. Refirió además comodidad en el desempeño de sus funciones de la vida diaria, y en el desarrollo de habilidades en su orientación y movilidad.
DISCUSIÓN
La enfermedad Vogt-Koyanagi-Harada es poco frecuente en la práctica médica diaria, pero ante la sospecha se hace necesario confirmar el diagnóstico y distinguirla de entidades clínicamente similares.12 El diagnóstico temprano y el tratamiento con un régimen agresivo esteroideo, disminuyen las manifestaciones sistémicas, las recurrencias y el riesgo de complicaciones. Se logra un mejor pronóstico visual en los pacientes.13-15 Se plantea que alrededor del 60 % de los pacientes con enfermedad de Vogt-Koyanagi-Harada quedan con agudeza visual de 0,5 o mejor si se realiza el diagnóstico a tiempo y el tratamiento oportuno; pero en caso de que la agudeza visual quedara comprometida, menor o igual de 0,3, a percepción de luz en su mejor ojo con corrección óptica, es un paciente con baja visión y una opción de tratamiento sería la rehabilitación visual que no es más que el conjunto de procesos encaminados a obtener el máximo aprovechamiento del resto visual con el fin de potencializar el resto visual y alcanzar los objetivos establecidos por el paciente a través del entrenamiento con el uso de ayudas ópticas y no ópticas.16,17
En la literatura revisada no se encontró ningún reporte acerca de la rehabilitación visual en pacientes con diagnóstico de enfermedad de Vogt-Koyanagi-Harada. Es válido señalar que dentro de las enfermedades uveales y su rehabilitación visual pudimos solo consultar una presentación de caso sobre toxoplasmosis ocular, que reportaba resultados alentadores,18 dada la baja incidencia de esta enfermedad y teniendo en cuenta la importancia en el manejo oportuno de esta para disminuir el número de personas con baja visión, y la orientación a quienes la presentan para enseñarles a aprovechar al máximo su remanente visual.
Nos propusimos presentar este caso para demostrar que con la rehabilitación visual mediante el empleo de ayudas ópticas y no ópticas se puede lograr una adecuada velocidad de lectura y comodidad en el desempeño de las funciones en las actividades de la vida diaria; insertarse a la sociedad como un ser biopsicosocial con una mejor calidad de vida,15,16 y apoyar a todos los pacientes con baja visión.
REFERENCIAS BIBLIOGRÁFICAS
1. American Academy of Ophthalmology. Intraocular inflammation and uveitis. EE.UU.: American Academy of Ophthalmology; 2008.
]]>2. Onho-Matsui K, Horie S, Mochizuki M. Primary Stromal Choroiditis. Vogt-Koyanagi-Harada (VKH) Disease. En: Gupta A, Gupta V, Herbort CP, Khairallah M. Uveitis text and imaging. New Delhi: Jaypee Brothers; 2009. p. 529-39.
3. Tesavibul N. Vogt-Koyanagi-Harada Syndrome. En: Foster CS, Vitale AT. Diagnosis and treatment of uveitis. Philadelphia: Saunders; 2001. p. 748-54.
4. Sukavatcharin S, Tsai JH, Rao NA. Vogt-Koyanagi-Harada disease in Hispanic patients. Int Ophthalmol. 2007;27(2-3):143-8.
5. Goto H, Mochizuki M, Yamaki K, Kotake S, Usui M, Ohno S. Epidemiological survey of intraocular inflammation in Japan. Jap J Ophthalmol. 2007;51(1):41-4.
6. Nussenblatt RB. Vogt-Koyanagi-Harada Syndrome. En: Nussenblatt RB, Whitcup SM. Uveitis: fundamental and clinical practice. Philadelphia: Mosby; 2004. p. 324-36.
7. Kiyomoto C, Imaizumi M, Kimoto K, Abe H, Nakano S, Nakatsuka K. Vogt– Koyanagi–Harada disease in elderly Japanese patients. Int Ophthalmol 2007; 27:149-53.
]]>8. Perente I, Utine CA, Cakir H, Kaya V, Tutkun IT, Yilmaz OF . Management of ocular complications of Vogt-Koyanagi-Harada syndrome. Int Ophthalmol. 2009;29(1):33-7.
9. Fardeau C, Tran TH, Gharbi B, Cassoux N, Bodaghi B, Le HP. Retinal fluorescein and indocyanine green angiography and optical coherence tomography in successive stages of Vogt-Koyanagi-Harada disease. Int Ophthalmol. 2007;27(2-3):163-72.
10. Yamamura K, Mori K, Hieda O, Kinoshita S. Anterior segment optical coherence tomography findings of acute angle closure glaucoma in Vogt-Koyanagi-Harada disease. Jap J OphthalmoL. 2008;52(3):231-2.
11. Tsai JH, Sukavatcharin S, Rao NA. Utility of lumbar puncture in diagnosis of Vogt-Koyanagi-Harada disease. Int Ophthalmol. 2007;27(2-3):189-94.
12. Ya-Ling Guo YL, Du Y, He JF. Correlation between sunset glow fundus and initial dosage of corticosteroid in patients with Vogt-Koyanagi-Harada disease. Am J Ophthalmol. 2009;147(5):946.
]]>13. Liu X, Yang P, Lin X, Ren X, Zhou H, Huang X, et al. Inhibitory effect of cyclosporin A and corticosteroids on the production of IFN-y and IL-17 by T cells in Vogt-Koyanagi-Harada syndrome. Clin Inmunol. 2009;131(2):333-42.
14. da Silva FT1, Damico FM, Marin ML, Goldberg AC, Hirata CE, Takiuti PH, et al. Revised diagnostic criteria for Vogt-Koyanagi-Harada disease: considerations on the different disease categories. Am J Ophthalmol. 2009;147(2):339-45.
15. Tugal-Tutkun I, Ozyazgan Y, Akova YA, Sullu Y, Akyol N, Soylu M, et al. The spectrum of Vogt-Koyanagi-Harada disease in Turkey. Int Ophthalmol. 2007;27(23):117-23.
16. Barañano Gl. Atención en baja visión. Madrid: ONCE; 2008.
17. OMS. Visión 2020. El derecho a la visión. Iniciativa mundial para la eliminación de la ceguera evitable. IAPB, 2006-2011; 2008.
]]>18. Ramos AE. Toxoplasmosis ocular y rehabilitación visual. Presentación de un caso. Revista Habanera de Ciencias Médicas. 2013;12(1):48-56.
Recibido: 2 de diciembre de 2014.
Aprobado: 3 de enero de 2015.
Dra. Mayrelis Quintero Busutil. Instituto Cubano de Oftalmología "Ramón Pando Ferrer". Ave. 76 No. 3104 entre 31 y 41 Marianao, La Habana, Cuba. Correo electrónico: mayrelisquintero@infomed.sld.cu