PRESENTACIÓN DE CASO
Síndrome de Chandler
Chandler's syndrome
MSc. Yurisván Escalona Ballester,I Dra.Yaquelín Ortiz Ávila,II Dr. Esmel A. Meneses Leyva,I Dra.Yadira Mendoza Rodríguez,II Dr. Nelson A. Fernández MoralesII
]]> I Policlínico "27 de Noviembre". Antilla, Holguín, Cuba.
RESUMEN
El síndrome de Chandler es una de las variaciones clínicas del síndrome iridocorneoendotelial, donde el denominador común es una alteración del endotelio corneal cuyo diagnóstico es, en ocasiones, muy difícil de realizar por la complejidad y la variabilidad de sus signos y síntomas. Se presenta una paciente de 67 años con disminución importante de la visión del ojo izquierdo. A la exploración existía un edema corneal severo, una midriasis pupilar, una corectopia leve hacia el sector temporal con tracción iridiana hacia el ángulo y sinequias anteriores angulares en el lado de la corectopia. La realización de un recuento endotelial demostró alteraciones cuali y cuantitativas del endotelio en el ojo izquierdo. Se concluyó que la microscopia especular es fundamental para el diagnóstico y la evaluación en casos sospechosos de síndrome de Chandler.
Palabras clave: Chandler, síndrome iridocorneoendotelial, microscopia especular.
Key words: Chandler, iridocorneal endothelial syndrome, specular microscopy.
INTRODUCCIÓN
El síndrome de Chandler fue descrito por Calves Chandler al observar un patrón de ojo rojo sin dolor y cierres intermitentes del ángulo iridocorneal, lo que desencadena episodios de hipertensión ocular y se resuelve con miótico y otros antihipertensivos oculares, así como espontáneamente; pero puede ser recurrente y llegar a la atrofia óptica.1,2 Afecta, con una relación de 8:1, a mujeres con respecto a hombres entre las edades de 40 y 60 años sin antecedentes de afección ocular. Puede ser adquirido y unilateral. Aunque se trata de una enfermedad poco frecuente, hasta el 50 por ciento desarrolla glaucoma de difícil control por sinequias anteriores periféricas o por recubrimiento de la malla trabecular.3,4 En todas las variaciones clínicas de síndrome iridocórneo-endotelial (ICE) está presente la anomalía del endotelio corneal,4-6 que puede ser asintomático u originar un edema corneal, más frecuente en síndrome de Chandler, en ocasiones agravado por la tensión ocular del ojo izquierdo (PIO) elevada.4,5 La microscopia especular revela una anormalidad difusa, varios grados de pleomorfismo, pérdida de márgenes hexagonales, y en ojo contralateral una leve disminución del recuento endotelial, así como pleomorfismo celular medio, casi siempre asintomático.5,6 La atrofia del iridiano está ausente en alrededor del 60 % de los casos y en los restantes su gravedad es variable. La corectopia es leve o moderada.7 El glaucoma suele ser menos grave que en los otros dos síndromes, y en el momento de la presentación la tensión ocular en el ojo izquierdo puede ser normal.8-10
PRESENTACIÓN DEL CASO
Mujer de 67 años quien acudió a la consulta del Cuerpo de Guardia del Servicio de Oftalmología, remitida por su área de salud por la pérdida visual lenta y progresiva del ojo izquierdo (OI), sin antecedentes oftalmológicos personales ni familiares de interés. En la exploración oftalmológica la agudeza visual del ojo derecho (OD) fue de 0,5; en el ojo izquierdo llamó la atención el edema corneal severo (en este momento ya con córnea transparente), acompañado de ojo rojo y de hipertensión ocular luego de las 72 horas de evolución. Presentaba además corectopia en el ojo izquierdo hacia el sector temporal y cierta tracción del iris hacia ese lado, así como midriasis media y ectropion uveal (Fig. 1).
]]>
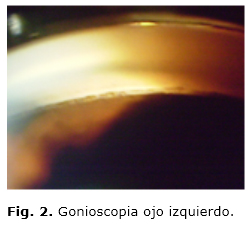
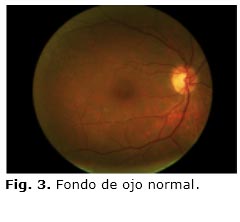
La tensión ocular fue de 12 mmHg en el ojo izquierdo (OI) y a las 72 horas se elevó a 54 mmHg. En el ojo izquierdo se observó gonioscopia, trabeculum hiperpigmentado, el ángulo grado III-grado IV (Fig. 2), el ángulo grado I-grado II y cierre angular de hora 1 a hora 4. Ante la sospecha de un síndrome iridocórneo-endotelial (ICE) se realizó una microscopia endotelial donde se observó en el ojo izquierdo un endotelio con pleomorfismo de 30,0 % y polimegatismo de 73,1 %. En el ojo derecho se pudo observar endotelio normal (Fig. 3).
DISCUSIÓN
Para llegar al diagnóstico del síndrome se tuvo en cuenta el cuadro clínico, que puede ser variable o incompleto, y se realizaron una serie de exámenes complementarios que, en este caso, fueron de gran importancia para poder establecer la conducta correcta. Los resultados fueron los siguientes: proteína C reactiva y factor reumatoideo, negativos; doppler carotídeo y ultrasonografía ocular, normales. En la microscopia especular con modificaciones y en la gonioscopia se obtuvo cierre angular parcial por sinequias. Al alta hospitalaria se logró en la operada la tensión ocular en 10, y la agudeza visual en 0,15 sin corrección y Asintomática. Al año de evolución del posoperatorio la paciente estuvo asintomática, el ojo blanco, tranquilo y adelfo, sin síntomas ni signos. La agudeza visual fue de 0,1 sin corrección y la tensión ocular de 12 mmhg. Además se obtuvo trabeculectomía (TBT) al año de evolución del posoperatorio. En estas pudimos observar midriasis media, iridectomía permeable, bula de filtración funcional, pigmentos iridianos en conjuntiva, atrofia iridiana y no ectropión uveal.
En el caso de la paciente estudiada, las células ICE tienen el aspecto de células endoteliales anormales pero relativamente regulares, que recuerdan la arquitectura normal del endotelio. Estos hallazgos pueden representar las fases iniciales o menos avanzadas de la enfermedad, tal y como apunta la publicación de Chiou9. En otros pacientes el endotelio aparece muy desorganizado, con múltiples células irregulares de núcleo hiperrefringente y abundante presencia de estructuras hiperrefringentes. Suele tratarse de pacientes con mayor tiempo de evolución, lo cual podría apoyar la teoría de que las células ICE son el resultado de una metaplasia endotelial.
Alvarado11 relaciona el síndrome ICE con la infección por el virus del herpes simple en 16 de 25 pacientes afectados, lo cual podría corresponder al "segundo suceso". Blair12 y Eiferman13 reportan el caso de un paciente afectado de iridosquisis y queratocono, y apuntan en la misma dirección al señalar el origen común de las estructuras afectadas. Menezo14 realiza la presentación de un caso en el 2002 de atrofia esencial progresiva de iris bilateral.
Otros autores publican un caso clínico con esa asociación. Plantean que los signos clínicos del paciente les permitió realizar el diagnóstico de atrofia esencial del iris con afectación endotelial y queratocono-asociación, que es excepcional en la literatura. En el ojo izquierdo los hallazgos en la microscopia especular muestran una alteración endotelial subclínica.15,16
Las posibilidades que nos ofrecen nuevos métodos diagnósticos, como la microscopia especular y la topografía de elevación, propiciarán que puedan diagnosticarse cada vez más estas asociaciones patológicas. Además, los avances en genética molecular nos aportarán en un futuro una valiosa información para comprender mejor las enfermedades que son causadas por alteraciones en la diferenciación de la cresta neural (neurocristopathies) y poder disponer así de mayores opciones terapéuticas.17,18
REFERENCIAS BIBLIOGRÁFICAS
1. Shields MB. Progressive essential iris atrophy, Chandler's syndrome and the iris nevus (Cogan-Reese) syndrome: a spectrum of disease. Surv Ophthalmol. 1979;24(1):3-20.
2. Huna R, Barak A, Melamed S. Bilateral iridocorneal endothelial syndrome presented as Cogan-Reese and Chandler's syndrome. J Glaucoma. 1996;5(1):60-2.
3. Denis P. Iridocorneal endothelial syndrome and glaucoma. J Fr Ophtalmol. 2007;30(2):189-95.
4. Herde J. Iridocorneal endothelial syndrome (ICE-S): classification, clinical picture, diagnosis. Klin Monbl Augenheilkd. 2005;222(10):797-801.
5. Morris RW, Dunbar MT. Atypical presentation and review of the ICE syndrome. Optometry. 2004;75(1):13-25.
6. Patel A, Kenyon KR, Hirst LW, Quigley HA, Stark WJ, Meyer RF, et al. Clinicopathologic features of Chandler's syndrome. Surv Ophthalmol. 1983;27(5):327-44.
7. Gogaki E, Tsolaki F, Tiganita S, Skatharoudi C, Balatsoukas D. Iridoschisis: case report and review of the literature. Clin Ophthalmol. 2011;5:381-4.
8. Hemady RK, Patel A, Blum S, Nirankari VS. Bilateral iridocorneal endothelial syndrome: case report and review of the literature. Cornea. 1994;13(4):368-72.
9. Chiou AG, Kaufman SC, Beuerman RW, Ohta T, Yaylali V, Kaufman HE. Confocal microscopy in the iridocorneal endothelial syndrome. Br J Ophthalmol. 1999;83(6):697-702.
10. Teekhasaenee C, Ritch R. Iridocorneal endothelial syndrome in Thai patients: clinical variations. Arch Ophthalmol. 2000;118(2):187-92.
11. Alvarado JA, Underwood JL, Green R, Wu S, Murphy CG, Hwang DG, et al. Detection of herpes simplex viral DNA in the iridocorneal endothelial syndrome. Arch Ophthalmol. 1994;112:1601-9.
12. Blair SD, Seabrooks D, Shields WJ, Pillai S, Cavanagh HD. Bilateral progressive essential iris atrophy and keratoconus with coincident features of posterior polymorphous dystrophy: a case report and proposed pathogenesis. Cornea. 1992;11:255-61.
13. Eiferman R, Law M, Lane L. Iridoschisis and Keratoconus. Cornea.1994;13:78-9.
14. Menezo V, López Torres J, Esteban Masanet M. Microscopia confocal en el síndrome I.C.E. bilateral. Ann Oftalmol. 2002;10(2):94-6.
15. Cavanagh HD, Petroll WM, Alizadeh H, et al. Clinical and diagnostic use of in vivo confocal microscopy in patients with corneal disease. Ophthalmology. 1993;100:1444-54.
16. Minezaki T. Non-Descemet's stripping automated endothelial keratoplasty for bullous keratopathy secondary to iridoschisis. Clin Ophthalmol. 2013;7:1353.
17. Crosby NJ, McDonnell P, Shah P. Iridoschisis associated with nanophthalmos and bullous keratopathy. Int Ophthalmol. 2013;33:83-5.
18. Wang HB, Hu YX, Feng X. Corneal endothelial decompensation secondary to iridoschisis in degenerative myopic eyes: a case report. Int J Ophthalmol. 2012;5:116-118.
Recibido: 2 de diciembre de 2014.
Aprobado: 3 de enero de 2015.
Dra. Yurisván Escalona Ballester. Policlínica "27 de Noviembre". Antilla. Holguín. Cuba. Correo electrónico: yurisvan@antilla.hlg.sld.cu