- Asintomático o con síntomas tolerables por el paciente.
- Ha presentado crisis miasténicas imputables a la enfermedad.
- Necesidad de reajustes terapéuticos motivados por la enfermedad.
- Síntomas intolerables por el paciente.
- Gran frecuencia de crisis miasténicas imputables a la enfermedad.
- Reajustes terapéuticos frecuentes, con escasa o ninguna mejoría clínica.
RESULTADOS
La distribución de los pacientes según la raza es: 21 pacientes (65,7 %) eran mestizos, 9 (28,1 %) pertenecieron a la raza blanca y 2 (6,2 %) a la raza negra.Las características en cuanto a edad y sexo aparecen en la tabla 1. ]]>
| | | | ||||
| | | | ]]> No. | | | |
| | | | | | | ]]> 28,1 |
| | | | | | | |
| | | ]]> 9,4 | | | | |
| | | | | | ]]> 5 | |
| | | | | | | |
| | ]]> 2 | | | | | |
| | ||
| Tratamiento | ]]> de pacientes | |
| Anticolinesterásicos | | |
| Anticolinesterásicos-esteroides | | |
| Timectomía | | |
| Total | | |
| Tiempo transcurrido entre el inicio de los síntomas y el comienzo del tratamiento (meses) | | ||
| Anticolines- terásicos | Anticolinesterásicos- esteroides | Timectomía | |
| ]]>
10 | | | |
| | | ]]> B | |
| | | | |
| | | | |
| | | | |
| | ||||||
| Tipo de tratamiento | | | | |||
| | | | ]]> (%) | | | |
| Anticolinesterásicos | | | | | | |
| Anticolines- | ||||||
| terásicos-esteroides | | ]]> (50,00) | | | | |
| Timectomía | | | | | | ]]> (20,00) |
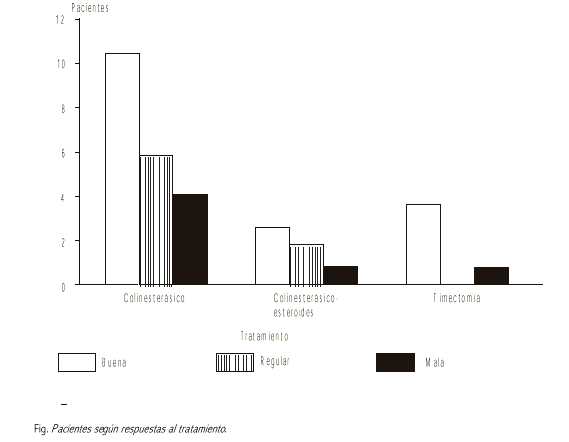
En la tabla 4 y figura se observa que el porcentaje de respuesta buena en los pacientes timectomizados (80 %) supera notablemente a la de los pacientes que recibieron tratamiento médico (52,38 %) para los anticolinesterásicos y 50 % para la combinación anticolinesterásicos-esteroides.
DISCUSIÓN
St Luis24 obtuvo los mejores resultados cuando la operación se realizó en el segundo año de evolución de la miastenia gravis. Emeryk25 postula que la timectomía debe realizarse lo antes posible tras el diagnóstico, pues en su trabajo con 471 pacientes timectomizados observó una marcada mejoría en aquéllos de menos de 1 año de evolución de la enfermedad.Consideramos que los resultados que obtuvimos con el tratamiento quirúrgico se debieron a que estos pacientes fueron operados precozmente y a que la lesión histológica encontrada en todos ellos fue la hiperplasia de la glándula tímica. Papatestas y otros26 en 185 pacientes timectomizados, pudieron observar remisión completa en el 6,5 % de los pacientes con timoma. Esta conclusión se ve reforzada por la de otros autores en su trabajo.27 En cuanto a la causa de la respuesta mala a la timectomía en 1 de los pacientes en que se usó este proceder consideramos que pudo ser por lo prolongado de la evolución de la enfermedad, la lesión de la sinapsis sería ya irreversible, también podría ser porque no se haya extirpado totalmente el tejido tímico, bien por defectos técnicos o porque existía tejido tímico ectópico. Respecto al fracaso del tratamiento quirúrgico, otros autores señalan causas similares.28
SUMMARY
32 patients with diagnosis of myasthenia gravis included in the group II-A according to Osserman and Genkin´s classification, and who received medical attention at the Internal Medicine and Neurology Services of "Celia Sánchez Manduley" Clinical an Surgical Hospital during the last 10 years were studied. The females and the age groups between the second and the fifth decades of life prevailed in the casuistics. A direct relationship was found between the time elapsed since the onset of the first symptoms and the beginning of the treatment and the drug dose used and the clinical response. The response was good in 52.38 % of the patients that were treated with anticholinesterase agents, whereas the response was also favorable in 50 % of the patients who were administered a combination of anticholinesterase agents with steroids. Thymectomy yielded satisfactory results in 80 % of these individuals. It was observed a relationship between the time elapsed since the diagnosis was made, the surgical procedure, and the clinical response.Subject headings: MYASTHENIA GRAVIS/ therapy.
REFERENCIAS BIBLIOGRÁFICAS
- Adams RA. Miastenia grave y formas episódicas de debilidad muscular. En Principios de neurología. La Habana: EditorialCientífico-Técnica, 1982;t 2:1042-80. (Edición Revolucionaria).
- Barraquer Bordas L. Neurología fundamental. 3 ed. Barcelona: Toray, 1976:12-3, 882-3.
- Engel GA. Acquired autoinmune myasthenia gravis. En: Myology basic and clinical. McGrow-Hill, 1986;1925-47. ]]>
- Guthire LB. Myasthenia gravis in the 17 century. Lancet 1943;1:33.
- Elías SB, Appel SH. Recent advances in myasthenia gravis. Life Sci 1976;18:1031.
- Adams RA. Miastenia grave y debilidad muscular episódica. En: Harrison Medicina interna. 5 ed. México, DF: La Prensa Médica Mexicana, 1979;t. 2:2383-5.
- Walker MB. Treatment of myasthenia gravis with physostigmine. Lancet 1934;1:1200.
- Jolly F. Uber myasthenia gravis pseudoparalityca. Berl Klin Wochenschar 1985;32:1.
- Dale H, Feldberg W. Chemical transmision at motor nerve endings in voluntary muscle. J Physiol 1934;81:39.
- Pritchard EAB. The use of prostigmin in the treatment of myasthenia gravis. Lancet 1935;1:432.
- Kjaer, M. Myasthenia gravis and myasthenia syndromes treated with prednisone. Acta Neurol Scand 1971;47:461.
- Johns TR, et al. The syndrome of myasthenia and polimyositis with comments on therapy. Ann NY Acad Sci 1971;183:64.
- Warmols JR, Engel WK. Benefit from alternate day prednisone in myasthenia gravis. N Engl J Med 1972;286:17. ]]> Mann JD. et al. Long term administration of corticosteroids in myasthenia gravis. Neurology 1976;26:729.
- Patten BM. Myastenia gravis: Review fo diagnosis and managements. Muscle nerve 1978;1:190.
- Martens HG, et al. The treatment of severe myasthenia gravis with inmunosuppresive agents. Eur Neurol 1983;2:321.
- Álvarez Sánchez B, y otros. Plasmaféresis en el tratamiento de la miastenia gravis. Rev Clin Esp 1983;170(1-2):61-4.
- Dau PC. Plasmapheresis and inmunosuppresive drug therapy in myasthenia gravis. N Eng J Med 1977;297.
- Kornfeld Pl. Plasmapheresis in myasthenia gravis. lancet 1979;1:190.
- Pila Pérez R, y otros. Resultados de la plasmaféresis en la miastenia gravis refractaria. Rev Cubana Med 1987;26(1):37-41.
- Llorens Figueroa JA, y otros. La timectomía en la miastenia gravis. Rev Cubana Med 1986;25(5):454-63.
- Stites DP. Inmunología básica y clínica. 5. ed. La Habana: Editorial Científico-Técnica, 1985;67:153-5, 1-176. (Edición Revolucionaria).
- Walton JH. Enfermedades del músculo voluntario. En: Price?s Medicina Interna. Barcelona: 1982;t.2:1862-4. ]]> St Luis González R. Valoración de la timectomía en el tratamiento de la miastenia gravis. Rev Cubana Med 1988;27(2):64-72.
- Emeryk B, Strugalska MH. Evaluation of result of thymectomy in myasthenia gravis. J Neurol 1976;211:115.
- Papatestas AE et al. Studies in myasthenia gravis: effects of thymectomy; results on 185 patients with non-thymomatous myasthenia gravis 1941-1969. Am J Med 1971;50:465.
- Genkis G et al. Studies in myasthenia gravis: early thymectomy, electrophysiologic and pathology correlations. Am J Med 1975;58:517.
- Havard CWH. Progress in myasthenia gravis. Br Med J 1973;3:437.
Recibido: 26 de noviembre de 1998. Aprobado: 18 de marzo de 1999.
Dr. César Mustelier Fernández. Hospital Provincial Clinicoquirúrgico "Celia Sánchez Manduley", Servicio de Medicina Interna, Avenida Camilo Cienfuegos, Manzanillo, Granma, Cuba.
]]>