










 Custom services
Custom services
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
Permalink
Introduction
Bronchiolitis is mainly caused by respiratory syncytial virus (RSV) although other viruses can be also responsible for this infection.1,2 This is one of the leading causes of infant hospitalization, with around 10% of cases admitted to the paediatric intensive care units (PICUs)3,4,5 with high burden of healthcare costs.1,6,7,8
Paediatric patients with bronchiolitis have a massive neutrophil infiltration that contributes to stopping viral replication but may damage lungs and promote later asthma in severe cases.9,10
The contact between the virus and the epithelial respiratory cells, with toll-like receptors (TLR), activates a local inflammatory response with cytokine that boosts cellular immunity to the infection site. This regulates the activity of T and B cells, improving the virus clearance or, increasing disease severity10,11,12) such as occurs when the Th1 and Th2 subpopulations of CD4+T cells produce imbalanced cytokines. Th1 lymphocytes produce tumor necrosis factor-alpha (TNFα) and interferon-gamma (IFNγ) which enhance the inflammatory response, whereas Th2 lymphocytes produce interleukins 4 (IL-4), 5 (IL-5), 13 (IL-13), which are associated with the promotion of IgE and IL-10 showingan anti-inflammatory response. A prevalence of either Th1 or Th2 cytokines or even a mixed Th1-Th2 inflammatory response has been reported in different studies, with contradictory results that point out the complexity of the regulatory mechanisms that modulate the inflammatory/anti-inflammatory response in bronchiolitis.13,14,15,16,17
Although the treatment of bronchiolitis with corticosteroids is not recommended, it could be assumed that steroids, because of their mechanism of action, will reduce inflammation. Once corticoids are linked to their receptors in the cytosol, the receptor-glucocorticoid complex can either up-regulate the expression of anti-inflammatory proteins in the nucleus (IL-4, IL-10, IL-13) or repress the expression of pro-inflammatory proteins in the cytosol (TNF-α, IL-1α, IL-β, IFNγ, IL-2, IL-3, IL-5, IL-6, IL-8, IL-12).18
Different trials have brought inconsistent results.19 The guidelines of bronchiolitis published in 2014 do not recommend the administration of systemic corticosteroids to infants with a diagnosis of bronchiolitis in any setting.20 The use of inhaled bronchodilators has also shown inconsistent results.21 The Canadian Bronchiolitis Epinephrine Steroid Trial showed, however, a reduction in hospitalizations at 7 days after treatment with combined nebulized epinephrine and oral dexamethasone as compared with placebo, but it was only one large trial.22 Both, the heterogeneous definition of bronchiolitis and the differences among trial designs regarding the reported outcomes affect the strength of evidence, especially in critical patients.19,21
On the basis of the controversy about treatment, it was designed a prospective, randomized, double blind placebo-controlled trial of glucocorticoids in infants of less than 12 months with severe or moderate bronchiolitis to determine whether corticoid therapy influenced the inflammatory response and clinical evolution of critically ill children. We measured a set of interleukins and cytokines as markers of pro- and anti-inflammatory response, as well as different lymphocyte subsets at baseline and at day 7 (end of treatment). Other outcomes related with the clinical response of the patients were also analysed.
This study aimed to assess whether corticoid therapy influenced the inflammatory and clinical response of critically ill infants.
Methods
Single-center, prospective, randomized, double blind, controlled, comparative, interventional clinical trial, conducted in the hospitalization and the pediatric intensive care units of a tertiary hospital.
Time: From November 2011 to April 2014 (last update October 2015). The study was approved by the Ethics Committee of the hospital, with EUDRA registration number CT 2011-000337-36. The study was registered at ClinicalTrials.gov with number NCT02571517. Parents received an information sheet and signed written informed consent prior to the inclusion of infants in the study.
Inclusion criteria: patients less than 12 months of age with severe or moderate bronchiolitis. Exclusion criteria: lack of informed consent, inclusion in other clinical trials, minor bronchiolitis or apnea as a main symptom, previous corticoid therapy, and primary immunodeficiency.
Bronchiolitis was defined according to the guidelines of the American Academy of Pediatrics 2006.6 Patients with a bronchiolitis score BROSJOD ≥ 6 (moderate to severe crisis) were eligible for the study.23
A research team collected parents’ consent, demographic (age, sex, ethnic group) and physical (weight, BROSJOD score, Pediatric Risk of Mortality PRISM-II and underlying disease on admittance) data. The infant was then randomly assigned to receive systemic corticoid therapy (oral or endovenous) or placebo. Patient allocation either to the systemic glucocorticoid therapy group (GCT) or the control group (placebo, non-GCT group) was done by generating a binary series of random numbers (‘random’ function of MS-Excel XP® for Windows®). This procedure generated an equivalent random number of patients in both groups that was only available to the pharmacist who was responsible for preparing the two different treatments. Treatments had the same appearance and only the pharmacist who prepared them knew their composition. Patients, clinicians, nurses, and investigators were blind to treatment allocation.
Daily trial interventions in the GCT group were performed using methylprednisolone e.v. in a dose of 1 mg/kg (twice a day, every 12 hours) or with equivalent doses of prednisolone p.o. in a dose of 1.25 mg/kg (twice a day, every 12 hours). In the non-GCT group (placebo), the treatment contained intravenous sodium chloride (NaCl) 0.9%. or 5% oral glucose sodium chloride (twice a day, every 12 hours).
Date range for participant recruitment was from November 2011 to April 2014. Patients follow-up included one month after the trial inclusion day, and the last patient follow-up finished on October 2015.
Trial intervention was for a maximum of 7 days in accordance with previous studies reporting an improvement in the inflammatory response.24,25,26) When patients improved sufficiently within the first days so as to receive hospital discharge, they were removed from the study.
Apart from the intervention of the trial, all patients were treated as follows: patients under conventional mechanical ventilation (MV) were treated with inhaled salbutamol on demand (auscultation with bronchospasm, or prolonged expiration). Patients with noninvasive ventilation (NIV) were tested for bronchodilator treatment at time of admission. Adrenaline or salbutamol were administered depending on patient age (< 6 months or > 6 months, respectively). If the BROSJOD score decreased 2 or more points after treatment, then the bronchodilator treatment was continued every 4-6 or 8 hours.
Common analytical data were recorded, including lymphocytes, leukocytes, and neutrophils. Lymphocyte subsets (CD4 and CD8) were determined with multiparametric flow cytometry in whole blood. Interleukins and IFNγ were assessed by means of solid phase enzyme-labelled chemiluminescent immunometric assays. Tests for reference values were performed following the manufacturer’s procedures. The etiology of bronchiolitis was determined by multiplex protein chain reaction in respiratory samples.
The main outcomes, measured at baseline and day 7 (end of intervention), consisted of: a) levels of lymphocyte subsets, b) levels of IL-2, IL-12, and IFNγ, and c) levels of IL-4 and IL-10. Although sample size was not calculated for this, secondary outcomes related with the clinical response were recorded and compared when possible: need for PICU admission; length of PICU stay and total length of stay (LOS); occurrence of community-acquired bacterial infection, or nosocomial infection; duration of inotropes, MV, NIV, and high flow nasal cannula (HFNC); need for other rescue breathing-treatments (nitric oxide, high frequency mechanical ventilation, extracorporeal membrane oxygenation); need for continuous renal replacement therapy; occurrence of multiple organ failure; and in-hospital mortality at 28 days.
Considered deviations from the protocol: consent not correctly done or not done; non-compliance with the inclusion or exclusion criteria; lack of clinical or analytical data at the baseline visit or performed outside the established period; failure of the study blind; action performed by a researcher who is not the one indicated; inadequate drug or blind doses.
Data were introduced on a clinical record form and were treated as strictly confidential.
Sample size calculation was done according to the statistical program Ene2.0 ®, taking as main variable the existence of differences in the inflammatory response and clinic evolution of patients with moderate-severe bronchiolitis treated with methylprednisolone/prednisolone compared to those receiving placebo. The null hypothesis (H0) was equality of means between the two treatments to be administered (placebo and methylprednisolone/prednisolone) and the alternative hypothesis (H1) was the existence of differences between the two treatments. Considering a power of 80% to detect differences and a level of significance of 0.05, and assuming that the proportion in the reference group was 0.5, the proportion in the experimental group of 0.8, and that the proportion of units experimental in the reference group with respect to the total was 50% it was be necessary include 39 patients in each group according to the results of the treatment with systemic corticosteroids from previous studies already commented.
After an exploratory analysis, sample size was recalculated and a final sample size of 50 patients in each group was obtained. Per-protocol analysis of primary and secondary outcomes was made by means of chi-square for categorical data, t- test for quantitative variables, and Mann-Whitney test for non-parametric data. Normality was assessed through a Kolmogorov-Smirnov test. Paired data were compared through a Wilcoxon signed ranks test. The SPSS® statistical software package 22.0 (SPSS, Inc., Chicago, III) and R software were used to perform the statistical analyses.
Ethics approval and consent to participate
The study was approved by the Ethics Committee of the Hospital Sant Joan de Déu with the reference and registered at ClinicalTrials.gov with EUDRA registration number CT 2011-000337-36, ClinicalTrials.gov registration number: 2011-000337-36. Parents received an information sheet and signed written informed consent prior to the inclusion of infants in the study.
Results
A total of 327 patients were assessed for eligibility but many of them declined to participate, 97 patients were randomised. One patient was excluded because parents revoked consent, two others due to lack of protocol compliance, and three others because it was required to unbind treatment allocation to allow them to receive additional glucocorticoid therapy. Finally, 53 subjects were assigned to the GCT group, and 44 to the placebo (Fig. 1).
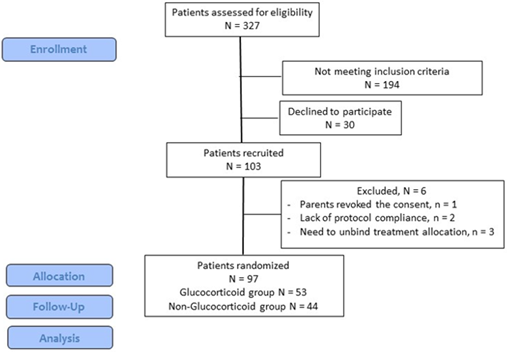
Table 1 shows the main demographic and clinical data.
Other recruited variables were etnia (caucasian in 69, 71.1%), comorbidities (18, 18.5%) and PICU admission (94, 96.9%), no significant differences were found with respect to the treatment group.
Table 1 Demographic and clinical variables between groups at admission
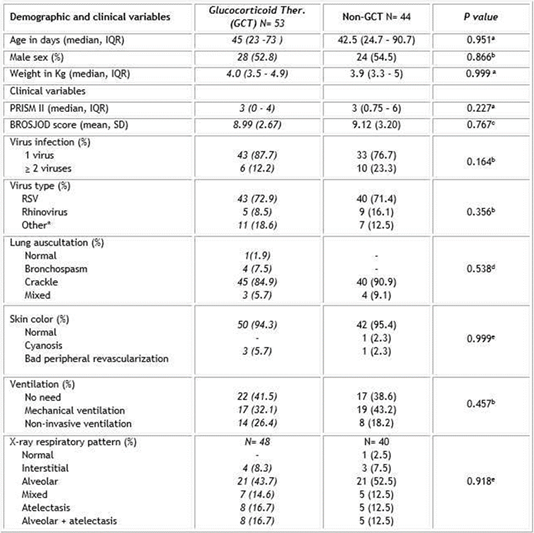
IQR: interquartile range 25-75. PRISM- Pediatric Risk of Mortality. BROSJOD-bronchiolitis score. *Other included adenovirus, metapneumorvirus, parainfluenza, bocavirus, enterovirus and coronavirus.
a Probability value of Mann-Whitney U test; b Probability value of Chi-square test; c Probability value of Student- t test; d Crackle vs the rest of categories have been compared through the Fisher exact test; e Normal vs the rest of categories have been compared through the Fisher exact test; f Normal respiratory pattern has been excluded for Chi-square test calculation.
The main immunological outcomes between days 1 and 7 are shown in Table 2.
Table 2 Immunological outcomes between groups. Levels are indicated as median (IQR). GCT sample size 36; non-GCT sample size 2
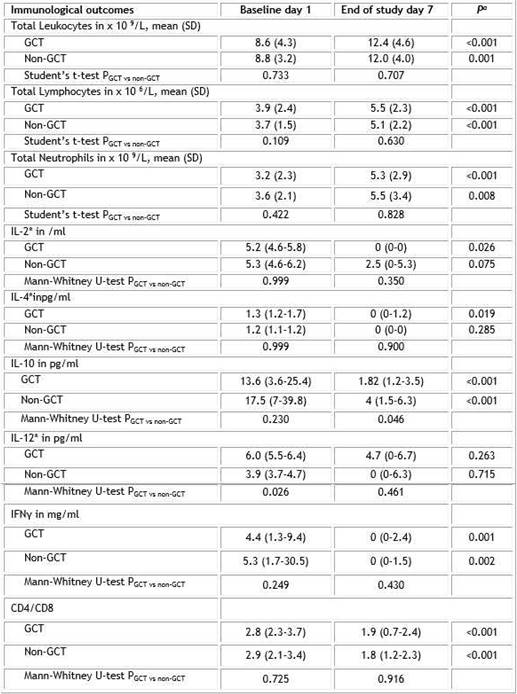
*Only patients with IL values > 0 at baselinewere considered. Pa: Students’t-test probability for paired samples baseline vs end of study; Pb: Wilcoxon signed ranks test probability for paired samples baseline vs end of study.
Lymphocyte subsets ratio (CD4 and CD8) increased from day 1 to day 7 without significant differences between treatment groups. Pro-inflammatory (IL-2, IL-12, and IFNγ) and antiinflammatory (IL-4 and IL-10) markers decreased between day 1 and day 7. The decrease was statistically significant in all cytokines except for IL-12 in both groups, and IL-2 and IL-4 in the placebo group. The only significant difference between treatment groups was observed for IL-10 values at the end of the study (p= 0.046) (Fig. 2).
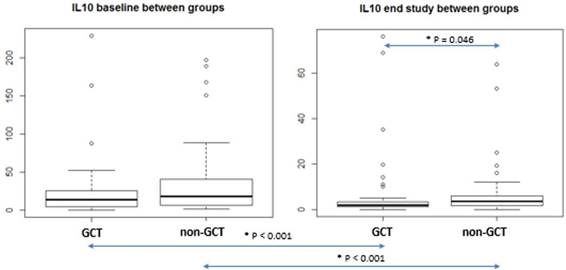
Fig. 2 IL-10 measurements between GCT and placebo (non-GCT) groups at baseline and at the end of the study.
The CD4/CD8 ratio also decreased along the study without differences between groups. No significant differences were detected with regard to secondary outcomes asinotropic or respiratory support requirements, bacterial coinfection and nosocomial infection, and length of PICU and hospital stay (Table 3).
Table 3 Secondary outcomes. Values are indicated as median (IQR) and n (%)
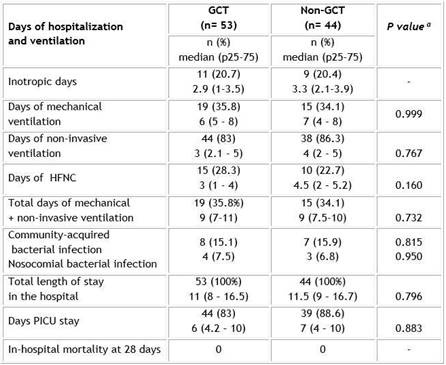
GCT: Glucocorticoid treatment; PICU: Pediatric Intensive Care Unit; HFNC: High-flow nasal cannula; MOF: multiple organ failure; a Mann-Whitney U test.
Even though the GCT group showed, on average, one day less of PICU stay, as well as one day less of MV and NIV. With respect to other outcomes: only one patient required HFVO (in the GCT group); no patients were supported with renal replacement support, and none had MOF or dead during the evolution.
Adverse events did not show differences between treatment groups. Only three non-severe adverse events were detected, all in the GCT group. In all cases, the children recovered without consequences.
Discussion
Regarding the main objective of this study, the administration of systemic corticoids did not significantly modify the inflammatory and clinical response of our patients. In spite of being a homogeneous group of infants less than 12 months of age with an episode of moderate-severe bronchiolitis, the systemic inflammatory response was very similar in the group treated with glucocorticoids and in the placebo group.
Baseline leukocyte and neutrophil count values were found in the low levels of normality in both groups, whereas the lymphocyte count was found in the upper range of age reference values. All these values significantly increased at the second determination, without differences between groups. It is well known that viral infections can debut with a drop in the white cell account, mainly in the number of neutrophils, whereas the lymphocyte count can vary.1,9 Presumably, the administration of glucocorticoids would increase these numbers since it generates the onset of leukocytosis trough neutrophilia. The fact that the GCT group did not show a higher count as compared with the placebo group at the end of the study may be explained by the fact that the duration of the treatment was only 5-7 days.
Pro-inflammatory interleukins and interferon, classically described as activators of the inflammatory response in patients with bronchiolitis, decreased in both treatment groups. Predictably, at baseline, the values were higher after the stimulus generated by the virus responsible for the infection. In the second determination, the natural immune response of the individual would be able to diminish such activation, even in the absence of glucocorticoids. In our study, the GCT group did not show a decrease in a more marked way. It should be noted that, in our study, IL-2, IL-12, and IFNγ already showed remarkably low levels at baseline. This fact is in accordance with a previous study that found that the younger the infants with bronchiolitis, the lower the levels of interleukins and interferon.27 The median age of our patients was 45 days, and thus antiviral immunity, and more specifically antiviral T-cells, could be diminished because of the immaturity of the neonatal immune system.28 Interleukin values in the second determination were practically undetectable, as it has also been described in other studies after 3-4 weeks following baseline determination.27
Anti-inflammatory interleukins IL-4 and IL-10 showed a significant decrease from baseline to the end of the study. IL-10 values at the end of treatment were significantly lower in the GCT group in comparison with the placebo group. Again, it would seem that patients by themselves were able to regulate the anti-inflammatory response by diminishing IL-10 levels after the initial infectious stimulus. In our patients, the inflammatory and anti-inflammatory responses seemed to evolve in a parallel way, independently of the administration of glucocorticoids. However, the significantly lower final levels of IL-10 in the GCT group as compared with the placebo group could be a relevant result. A previous study suggested that higher IL-10 levels in the convalescent phase of patients with RSV bronchiolitis were associated with recurrent wheezing throughout the year after the infection.29 If this finding is confirmed in future studies, the use of glucocorticoids could be recommended for hospitalized patients or for severe cases of bronchiolitis.
The relationship among the pattern of cytokines and glucocorticoids was also explored in a previous study analyzing tracheal aspirates of children with severe bronchiolitis. The authors concluded that dexamethasone did not show any significant effect on the concentrations of 25 cytokines and chemokines involved in the inflammatory response of this infection.30
Given the complexity of the inflammatory response in bronchiolitis, a second objective was proposed aiming at evaluating whether glucocorticoids influenced the clinical evolution of patients, independently of the analytical results. The group treated with glucocorticoids showed one day less of PICU length of stay, MV, NIV and HFNC ventilation in comparison to the placebo group, although the differences were not statistically significant. The mean duration of mechanical ventilation was 1.6 days shorter in a previous study comparing dexamethasone and placebo, and the difference was also not statistically significant.31
Although it has been reported that the infectious etiology of bronchiolitis does not affect outcomes, some studies have linked specific pathogens of bronchiolitis to short- and long-term outcomes and the risk of developing asthma. Influenza virus, for example, showed higher levels of IFNγ (marker of Th1 response) and IL-4 (marker of Th2 response) as compared with RSV and metapneumovirus. With regard to the clinical severity, no differences were detected either for the hospital admission rate or for the presence of bronchospasm among patients infected with influenza, RSV, or metapneumovirus.32,33 Other publications have reported that bronchiolitis by rhinovirus showed a good response to GCT therapy, improving clinical symptoms and showing less risk of wheezing recurrence as compared with placebo.34 In our study, the low number of patients infected with viruses other than RSV does not allow us to draw any solid conclusion. Probably the benefit of GCT might be influenced by the viral etiology of the bronchiolitis due to the different inflammatory response caused by the different respiratory viruses.
No cases of severe adverse reaction attributable to the treatment with glucocorticoids were detected in our study. Three patients with non-severe adverse events were reported. The total number of infections was similar in the systemic GCT and placebo groups. These infections were more likely due to the risk of nosocomial infection of patients admitted to the PICU, the secondary immunosuppression of these patients, and the use of invasive devices.
Although our patients were less than 3 months of age, no cases of hepatic, renal, or hematological toxicity were detected. Likewise, no patients with arterial hypertension or severe hyperglycemia, two of the most common side effects of systemic corticotherapy, were observed, nor did any suffer suprarenal insufficiency after treatment. Consistent with this, studies analyzing the use of corticoids in cases of acute respiratory distress syndrome (ARDS) have reported that the use of high doses of methylprednisolone (30 mg/kg/6h) for a short period (one day) increased the risk of ARDS and death. However, more recent studies concluded that lower doses of methylprednisolone (1-2 mg/kg/day) for at least 1-4 weeks showed beneficial effects on the morbidity and mortality of patients, with scarce adverse events.18
The reduced sample size is the main limitation of this trial especially with regard to the clinical outcomes, although this limitation is a problem detected in most studies in pediatrics, such as those discussed in this paper.27,28,29,33,34 Furthermore, the fact that not all the patients had an available central line for blood extractions, together with their low age, meant that in some cases there was not enough sample available to determine all the variables included in the study. For this reason, the sample size of interleukins, interferon, and lymphoid populations was lower than the number of patients recruited. Otherwise, this clinical trial was not designed in order to analyse this secondary outcomes. The homogeneity of the recruited patients in terms of age, severity, clinical presentation, and evolution could partially overcome these limitations.
The results of this study allow us to conclude that the administration of systemic GCT did not modify the inflammatory and clinical response of very young patients with moderate or severe bronchiolitis, except for IL-10 levels that were significantly lower in the GCT group as compared with the placebo one.
Given the epidemiological and clinical relevance of bronchiolitis and the high health care resources consumed, more clinical trials are needed to conclude on the efficacy of a corticoid therapy, and also on the impact on such treatment on IL-10, and its possible effect on future wheezing. These trials should ideally recruit a greater number of patients, with homogeneous criteria of severity (validated clinical scores) and with different branches of mixed therapeutic options to be useful, especially in patients with severe bronchiolitis.

