Universidad de Valencia, España
Facultad de Medicina. Departamento de Farmacología
Coinfección virus de inmunodeficiencia humana-virus de la Hepatitis C: hacia un nuevo escenario terapéutico
]]> Human Immunodeficiency Virus–Hepatitis C virus coinfection: towards a new therapeutic scenario
Víctor García-BustosI, Juan Vicente Esplugues-MotaII, Alberto Martí-RodrigoIII
IMédico. Graduado en Medicina por la Universidad de Valencia. Departamento de Farmacología, Facultad de Medicina. Universidad de Valencia, España. bustos@alumni.uv.es
IIMédico. Catedrático de la Universidad de Valencia en el Departamento de Farmacología, Facultad de Medicina. Universidad de Valencia, España. Miembro Científico de la Fundación para el Fomento de la Investigación Sanitaria y Biomédica de la Comunidad Valenciana (FISABIO). Hospital Universitario "Dr.Peset", Valencia, España. Investigador Principal del Centro de Investigación Biomédica en Red Enfermedades hepáticas y digestivas, CIBERehd, Valencia, España. juan.v.esplugues@uv.es
IIIFarmacéutico. Máster en Investigación y Uso Racional de Medicamento. Personal docente e investigador. Departamento de Farmacología, Facultad de Medicina. Universidad de Valencia, España. alberto.marti-rodrigo@uv.es
Introducción: Las terapias contra el virus de la Hepatitis C han evolucionado vertiginosamente con el desarrollo de los antivirales de acción directa (AADs). Los nuevos regímenes han conseguido igualar las tasas de respuesta al tratamiento en los monoinfectados y los coinfectados con VIH, una población tradicionalmente difícil de tratar debido a la elevada morbimortalidad hepática y sistémica, reacciones adversas e interacciones medicamentosas. ]]>
Objetivo: Analizar las opciones farmacoterapéuticas más modernas disponibles para los pacientes coinfectados con VIH y VHC, con énfasis en los nuevos antivirales de acción directa, a fin de ofrecer una herramienta útil en el abordaje terapéutico en estos pacientes.
Material y métodos: Se revisaron artículos originales, ensayos clínicos y revisiones sistemáticas hasta septiembre de 2016, bases de datos internacionales de interacciones medicamentosas y Guías de Práctica Clínica actualizadas.
Desarrollo: Las terapias contra el virus de la Hepatitis C (VHC) han evolucionado vertiginosamente con el desarrollo de los antivirales de acción directa (AADs). Los nuevos regímenes han conseguido igualar las tasas de respuesta al tratamiento en los monoinfectados y los coinfectados con VIH, una población tradicionalmente difícil de tratar que, además, asociaba una elevada morbimortalidad hepática y sistémica, más reacciones adversas y complejas interacciones medicamentosas.
Conclusiones: En este nuevo escenario es fundamental dedicar esfuerzos a identificar el elevado porcentaje de infectados no diagnosticados, potenciales interacciones, especialmente con fármacos para patologías asociadas al envejecimiento de los pacientes, reacciones adversas a medio-largo plazos y desarrollo de resistencias, además de garantizar la cobertura universal en todos los contextos clínicos.
Palabras claves: Coinfección VIH/VHC, Tratamiento VIH/VHC, Hepatitis C, VIH, Antivirales de acción directa, AAD.
Introduction:Therapies for hepatitis C virus (HCV) have rapidly evolved with the development of direct-acting antiviral agents. New regimens, achieve an equate response rates to treatment in cases of HCV mono-infected and HIV/HCV co-infected; a population traditionally difficult to treat due to a high hepatic and systemic morbidity-mortality, adverse reactions and drug interactions.
Objective: To analyse the current Pharma-therapeutic options available for co-infected HIV-HCV patients, with emphasis I the new direct-acting antiviral agents, in order to offer a useful tool for the therapeutic approach in these patients.
Material and Methods: Original articles, clinical studies and systematic reviews until September 2016 were carried out, as well as international drug interactions databases and updated Practical Guidelines.
Development: Therapies for hepatitis C virus (HCV) have rapidly evolved with the development of direct-acting antiviral agents. New regimens achieve an equate response rates to treatment in HCV mono-infected and HIV/HCV co-infected; a population traditionally difficult to treat, which also associate a high hepatic and systemic morbidity-mortality, adverse reactions and complex drug interactions. ]]>
Conclusions: In this new scenario efforts must be addressed to identify the high percentage of undiagnosed patients; potential interactions, especially with drugs related with patient’s aging; medium and long-term adverse reactions and development of drug resistances, as well as to guarantee universal coverage in all clinical contexts.
Keywords: HIV/HCV coinfection, HIV/HCV treatment, Hepatitis C, HIV, Direct-acting antiviral agents, DAA.
INTRODUCCIÓN
Se estima que el virus de la inmunodeficiencia humana (VIH) afecta actualmente a 36,7 millones de personas1 y que 185 millones viven infectadas por el virus de la Hepatitis C (VHC).2, 3 Debido a que ambos virus comparten rutas similares de transmisión, de 10 a 30% de los infectados por VIH se encuentran coinfectados por el virus de la Hepatitis C. La coinfección cobra una gran relevancia clínica y farmacoterapéutica puesto que los pacientes coinfectados tienen, tradicionalmente, mayor riesgo de sufrir progresión acelerada de la enfermedad hepática, cirrosis, fallo hepático y hepatocarcinoma; además de presentar una menor efectividad de los tratamientos, mayor incidencia de reacciones adversas e interacciones farmacológicas, lo que dificulta el cumplimiento terapéutico.4-9 En el caso del virus de la Hepatitis C, con el desarrollo de los nuevos antivirales de acción directa (AAD), en los últimos meses el escenario clínico-terapéutico en esta enfermedad ha cambiado vertiginosamente,3, 6, 7 y se ha alcanzado la eliminación del virus en porcentajes cercanos a 100%. Por su parte, también se ha avanzado en las últimas décadas en las terapias anti-VIH, convertido el SIDA en una enfermedad crónica. Con fármacos menos hepatotóxicos, hoy está indicado tratar precozmente a todos los pacientes independientemente de la cifra de linfocitos CD4.10
OBJETIVO
El objetivo de esta revisión es analizar los paradigmas preexistentes, reevaluar los dogmas de la evidencia científica disponible y actualizarla a este nuevo escenario clínico y social para este grupo de pacientes.
]]>MATERIAL Y MÉTODOS
Se realizaron búsquedas sistemáticas en la base de datos MEDLINE de información biomédica a través del motor PubMed. Se incluyeron en la selección clínicos ensayos, resultados de investigaciones originales y revisiones sistemáticas hasta septiembre de 2016. Se utilizó, además, la biblioteca médica UpToDate ® para acceder a las Guías de Práctica Clínica en el contexto de coinfección por VIH/VHC; así como las Guías AEEH/SEIMC de manejo de la Hepatitis C (Asociación Española para el estudio del Hígado y Sociedad Española de Enfermedades Infecciosas y Microbiología Clínica) y las Guías de Hepatitis C de la American Association for the Study of Liver Diseases, ambas con actualización de julio de 2016. En materia de interacciones medicamentosas se accedió a las bases de datos de la Universidad de Liverpool mediante la plataforma www.hep-druginteractions.org, con última actualización de evidencia científica el 26 de noviembre de 2015.
DESARROLLO
VHC y VIH: mecanismos de interacción y comorbilidad
Progresión del VIH en el contexto de coinfección VHC
Hoy todavía está en entredicho el papel que tiene el VHC en la progresión del VIH y la mayoría de estudios no ha demostrado relevancia clínica.3,5,11-13 Se postula que la activación continua de los linfocitos T podría limitar la respuesta inmunológica. Además, la infección extrahepática de los linfocitos CD4 por el VHC podría derivar en interacciones virológicas directas que influyeran en la recuperación de los CD4. Las proteínas NS3/NS4A del virus C promueven la transcripción del VIH, mientras que la del Core activa la replicación.14,15
Progresión del VHC en el contexto de coinfección VIH
El VIH tiene un importante impacto en el ciclo del virus C y en su historia natural. Los coinfectados tienen menor tasa de eliminación del VHC y progresión acelerada hacia enfermedad hepática sintomática, terminal, cirrosis y carcinoma hepatocelular.3, 16, 17 Los mecanismos etiopatogénicos implicados se detallan en la Tabla1.
]]> La primera causa de muerte en los pacientes coinfectados tratados con terapia antirretroviral era la enfermedad hepática terminal.3 Este incremento se debe, en parte, al aumento de la esperanza de vida y al descenso de la mortalidad asociada a las complicaciones del SIDA en pacientes tratados.10 Sin embargo, según la evidencia más actual, con los nuevos regímenes de tratamiento con AAD se podría llegar a igualar la progresión de la fibrosis en ambas subpoblaciones.10 Por otra parte, también es necesario recalcar el mayor número observado de reinfecciones por VHC en los individuos coinfectados, debido, posiblemente, a la permanencia de los factores de riesgo.Otras complicaciones de la coinfección
Con la disminución de la mortalidad por SIDA y el envejecimiento de los pacientes, la inflamación crónica se asociaba a mayor riesgo de morbimortalidad cardiovascular debido a la disfunción endotelial.18 Además, en individuos con una larga historia de seropositividad VIH, se observa un incremento significativo del riesgo relativo de enfermedad renal por VIH.19 Por otro lado, la coinfección aumenta la incidencia de neuropatía motora periférica, daño cognitivo y empeoramiento de la demencia asociada a VIH5,9 y asocia mayor riesgo de Diabetes Mellitus independientemente del daño hepático.3,20 En los últimos años se ha definido que tanto el riesgo de fracturas como de osteoporosis se encuentran significativamente elevados.21
Propósitos de la terapia
La curación del VHC se asume en base a la respuesta virológica sostenida (RVS), que asocia a reducciones sustanciales de la morbimortalidad hepática: se frena, enlentece o mejora la progresión de la fibrosis y la necroinflamación y disminuye la tasa de carcinoma hepatocelular, además de desaparecer los efectos adversos de la pluriterapia y las interacciones farmacológicas.22 Con los nuevos AAD, se considera RVS una carga viral indetectable 12 semanas tras el tratamiento. La RVS4, sin ser un parámetro definitorio de curación, se considera buen factor de predicción.23-25
Opciones terapéuticas contra el VHC en el contexto particular de la coinfección VIH/VHC
Con los AAD no parecen existir diferencias en tasas de curación y tolerabilidad entre pacientes mono y coinfectados, al contrario de lo que ocurría con la biterapia clásica y la triple terapia de primera generación. De tal manera, el tratamiento antiviral de la Hepatitis C tiene, en las últimas guías, las mismas indicaciones y regímenes que en monoinfectados.6,7,10,23 Para el desarrollo de estos fármacos ha sido fundamental el conocimiento del ciclo viral3 y sus dianas terapéuticas se detallan en la Tabla2. La coinfección VIH/VHC proporciona mayor prioridad en cuanto al tratamiento del VHC incluso en estadios tempranos de fibrosis (F0/F1) y se aboga por un tratamiento precoz.7 La elección del régimen terapéutico depende del genotipo, el estadio de lafibrosis hepática, la historia de previo tratamiento o la elegibilidad de regímenes con interferón en algunos casos. Sin embargo, en los pacientes coinfectados, las interacciones medicamentosas suponen una limitación al tratamiento que no debe ser obviada.3,9,25
Interacciones farmacológicas
La necesidad de pluriterapia para evitar resistencias aumenta la posibilidad de interacciones que alteren el equilibrio riesgo/beneficio entre los efectos adversos del tratamiento y su efectividad terapéutica, amén de la crucial cumplimentación. Por ello, encontrar una pauta individualizada carente de interacciones que repercutan negativamente sobre el cursusmorbi y sobre sí mismos supone todo un reto en la práctica clínica.7,9
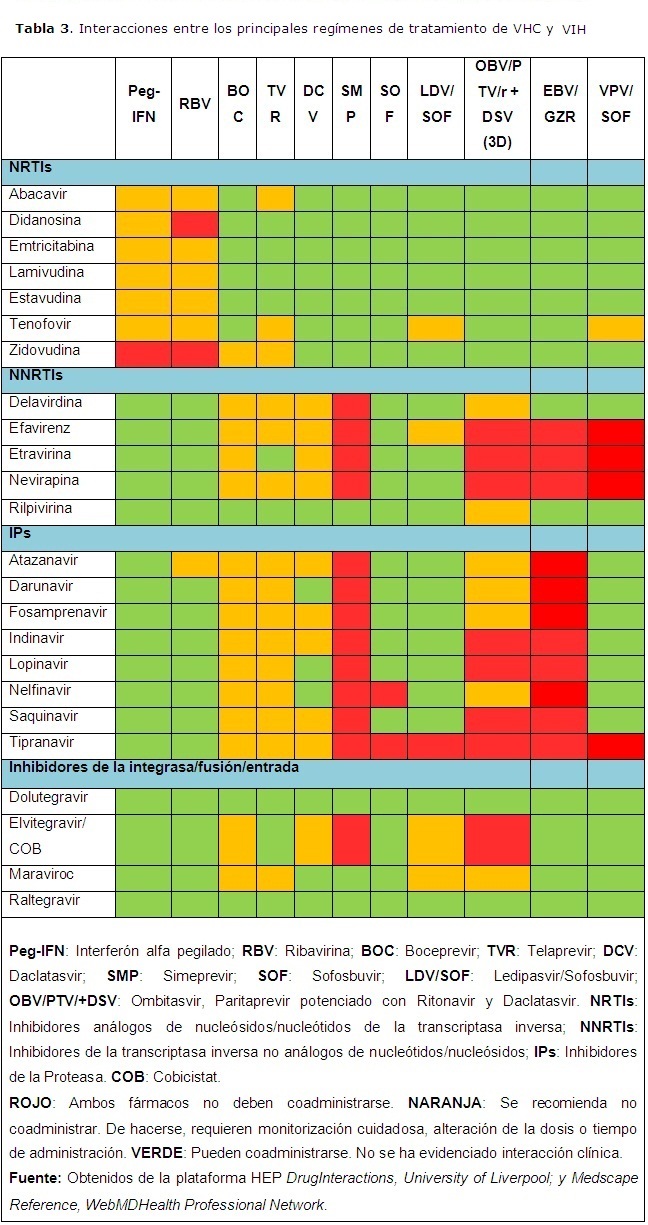
]]> Interacciones con los nuevos AADMuchos son sustratos del CYP3A4 o de la p-gp, lo que puede contraindicar su coadministración con inhibidores no nucleósidos de la transcriptasa inversa (NNRTIs) o inhibidores de la proteasa (IPs). Las contraindicaciones con inhibidores de la integrasa son escasas. La relevancia clínica se encuentra gradada en la Tabla3.
a. Sofosbuvir: Una de las grandes ventajas de este fármaco es la ausencia de interacciones farmacológicas clínicamente significativas con los antirretrovirales y su efecto pan-genotípico.26 No se aconseja la coadministración con Tipranavir, puesto que se postula que este podría disminuir su eficacia e inducir la glicoproteína P.27
b. Daclatasvir: No ha mostrado interacción alguna con los inhibidores nucleósidos de la transcriptasa inversa (NRTIs). En el grupo de los NNRTIs solo se ha demostrado su interacción con el Efavirenz, que obliga a aumentar la dosis del primero. Se estima que la inhibición del CYP3A4 por la Nevirapina, la Etravirina y la Delavirdina; y por Tipranavir, Saquinavir, Indinavir, Ritonavir, Fosamprenavir y Cobicistat pueda incrementar sus concentraciones. Debe reducirse su dosis a la mitad en cotratamiento con Atazanavir/Ritonavir.27
c. Simeprevir: No se esperan interacciones farmacológicas clínicamente significativas con la coadministración de Simeprevir con los NRTIs. Al ser sustrato del CYP3A4 está contraindicado con todos los IPs. Tampoco se recomienda la administración conjunta de Delavirdina, Efavirenz, Etravirina y Nevirapina, siendo la Rilpivirina el único NNRTI que no asocia ninguna interacción significativa.27
d. Ledipasvir (Ledipasvir/Sofosbuvir): El Ledipasvir se asocia en la práctica clínica al Sofosbuvir por lo que no se recomienda la coadministración con Tipranavir. No tiene interacción con ningún otro IP del VIH. Respecto a los NRTIs, la coadministración con Tenofovir incrementa la exposición de este fármaco, especialmente si se asocia a Elvitegravir, Cobicistat o Emtricitabina, y hace recomendable la monitorización cuidadosa de la función renal. En el grupo de NNRTIs, se estudió la interacción farmacológica en pacientes tratados con los regímenes Ledipasvir/Sofosbuvir y Tenofovir/Emtricitabina/Efavirenz. En este grupo se incrementó el AUC del Tenofovir 98% y disminuyó la del Ledipasvir 34%. No se recomienda ajuste de dosis, pero sí monitorizar la función renal por el riesgo de toxicidad del Tenofovir.28
e. Combinación de Ombitasvir/Paritaprevir potenciado con Ritonavir y Ombitasvir/Paritaprevir/r y Dasabuvir (régimen 3D): No existen interacciones clínicamente significativas con los NRTIs, pero sí con los NNRTIs debido, mayormente, al efecto sobre el citocromo p450 del Ritonavir. Está contraindicado administrarse con Efavirenz, Etravirina o Nevirapina. La Rilpivirina puede coadministrarse pero tiene interacciones potenciales. También con los IP. Se contraindica su coadministración con Indinavir, Lopinavir y Saquinavir por su inhibición del CYP3A4. La coadministración de este régimen con Atazanavir, Darunavir, Fosamprenavir y Nelfinavir no se recomienda, pero en caso de utilizarse debe ser monitorizada cuidadosamente, alterar las dosis o el tiempo de administración. No se observan interacciones significativas con el Raltegravir o el Dolutegravir. Elvitegravir se combina con Cobicistat, que podría incrementar su concentración por inhibición del CYP3A4.27,29
f. Grazoprevir/Elbasvir: Ambos son sustratos del CY3A4 y la p-gp. El Grazoprevir también lo es de OATP1B1. Por ello, no pueden ser administrados con los inhibidores de la proteasa o con NNRTIs inductores del citocromo como el Efavirenz, la Etravirina o la Nevirapina. No existe interacción con los NRTIs o inhibidores de la integrasa.23,27
g. Velpatasvir (Velpatasvir/Sofosbuvir): El Velpatasvir se metaboliza por el CYP3A4 y es sustrato de la p-gp, pero solo se ha evidenciado interacción con el Tipranavir, Efavirenz, Etravirina y Nevirapina. La función renal debe vigilarse, especialmente en combinación con Tenofovir. No interaccionan con los inhibidores de la integrasa y con el resto de ARV.23,27
Efecto del VIH en la respuesta al tratamiento del VHC y hepatotoxicidad de los antirretrovirales
]]> Los pacientes coinfectados respondían peor a la biterapia: la RVS en el genotipo 1 del VHC descendía para situarse en rangos variables desde 14 a 35%, en comparación con 42 a 46% de los monoinfectados.30Uno de los principales problemas lo constituye la hepatotoxicidad del tratamiento antirretroviral, cuya incidencia es heterogénea (3-18%),31 debido a la variabilidad en sus manifestaciones. Las más graves son más frecuentes en pacientes infectados por VHB o VHC, particularmente en el GT3 del VHC, que no asocia respuestas terapéuticas tan elevadas como otros genotipos del virus.25,32 Son factores de riesgo el grado de fibrosis previa, GT3, el sexo femenino, duración elevada del tratamiento antirretroviral, alcohol y tratamiento con nevirapina o con IPs.32 Los mecanismos son variables. Por un lado, se ha demostrado que las interacciones mediadas por el CYP3A4 comentadas en el punto anterior son causa de hepatotoxicidad, generalmente debida a acumulación de NNRTIs e IPs o sus metabolitos y generación de especies reactivas del oxígeno.31,32 La Didanosina o la Estavudina pueden inhibir la DNA polimerasa gamma, que resulta en acumulación de ácidos grasos libres y esteatosis hepática y causar toxicidad mitocondrial que puede llevar a fallo hepático agudo. Otro factor a considerar son las alteraciones metabólicas; la resistencia a la insulina y la esteatohepatitis podrían incrementar el riesgo.
La heterogeneidad de las series y la combinación farmacológica dificultan la determinación precisa de esta hepatotoxicidad. Dentro de los IPs, el Ritonavir a dosis completa parece ser el más tóxico, junto con el Indinavir y el Saquinavir.32 En un estudio con 1 052 pacientes que comparó Ritonavir, Indinavir, Amprenavir, Saquinavir y Nelfinavir se observó que este último era el menos perjudicial.33 El Lopinavir y el Atazanavir potenciados con dosis bajas de Ritonavir también tienen buenos perfiles de seguridad. Otro estudio observacional concluyó que un cambio a Raltegravir y la Rilpivirina frente a Efavirenz mejora la hepatotoxicidad asociada, con un mismo perfil de efectividad.34
Régimen actual de tratamiento del VHC en pacientes coinfectados
Los regímenes libres de interferón basados en AAD deben ser considerados como tratamiento estándar para infección crónica por VHC tanto en el contexto de la mono como la coinfección VIH, y los regímenes con interferón solamente se recomiendan en infecciones por el genotipo 3 que no hayan respondido a previo tratamiento con Sofosbuvir + Daclatasvir o Sofosbuvir/Velpatasvir.23,24
El tratamiento y su duración dependen del genotipo viral, de la presencia de cirrosis compensada o descompensada y el previo tratamiento con AADs. Los regímenes terapéuticos libres de IFN para pacientes naïve a AADs y las opciones con IFN se definen en las tablas 4 y 5, respectivamente.
Evidencia clínica de las combinaciones en coinfectados VIH/VHC
Regímenes sin interferón
a. Simeprevir y Sofosbuvir: Un estudio con 50 pacientes coinfectados con marcadores negativos de respuesta encontró una RVS24 de 82% asociando Ribavirina.35 El estudio COSMOS randomizado que evaluó la eficacia y la seguridad de esta combinación en 167 pacientes, sin embargo, no evaluó los coinfectados por VIH.36-38
b. Sofosbuvir y Ledipasvir: Un ensayo de fase 2b en 50 pacientes no tratados, sin cirrosis, infectados por el GT1, demostró una RVS de 98% a 12 semanas.28 El ensayo NAIAD ERADICATE estudió 50 pacientes naïve divididos en dos grupos: uno, con tratamiento ARV con Tenofovir/Emtricitabina asociados a Efavirenz, Rilpivirina o Raltegravir y otro ARV naïve, con mayoría (74%) de infectados por el GT1b. Las RVS fueron 98% y 100%, respectivamente, a 12 semanas.39 El ION 4 siguió a 355 pacientes con esta combinación con GT 1 y 4 y 12 semanas de esta combinación. Globalmente, 96% alcanzó la RVS12, 96% en los genotipos 1a y 1b y 100% en el GT4, y no fue significativa la presencia de cirrosis o previo tratamiento.40 La German Hepatitis C Cohort (GECCO) evaluó la respuesta en coinfectados tratados con Ledipasvir-Sofosbuvir durante 8 semanas. De 148 pacientes, 28 tenían coinfección VIH/VHC y estaban infectados por el GT1 del VHC. En este grupo, la respuesta viral en la semana 4 y la RVS12 fue de 100%. Los efectos adversos relacionados con el tratamiento fueron leves y poco frecuentes.41 En ningún caso hubo discontinuaciones por efectos adversos.
]]> c. Daclatasvir y Sofosbuvir: Un estudio con 151 pacientes naïve y 52 tratados, con GT del 1 al 4 (GT1 83%) demostró unas RVS12 de 96, 4% 97,7% respectivamente, en el GT1. La RVS global fue de 97% y la cirrosis no fue un factor determinante. No hubo discontinuaciones por reacciones adversas.42 Cabe mencionar que en pacientes monoinfectados, sí existe respuesta subóptima en pacientes cirróticos, por lo que podría considerarse extrapolable a los coinfectados.43d. Ombitasvir, Paritaprevir/r y Dasabuvir asociados a Ribavirina, o régimen 3D: El estudio TURQUOISE-I parte 1a analizó esta combinación en 63 pacientes coinfectados, con el GT1, naïve o con fallo terapéutico con biterapia, incluyendo pacientes con cirrosis. Las RVS12 y RVS24 fueron de 94% y 91%, respectivamente, sin que hubiera discontinuaciones por efectos adversos.44 Según resultados preliminares, la parte 1b del estudio evaluó un total de 22 pacientes divididos en dos brazos, según toma única diaria o dividida en dos dosis. La respuesta viral en la semana 4 y la RVS12 fue de 100%. No hubo efectos adversos graves relacionados con fármacos ni alteraciones clínico-analíticas relacionadas con el Darunavir. La parte 2 del estudio continúa evaluando el régimen 3D en coinfectados, con el GT1 y el GT4 en un ensayo multicéntrico global con 230 pacientes.44
e. Sofosbuvir y Ribavirina: El estudio PHOTON-245 analizó esta combinación en 274 pacientes de los genotipos 1, 2, 3 y 4; durante 12 semanas en los pacientes naïve infectados por el GT2 y durante 24 en el resto. Las RVS12 globales fueron de 85% en el GT1, 88% en el GT2, 89% en el GT3 y 84% en el GT4. Las respuestas en pacientes naïve con GT 2 y 3 comparadas con las de aquellos que habían recibido tratamiento fueron similares (89% y 91% vs 83% y 86%, respectivamente. Seis pacientes discontinuaron el tratamiento por efectos adversos.
f. Grazoprevir/Elbasvir: El estudio C-WORTHY, un ensayo clínico multicéntrico, aleatorizado y controlado de fase 2, evaluó la eficacia y la seguridad del Grazoprevir y dos dosis de Elbasvir, asociado o no a Ribavirina, en pacientes monoinfectados por el VHC y en coinfectados naïve VIH/VHC con GT1 durante 12 semanas. De los 218 pacientes del estudio, 59 eran coinfectados. La RVS12 en este grupo fue de 87% sin Ribavirina y de 97% con Ribavirina, frente a 98% y 93%, respectivamente, en el grupo de los monoinfectados. El perfil de seguridad fue similar en ambos grupos y ningún paciente discontinuó debido a efectos adversos o anormalidad analítica.46 Por otra parte, el estudio C-EDGE CO-INFECTION, un ensayo de fase 3 multicéntrico, estudió, particularmente en un grupo de 218 pacientes coinfectados VIH/VHC con los genotipos 1, 4 y 6, y entre los que se incluían tanto cirróticos como pacientes sin cirrosis, la eficacia, la seguridad y la tolerabilidad del régimen Grazoprevir + Elbasvir durante 12 semanas. Si bien no es un ensayo aleatorizado y controlado, se consiguió la RVS12 en 96% de los pacientes, de los cuales uno no la alcanzó por motivo no virológico. Las reacciones adversas fueron leves y poco frecuentes, y todos completaron el estudio.47
g. Velpatasvir/Sofosbuvir: Todavía no existe evidencia publicada en coinfectados. Está en marcha un estudio de fase 3, el ASTRAL-5, con 106 pacientes coinfectados con Gt1-4, de los cuales 18% tiene cirrosis compensada. Los resultados preliminares informan una RVS12 de 95%.48 Los estudios ASTRAL de fase 3 (ASTRAL-1, ASTRAL-2, ASTRAL-3 y ASTRAL-4) han estudiado un total de 1 302 pacientes monoinfectados bajo este régimen durante 12 semanas–24 semanas en cirrosis descompensada- y, salvo en este caso, en el que las RVS fueron de 83-86%, en todos los genotipos se alcanzó RVS>95%, incluido el GT3.49-51
Las reacciones adversas con los nuevos AAD son menores, leves, principalmente comunes a todos ellos e inespecíficas. Las más frecuentes incluyen fatiga (en torno a 20% de los pacientes, salvo en el régimen 3D, que asciende a 48%), cefalea (16-25%),38-40,42,43,46 náusea (15-18%)28,38,43,46,47 y diarrea en algunos casos (10-11%).39, 40 Otros efectos menores son la congestión nasal y la mialgia con el Ledipasvir (16% y 14% respectivamente),28 o insomnio en el régimen 3D (19%).36 Ninguno repercute en el seguimiento. Si se administran con Ribavirina, esta superpone sus efectos secundarios, si bien su tolerancia sigue siendo mejor que la del IFN.
Regímenes con interferón
a. pegIFN - Ribavirina más Rimeprevir: En un estudio, 106 pacientes recibieron Simeprevir asociado a la biterapia clásica. No cirróticos naïve y recaedores previos lo recibieron guiado por la respuesta durante 24-48 semanas, y los cirróticos, los no respondedores y los respondedores parciales durante 48 semanas. Las tasas de SVR12 fueron 79.2% en los pacientes naïve, 57,1% en los no respondedores, 86,7% en los recaedores y de 70% en los respondedores parciales. Las reacciones adversas, ocurridas en 5,7% de los pacientes, ninguna fatal, fueron las atribuibles a la biterapia.52
b. PegIFN – Ribavirina más Telaprevir o Boceprevir: Un ensayo de fase 2 en 69 pacientes infectados –excluyendo cirróticos y no respondedores- por el genotipo 1 y con tratamiento antirretroviral con Tenofovir, Emtricitabina, Efavirenz, Atazanavir, y Raltegravir como ARV permitidos recibió biterapia asociada a Telaprevir,y se obtuvo una RVS24 de 80%. Sin embargo, 20% de los pacientes discontinuó el tratamiento por efectos adversos, y dos pacientes murieron durante el estudio. No hubo alteración en el control del VIH.53 Otro estudio se dedicó a estudiar las diferencias en la tasa de respuesta de 134 pacientes coinfectados por VIH tratados con biterapia frente a la asociación de esta con inhibidores de la proteasa durante 48 semanas –triple terapia durante 8 semanas y biterapia hasta finalizar las 48–. En el genotipo 1 se obtuvo una tasa de RVS de 50% (frente a 33,3% de la biterapia).
Nuevos tratamientos contra el virus C en pacientes coinfectados
]]> Algunos autores cuestionan la necesidad de nuevos fármacos contra el VHC.6 Se afirma que en una situación en la que se consiguen tasas de RVS de más de 90% con los nuevos regímenes disponibles, la investigación tanto farmacológica como clínica debe centrarse en las áreas que quedan sin resolver, a saber: RVS subóptimas; cirrosis compensada y descompensada; cargas virales asociadas a peor pronóstico (>6000000 copias/mL), así como abogar por una cobertura mayor en los sistemas de salud que persiga la universalidad en el acceso al tratamiento en los pacientes con VHC. Además, con los nuevos ensayos clínicos y las precoces RVS, se están evaluando pautas más cortas de tratamiento con resultados variables7,43 que todavía deben ser evaluados.Pese a la diversidad de posturas, emergen AAD de segunda generación, haciendo que las guías terapéuticas y las recomendaciones clínicas cambien rápidamente.54 Los nuevos inhibidores de la NS3/4A (como el Sovaprevir, ABT-493 o GS-9857) y NS5A (Samatasvir, GS-5816, MK-8408 o ABT-530) presentarán una mejor barrera de resistencia y efecto pangenotípico. Además, eludirán el problema de las variantes asociadas a resistencia (RAV), como ya se ha demostrado con el ABT-530 o el ABT-493. Se prevé incluso que se acorte la duración del tratamiento.
CONCLUSIONES
La coinfección VIH/VHC ha sufrido una revolución que ha sacudido los paradigmas previos y acerca la erradicación del VHC. Para conseguirlo cabrá además atajar el problema del elevado porcentaje de infectados no diagnosticados. Con los AAD se ha salvado la brecha que les separaba de los pacientes monoinfectados y les condenaba a menores tasas de respuesta terapéutica, las interacciones y la toxicidad farmacológica que ponía en riesgo la cumplimentación, y a una mayor morbimortalidad hepática. Con esta nueva etapa se abren nuevos retos: debido al aluvión de nuevas moléculas debemos estar alerta ante potenciales interacciones farmacológicas, especialmente con fármacos asociados a patologías prevalentes asociadas al envejecimiento, reacciones adversas a medio-largo plazos, amén de la aparición de resistencias. Finalmente, es imprescindible dedicar esfuerzos a los grupos de respuesta subóptima, a aumentar la detección de casos sin diagnosticar, sobre todo, en las poblaciones ocultas, y a garantizar la transparencia y la cobertura universal en todos los contextos clínicos.
REFERENCIAS BIBLIOGRÁFICAS
1. Global AIDS Update 2016. UNAIDS Report. Joint United Nations Programme on HIV/AIDS. [Internet]. Who.int. 2016. Consultado: 13 de diciembre 2016. Disponible en: http://www.who.int/hiv/pub/arv/global-AIDS-update-2016_en.pdf?ua=1
2. Messina J, Humphreys I, Flaxman A, Brown A, Cooke G, Pybus O, et al. Global distribution and prevalence of hepatitis C virus genotypes. Hepatology. 2014;61(1):77-87.
3. Kang W, Tong H, Sun Y, Lu Y. Hepatitis C virus infection in patients with HIV-1: epidemiology, natural history and management. Expert Rev Gastroenterol Hepatol. 2014;8(3):247-266.
4. Kaźmierczak J, Pawełczyk A, Cortes K, Radkowski M. Seronegative Hepatitis C Virus Infection. Arch Immunol Ther Exp. 2013;62(2):145-151.
5. Operskalski EKovacs A. HIV/HCV Co-infection: Pathogenesis, Clinical Complications, Treatment, and New Therapeutic Technologies. Curr HIV/AIDS Rep. 2011;8(1):12-22.
]]>6. Petta SCraxì A. Current and future HCV therapy: do we still need other anti-HCV drugs? Liver Int. 2014;35:4-10.
7. Sulkowski M. HCV-HIV co-infected patients: no longer a ‘special’ population? Liver Int. 2016;36:43-46.
8. Wyles D. Regimens for Patients Coinfected with Human Immunodeficiency Virus. Clin Liver Dis. 2015;19(4):689-706.
9. Silverstein P, Kumar S, Kumar A. HIV-1, HCV and Alcohol in the CNS: Potential Interactions and Effects on Neuroinflammation. Curr HIV Res. 2014;12(4):282-292.
10. Arends J, Lieveld F, Boeijen L, de Kanter C, van Erpecum K, Salmon D et al. Natural history and treatment of HCV/HIV coinfection: Is it time to change paradigms? J Hepatol. 2015;63(5):1254-1262.
11. Sullivan P, Hanson D, Teshale E, Wotring L, Brooks J. Effect of hepatitis C infection on progression of HIV disease and early response to initial antiretroviral therapy. AIDS. 2006;20(8):1171-1179.
12. Chen T, Ding E, Seage III G, Kim A. Meta‐Analysis: Increased Mortality Associated with Hepatitis C in HIV‐Infected Persons Is Unrelated to HIV Disease Progression. Clin Infect Dis. 2009;49(10):1605-1615.
]]>13. Liberto M, Zicca E, Pavia G, Quirino A, Marascio N, Torti C, et al. Virological Mechanisms in the Coinfection between HIV and HCV. Mediators of Inflammation. 2015;2015:1-7.
14. Kang L, Luo Z, Li Y, Zhang W, Sun W, Li W, et al. Association of Vpu with hepatitis C virus NS3/4A stimulates transcription of type 1 human immunodeficiency virus. Virus Research. 2012;163(1):74-81.
15. Swaminathan G, Pascual D, Rival G, Perales-Linares R, Martín-García J, Navas-Martín S. Hepatitis C virus core protein enhances HIV-1 replication in human macrophages through TLR2, JNK, and MEK1/2-dependent upregulation of TNF-α and IL-6. FEBS Letters. 2014;588(18):3501-3510.
]]>
16. Merchante N, Merino E, López-Aldeguer J, Jover F, Delgado-Fernández M, Galindo M, et al. Increasing Incidence of Hepatocellular Carcinoma in HIV-Infected Patients in Spain. Clin Infect Dis. 2012;56(1):143-150.
17. Limketkai B, Mehta S, Sutcliffe C, Higgins Y, Torbenson M, Brinkley S, et al. Relationship of Liver Disease Stage and Antiviral Therapy With Liver-Related Events and Death in Adults Coinfected With HIV/HCV. JAMA. 2012;308(4).
18. De Castro I, Micheloud D, Berenguer J, Guzmán-Fulgencio M, Catalán P, Miralles P, et al. Hepatitis C virus infection is associated with endothelial dysfunction in HIV/hepatitis C virus coinfected patients. AIDS. 2010;24(13):2059-2067.
19. Wyatt C, Malvestutto C, Coca S, Klotman P, Parikh C. The impact of hepatitis C virus coinfection on HIV-related kidney disease: a systematic review and meta-analysis. AIDS. 2008;22(14):1799-1807.
20. Marks K, Kitch D, Chung R, Hadigan C, Andersen J, Tien P, et al. Pilot Study of Pioglitazone Before HCV Retreatment in HIV/HCV Genotype 1–Infected Subjects With Insulin Resistance and Previous Nonresponse to Peginterferon and Ribavirin Therapy. J Acquir Immune Defic Syndr. 2014;65(3):345-349.
21. Dong H, Cortés Y, Shiau S, Yin M. Osteoporosis and fractures in HIV/hepatitis C virus coinfection. AIDS. 2014;28(14):2119-2131.
22. Mira J, Rivero-Juárez A, López-Cortés L, Girón-González J, Téllez F, Santos-Gil I, et al. Benefits From Sustained Virologic Response to Pegylated Interferon Plus Ribavirin in HIV/Hepatitis C Virus-Coinfected Patients With Compensated Cirrhosis. Clin Infect Dis. 2013;56(11):1646-1653.
]]>23. AASLD-IDSA. HCV Guidance: Recommendations for Testing, Managing, and Treating Hepatitis C. February 2016. [Internet];. Consultado: 13 diciembre 2016. [Internet]. Consultado: 13 diciembre 2016. Disponible en: http://hcvguidelines.org/sites/default/files/HCV-guidance_February_2016_a1.pdfGuidance_February_2016_a1.pdf
24. Sociedad Española de Enfermedades Infecciosas y Microbiología Clínica. Asociación Española para el estudio del Hígado. Guías AEEH/SEIMC de manejo de la Hepatitis C. Julio 2016 [Internet]. Consultado: 13 diciembre 2016. Disponible en: https://www.seimc.org/contenidos/documentoscientificos/guiasclinicas/seimc-clinicasclinicas-2016-Manejo_HepatitisC.pdf
25. Webster D, Klenerman P, Dusheiko G. Hepatitis C. Lancet. 2015;385 (9973):1124-1135.
26. Naggie SKim A. PHOTON-2: hope for patients with HIV and HCV co-infection? Lancet. 2015;385(9973):1052-1054.
]]>27. University of Liverpool. Hep-Drug Interactions, [Internet]. Disponible en: http://www.hep-druginteractions.org
28. Osinusi A, Townsend K, Kohli A, Nelson A, Seamon C, Meissner E, et al. Virologic Response Following Combined Ledipasvir and Sofosbuvir Administration in Patients With HCV Genotype 1 and HIV Co-infection. JAMA. 2015;313(12):1232.
29. Nelson D, Cooper J, Lalezari J, Lawitz E, Pockros P, Gitlin N, et al. All-oral 12-week treatment with daclatasvir plus sofosbuvir in patients with hepatitis C virus genotype 3 infection: ALLY-3 phase III study. Hepatology. 2015;61(4):1127-1135.
30. Torriani F, Rodríguez-Torres M, Rockstroh J, Lissen E, González-García J, Lazzarin A, et al. Peginterferon Alfa-2a plus Ribavirin for Chronic Hepatitis C Virus Infection in HIV-Infected Patients. N Engl J Med. 2004;351(5):438-450.
31. Núñez M. Clinical syndromes and consequences of antiretroviral-related hepatotoxicity. Hepatology. 2010;52(3):1143-1155.
32. Surgers Lacombe K. Hepatoxicity of new antiretrovirals: A systematic review. Clin Res Hepatol Gastroenterol. 2013;37(2):126-133.
33. Rodríguez-Rosado R, García-Samaniego J, Soriano V. Hepatotoxicity after introduction of highly active antiretroviral therapy. AIDS. 1998;12(10):1256.
]]>34. Cevik M, Katsarolis I, Singh G, Nelson M. A switch to Raltegravir improves antiretroviral associated hepatotoxicity in individuals co-infected with HIV and hepatitis C. J Infect. 2014;69(2):190-193.
35. Basu P, Shah N, Brown R. P0819: Simeprevir and sofosbuvir with modified doses of ribavirin (RBV) therapy on telaprevir experienced co infected (with HIV) cirrhotics with chronic hepatitis C (CHC). A randomized open label clinical pilot study: Stop C. J Hepatol. 2015;62:S643.
36. Lawitz E, Sulkowski M, Ghalib R, Rodríguez-Torres M, Younossi Z, Corregidor A, et al. Simeprevir plus sofosbuvir, with or without ribavirin, to treat chronic infection with hepatitis C virus genotype 1 in non-responders to pegylated interferon and ribavirin and treatment-naive patients: the COSMOS randomised study. Lancet. 2014;384(9956):1756-1765.
]]>
37. Sulkowski MBenhamou Y. Therapeutic issues in HIV/HCV-coinfected patients. J Viral Hepat. 2007;14(6):371-386.
38. Sulkowski M, Eron J, Wyles D, Trinh R, Lalezari J, Wang C, et al. Ombitasvir, Paritaprevir Co-dosed With Ritonavir, Dasabuvir and Ribavirin for Hepatitis C in Patients Co-infected With HIV-1. JAMA. 2015;313(12):1223.
39. Kumari R, Nguyen M. Fixed-dose combination of sofosbuvir and ledipasvir for the treatment of chronic hepatitis C genotype 1. Expert Opin Pharmacother. 2015;16(5):739-748.
40. Naggie S, Cooper C, Saag M, Workowski K, Ruane P, Towner W, et al. Ledipasvir and Sofosbuvir for HCV in Patients Co-infected with HIV-1. N Engl J Med. 2015;373(8):705-713.
41. Ingiliz P. Sofosbuvir Plus Ledipasvir for 8 Weeks in HCV-mono- and HIV-HCV-co-infected Patients. Results from the German Hepatitis C Cohort (GECCO). 15th European AIDS Conference. Oct 23, 2015.
42. Wyles D, Ruane P, Sulkowski M, Dieterich D, Luetkemeyer A, Morgan T et al. Daclatasvir plus Sofosbuvir for HCV in Patients Co-infected with HIV-1. N Engl J Med.2015;373(8):714-725.
43. Nelson D, Cooper J, Lalezari J, Lawitz E, Pockros P, Gitlin N, et al. All-oral 12-week treatment with daclatasvir plus sofosbuvir in patients with hepatitis C virus genotype 3 infection: ALLY-3 phase III study. Hepatology. 2015;61(4):1127-1135.
]]>44. Trinh R. TURQUOISE-I Study: Use of Ombitasvir/Paritaprevir/Ritonavir + Dasabuvir + Ribavirin in Patients with HCV/HIV-1 Co-infection on Stable Darunavir-containing Antiretroviral Therapy. 15th European AIDS Conference. Oct 23, 2015.
45. Molina J, Orkin C, Iser D, Zamora F, Nelson M, Stephan C, et al. Sofosbuvir plus Ribavirin for treatment of hepatitis C virus in patients co-infected with HIV (PHOTON-2): a multicentre, open-label, non-randomised, phase 3 study. Lancet. 2015;385(9973):1098-1106.
46. Sulkowski M, Hezode C, Gerstoft J, Vierling J, Mallolas J, Pol S, et al. Efficacy and safety of 8 weeks versus 12 weeks of treatment with Grazoprevir (MK-5172) and Elbasvir (MK-8742) with or without ribavirin in patients with hepatitis C virus genotype 1 mono-infection and HIV/hepatitis C virus co-infection (C-WORTHY): a randomised, open-label phase 2 trial. Lancet. 2015;385(9973):1087-1097.
]]>
47. Rockstroh J, Nelson M, Katlama C, Lalezari J, Mallolas J, Bloch M, et al. Efficacy and safety of grazoprevir (MK-5172) and elbasvir (MK-8742) in patients with hepatitis C virus and HIV co-infection (C-EDGE CO-INFECTION): a non-randomised, open-label trial. Lancet HIV. 2015;2(8):e319-e327.
48. Wyles D, Brau N, Kottilil S, Daar E, Workowski K, Luetkemeyer A, et al. Sofosbuvir/Velpatasvir Fixed Dose Combination for 12 Weeks in Patients Co-Infected with HCV and HIV-1: The Phase 3 Astral-5 Study. April 2016. Barcelona. España.
49. Feld J, Jacobson I, Hézode C, Asselah T, Ruane P, Gruener N, et al. Sofosbuvir and Velpatasvir for HCV Genotype 1, 2, 4, 5, and 6 Infection. N Engl J Med. 2015;373(27):2599-2607.
50. Foster G, Afdhal N, Roberts S, Bräu N, Gane E, Pianko S, et al. Sofosbuvir and Velpatasvir for HCV Genotype 2 and 3 Infection. N Engl J Med. 2015;373(27):2608-2617.
]]>51. Curry M, O’Leary J, Bzowej N, Muir A, Korenblat K, Fenkel J et al. Sofosbuvir and Velpatasvir for HCV in Patients with Decompensated Cirrhosis. N Engl J Med. 2015;373(27):2618-2628.
52. Dieterich D, Rockstroh J, Orkin C, Gutiérrez F, Klein M, Reynes J, et al. Simeprevir (TMC435) With Pegylated Interferon/Ribavirin in Patients Coinfected With HCV Genotype 1 and HIV-1: A Phase 3 Study. Clin Infect Dis. 2014;59(11):1579-1587.
53. Cotte L, Braun J, Lascoux-Combe C, Vincent C, Valantin M, Sogni P, et al. Telaprevir for HIV/Hepatitis C Virus-Coinfected Patients Failing Treatment With Pegylated Interferon/Ribavirin (ANRS HC26 TelapreVIH): An Open-Label, Single-Arm, Phase 2 Trial. Clin Infect Dis. 2014;59(12):1768-1776.
54. Zopf S, Kremer AE, Neurath MF, Siebler J. Advances in hepatitis C therapy: What is the current state - what come's next? World J Hepatol. 2016;8(3):139-47.
Recibido: 20 de septiembre de 2016.
Aprobado: 6 de febrero de 2017.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}