










 Custom services
Custom services English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
PermalinkINTRODUCTION
Nocardiosis is a localized or disseminated infection caused by an aerobic microorganism, partially acid resistant alcohol, of the genus of Gram-positive, branched bacteria, with more than 50 species that cause infection; It is usually an opportunistic pathogen that is found in patients with suppurating and granulomatous diseases, (which usually begins in the lungs and can spread to other organs and systems, most often, to the brain and skin. It can also involve the kidneys, the joints, the heart, the eyes and the bones (Arango et al, 2014). The different species of Nocardia are pathogenic bacteria of low virulence; therefore they are clinically significant as opportunistic infections. The nocardial virulence factors are catalase enzymes and superoxide dismutase (which inactivate reactive oxygen species that would otherwise be toxic to the bacterium in addition to "cord factor" that interferes with macrophage phagocytosis preventing phagosome fusion with the lysosome (Murray & Rosenthal, 2006).
In the Central Nervous System, it is uncommon, only 2% of brain abscesses (Brown & McNeil, 2003) (Lin et al, 2010) (Patel & Clifford, 2014) (Chow, 2018). It usually affects immunocompromised patients and is very rare in immunocompetent patients (Guzmán et al, 2017). In both causes a significant morbidity and mortality. Most infections caused by Nocardia are acquired by inhalation of the bacteria or through skin inoculation secondary to trauma (Brown & McNeil, 2003) (Lin et al, 2010) (Patel & Clifford, 2014) (Chow, 2018) (Zheng et al, 2014).
We present the case of a male patient, who developed a non-atherosclerotic cerebral vascular occlusion in the course of a systemic Nocardia infection associated with secondary immunodeficiency due to chronic liver disease, probably caused by excessive alcohol intake.
The objective of this work was to characterize a patient with general and neurological symptoms as a form of presentation of a Nocardiosis with involvement at the cerebral vascular level.
MATERIALS AND METHODS
Clinical case: Male patient, 59-year-old, right-handed craft, with a personal history of hypertension and diabetes mellitus controlled, and chronic liver disease. As toxic habits, frequent and excessive intake of alcoholic beverages is included. Epidemiologist by profession (attending the Leprosy and Tuberculosis Program in his province). The patient debuts with gait disorders primarily with decreased muscle strength of the lower left limb, accompanied by sphincter disorders manifesting urinary incontinence. Two months later, he presented with abundant, shining hemoptysis, preceded by cough. He is admitted to the Pulmonology Service of his provincial hospital; after 3 days the motor picture worsens, deepening the preexisting left hemiparesis, it moves to the Intermediate Therapy Unit and subsequently, if a brain tumor is suspected, it is transferred to the Neurosurgery Service of said Hospital where a brain biopsy is performed by a stereotaxic device which resulted in cerebritis-meningitis. Neurological symptoms remained stable, so he was discharged. Later, clinical manifestations began to occur where an acute febrile syndrome (39-40 oC) was prevalent, which yielded with antipyretics and sometimes the presence of intermittent icterus was identified, and antibiotic treatment was prescribed in the health area improving its clinical manifestations.
Referred from Camagüey arrives at our center (Institute of Neurology and Neurosurgery), with a clinical picture of high fever, left hemiplegia and icterus accompanied by a general syndrome given by asthenia, anorexia and weight loss.
RESULTS
Through a neurological physical examination, a conscious patient was identified, with normal language, conserved superior psychic functions, and a motor defect, hyperreflexia, positive Babinski, left spasticity and normal sensitivity were found. Rest of the neurological examination was normal, including the fundus. Hemochemistry studies were performed on the first day, which were normal except for the glutamic pyruvic transaminase, which showed mild hypertransaminemia, at 62 U/I. Lumbar puncture is performed with cerebrospinal fluid studies, the cytochemical was normal; the negative Chinese ink; in Gram staining of cerebrospinal fluid no bacterial structures were observed; cerebrospinal fluid culture in blood agar and chocolate agar was negative; the microscopic examination for acid resistant bacillus alcohol was negative, as was the immunoglobulin M (IGM) for Toxoplasma IgM; HIV seronegative and non-reactive VDRL serology; blood culture without bacterial growth.
The simple computed axial tomography showed hypodense lesions in the frontal-parietal and right paramedian region without midline displacement (Fig. 1), the Electrocardiogram and Echocardiogram were normal. Due to the presence of a high fever and a probable infectious neurological syndrome, it was decided to start treatment with Cefepime (2 g) every 12 hours x 10 days.
Other studies were performed during admission: Chest Rx: normal; abdominal ultrasonography: hepatomegaly of plus or minus 2 cm was observed, of preserved eco-structure, no dilation of bile ductus, cholecystectomy pancreas, spleen, normal kidneys, without adenopathy.
Evolutionary hemochemistry studies were indicated which showed erythrosedimentation: 80 mm/h; glutamic oxalacetic transaminase: 104 U/I; glutamic pyruvic transaminase: 115 U/I; gamma glutaryl transferase: 231 U/I; triglycerides: 3.9 mmol/L, rest of the normal parameters including the coagulogram.
It was evaluated by multiple specialties among them: Nutritionist recommended the need of intervention in eating habits. Gastroenterology: raised a chronic cholestatic liver disease and Neurophthalmology: no evidence of ophthalmological alterations.
The following results were obtained from the imaging studies performed: Cerebral Magnetic Resonance Imaging where hypo-intense lesions in territory 1 and hyper-intense in territory 2 were demonstrated in vascular territories of the right and middle right cerebral arteries; in diffusion sequences, restriction was observed in relation to recent ischemic lesion of the right anterior cerebral artery and middle cerebral artery (Fig. 2).
The digital subtraction arteriography showed a fine-tuned right internal carotid artery with absence of normal vascularization in the anterior cerebral artery and middle cerebral artery terminal branches, normal remainder (Fig. 3 and Fig. 4).
TSA Doppler: Left carotid atheromatosis with a 50% stenosis with the presence of fibrous plaque type IV.
The histopathological study of brain tissue obtained by stereotaxic biopsy with Hematoxylin-Eosin stains, acute inflammatory infiltrate based on polymorphonuclear and neutrophils was observed and with the silver methylamine technique evidenced the presence of clustered filamentous bacteria, compatible with infection by Nocardia (Fig. 5 and Fig. 6).
The brain tissue sample was also sent to the Department of Microbiology and said Microbiological diagnosis:
In the cultures made in Columbia-based agar with 5% sheep blood, in Saboreaud dextrose agar and in chocolate agar, dry colonies, with a musty smell, white, adherent to the medium, developed, which turned yellowish with prolonged incubation at temperature environment at 72 hours.
Gram staining was performed, and phenotypic study described below, we do not have molecular biology studies.
Catalase test was performed which was positive, negative motility, use of Simmons citrate positive, use of negative adenine, casein hydrolysis (7 days) negative, use of hypoxanthine (7 days) negative, use of tyrosine negative, production of negative gas from positive rhamnosa, growth at 45 oC negative, use of positive glucose, use of negative acetamide.
The other cultures were carried out following the conventional methodology established in the technical marches of the Laboratory and showed no development of other aerobic bacteria, strict anaerobic bacteria, fungi or mycobacteria.
Antimicrobial sensitivity was performed by the epsilometric method (E test Liofilchem s.r.l, Italy). The cut-off points, expressed in ug/mL, were those recommended by NCCLS (Murray & Rosenthal, 2006): sensitive amikacin ≤ 8; resistant ≥ 16; Amoxicillin-sensitive clavulanic acid ≤ 8/4, intermediate 16/8, resistant ≥ 32/16; Cetriaxone sensitive ≤ 8, intermediate 16-32, resistant ≥ 64; trimethoprim-sulfatoxazole: sensitive ≤ 2/32; resistant ≥ 4/76; Ciprofloxacin: sensitive ≤ 1, intermediate 2, resistant ≥ 4; Clarithromycin: sensitive ≤ 2, intermediate 4, resistant ≥ 8.
The active antibiotics (in µg/mL) were: trimethoprim-sulfatoxazole (0.064), Ciprofloxacin (0.032), amoxicillin-clavulanic acid (0.50) and Amikacin (0.125).
The microorganism was resistant to Cetriaxone (> 32) and clarithromycin (> 32).
The patient was treated with Trimetropin-Sulfamethoxazole, at the dose of 15 mg/kg intravenously of the Trimethoprim component, divided into four daily doses, for three weeks. With this therapy the clinical manifestations disappeared and a significant improvement of the neurological signs was achieved. The patient was discharged with 2 tablets of Trimethoprim-Sulfamethoxazole 160/800 mg, twice a day until one year was completed and follow-up by Gastroenterology and Neurology.
DISCUSSION
Nocardia is a Gram positive aerobic bacillus, which has a filamentous appearance, sometimes branched, difficult to identify with Hematoxylin-Eosin staining, and partial resistant acid-alcohol using Ziehl-Neelsen staining. It is a saprophyte of the soil. Its access door to the organism is through the lung fields, occasionally through the skin and digestive system (Chow, 2018) (Lin et al, 2010). It is more common in adult males, although it can occur in both sexes at different ages. This pathology intervenes as determining and predisposing factors among which the underlying lung diseases, malignant tumors of the Reticulum-lymphoid, organ transplantation, the use of glucocorticoids at immunosuppressive pharmacological doses in prolonged or short-term treatments are recognized, and other immunosuppressants, condition observed in half of the affected patients (Greenwood et al, 2002). May cause localized and systemic disease. The most affected organs are the skin and lungs, and hematic spreads in the brain, heart and kidney (Brown & McNeil, 2003) (Chow, 2018) (Patel & Clifford, 2014) (Ishotoya et al, 2017).
Nocardia brain abscess is very rare, occurs from a pulmonary focus, manifests insidiously, in days or weeks (Ishitoya et al, 2017). Most cases have the most striking symptoms: headache, fever, neurological deficit, focus signs, seizures, nausea and vomiting, neck stiffness and papilledema (Southwick, 2007), (Brown-Elliot et al, 2006) (Corti et al, 2008) (Fellows et al, 2007) (Kilincer et al, 2006) (Laurent et al, 2003).
Computed Axial Tomography, Magnetic Resonance Imaging and puncture culture are used for diagnosis. The treatment is carried out based on antibiotics, the most useful is Trimetropin-Sulfamethoxazole, Computed Axial Tomography-guided drainage and tumor excision and enucleation (Lin et al, 2010) (Murray & Rosenthal, 2006) (Patel & Clifford, 2014).
Previously, Nocardia asteroids were considered the most common pathogen in man, but recently it has been discovered that most strains of this bacterium were misclassified, and that Nocardia asteroids could very rarely be associated with the disease. Other species of interest are Nocardia basilienses (causative agent of the disease in immunocompetent) and Nocardia otitidiscaviarum (formerly Nocardia caviae) (Murray & Rosenthal, 2006). The most common form of disease in humans is a slowly progressive pneumonia, whose common symptoms include cough, dyspnea (shortness of breath). All organs can be affected if a systemic spread occurs; in approximately 25-33% of patients, Nocardia infection takes the form of encephalitis and / or the formation of a brain abscess (Chow, 2018).
To treat Nocardiosis, it is necessary to carry out prolonged antibiotic therapy (usually with sulfa drugs) for 6 months to a year or for longer, depending on the patient's response to treatment (Chow, 2018) (Guzmán et al, 2017) (Lin et al, 2010). Often, chronic inhibitory therapy is needed (prolonged therapy with low doses of antibiotics). The patient's prognosis depends on the affected organs, severity of the infection and the patient's immune response, with a significant mortality rate when there is more than one site involved (disseminated nocardiosis) (Sorrell et al, 2005) (Sorrell et al, 2015).
In our patient, taking into account the age of 59, with vascular risk factors such as hypertension, diabetes mellitus, left carotid atheromatosis demonstrated by Doppler of the Supra Aortic Trunks and a history of harmful toxic habits such as excessive alcohol intake, and malnutrition, In addition, presenting a general syndrome associated with a picture of focal neurological deficit and respiratory and abdominal manifestations, several diseases were suspected such as cerebral tuberculosis, neurosyphilis and other sepsis due to opportunistic and atypical germs that cause secondary vasculitis (Southwick, 2007) (Branaud et al, 2005) the possibility of encephalitis or lymphoma secondary to HIV infection was also considered.
The microbiological confirmation is important to make the diagnosis, the culture media that were used were Columbia based agar with 5% sheep blood, in Saboreaud dextrose agar and in chocolate agar; as well as gram staining and other routine identification methods already referred to in the microbiological diagnosis (Duarte, 2013) (Hoshino et al, 2007); as well as the diagnosis by pathological anatomy through the processing of brain tissue biopsied with specific stains (Eshraghi et al, 2013).
We present a seronegative patient for HIV with a systemic Nocardia infection with a greater impact of the symptoms in the Central Nervous Systems, according to the clinical, imaging and pathological anatomy diagnosis.
Subsequent evaluations after imposing specific antimicrobial treatment were satisfactory, gradually returning general and neurological symptoms.
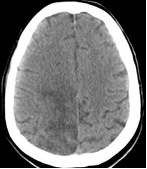
Fig. 1: Simple cerebral computed axial tomography hypodense lesion in the right paramedian parietal region.

Fig. 2: Cerebral Magnetic Resonance Imaging Sequence of axial territory 2. Hyperintense lesion is observed in territory 2 in the right paramedian fronto-parietal region.

Fig. 3: Digital subtraction arteriography and side view of ACD arterial phase internal carotid artery refinement and absence of distal circulation in anterior cerebral artery territory and right middle cerebral artery.

Fig. 4: Simple cerebral computed axial tomography. Suggestive hypodense lesions of ischemic origin in the territory of the right middle cerebral artery and anterior cerebral artery.

Fig. 5: Brain tissue: Silver-methenamine staining technique clustered filamentous bacteria are observed.

CONCLUSION
It is concluded that our patient was characterized as a carrier of a non-atherosclerotic cerebral vascular occlusion in the course of a systemic infection by asteroid Nocardia (opportunistic germ) associated with an immunodeficiency secondary to chronic liver disease and the recommended antimicrobial treatment for this disease was satisfactory.

