










 Servicios personalizados
Servicios personalizados Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
For more than 3 decades, the advent of transradial access (TRA) in the hemodynamics laboratory for catheterization of epicardial coronary arteries and percutaneous coronary intervention (PCI) has shown benefit over transfemoral access (TFA). TRA is associated with lower rates of bleeding, it has also demonstrated a mortality benefit in the population with acute coronary syndrome (ACS).1,2,3,4,5,6,7) Despite these results, the selection of the TRA varies worldwide, in Europe and Asia operators have a higher percentage of TRA for PCI compared to operators in the United States.8 Although recently the National Registry of Cardiovascular Data (NCDR), reported an increase to more than 23% of the primary PCI through the TRA in 2015.9 The Institute of Cardiology of Cuba performs most coronary angiography and PCI through TFA. Given the upward trend of TRA worldwide, this article provides a general description of the initial experience of a femoralist center in the first patients who underwent coronary angiography and/or PCI through the new transradial access.
Coronary angiography through the radial approach was first described by Campeau in 1989.9 Later in 1993, Kiemeneij and Laarman described the first transradial PCI.10 Since then, several studies have emerged comparing TRA with TFA, showing a significant reduction in bleeding and vascular complications with TRA compared with TFA for PCI.11,12 However, Carvalho et al reported only a conversion rate of radial artery to femoral of 5.8%.13
The distal TRA has been of growing interest among radial operators due to improved ergonomics and accessibility of the patient's hand. In an article published by Kiemeneij, inspired by work not reported by researchers in the Russian Federation and Iran, he introduced many in Europe and the United States to the distal left TRA.14 The distal radial artery is located in the anatomical snuffbox of the hand, and in selected patients it can be successfully cannulated (Fig. 1A, 1B, 1C).
Access to the radial artery in the anatomical snuff box compartment facilitates a position of the patient's arm more comfortable for the operator, as well as better ergonomics for the patient.15 It is also believed that it offers better support compared to the right distal TRA, since the catheters are better coupled to the coronary arteries when they cross the aortic arch from the left distal radial artery, by mimicking the TFA. Hemostasis can be achieved in several ways in several studies, it was achieved by applying a traditional vascular band used for conventional TRA. This allows the hand to flex on the wrist, without risk of bruising.16
Several studies have evaluated the safety and feasibility of this new arterial access, Kiemeneij described his experience in the left distal TRA. In this cohort, the failure rate to access the distal left radial artery was 11% (eight patients). No major hemorrhages were documented at the access site. Although there was an acute left distal radial occlusion, no acute occlusion was reported in the proximal segment.14 In the United States, the series by Al-Azizi et al, reported no complications, and the success rate for cardiac catheterization with PCI due to the left distal radial artery was 96.7%.17 Based on these arguments, we evaluate the initial experience in a tertiary care center in Cuba with a cohort of well-selected patients.
Methods
It was a prospective, observational study with consecutive recruitment. The access site to the left distal radial artery was used in 6 patients admitted to the Institute of Cardiology and Cardiovascular Surgery of Cuba (ICCCV) for coronary angiography and PCI. Between May 6 and June 6, 2019. Our study was prospectively designed in accordance with the principles of the Helsinki declaration and obtained the approval of the local ethics committee. All patients were over 18 years old and had a palpable arterial pulse in the anatomical snuffbox. Those with arterial abnormalities or irregularities documented in the Allen, Barbeau test or inverse Barbeau test were excluded.
Prior written informed consent proceeded with the intervention. After checking the appropriate pulse in the anatomical tobacco by manual palpation, with the left forearm in slight abduction, flexed on the abdomen. Then we proceeded with the usual asepsis-antisepsis on the area to be punctured.
Then the left hand was abducted slightly with the thumb under the remains of the fingers, thus making the radial fossa more prominent. The operator was placed on the right side of the patients.
Was infiltrated 2.5 ml of 2% lidocaine in the area selected for puncture, then the artery cannulated with a trocar (20 G) at an inclination between 35-45 ° degrees, directed towards the site where the pulse is palpated with greater intensity. Once access was achieved, confirmed by the presence of adequate flow of arterial blood return, a 0.018 guide was advanced by slightly flexing the forearm, in the direction of the radial artery. Subsequently, 5 and 6 Fr introductors were advanced; and 200 mcg of intraarterial nitroglycerin with 5000 IU of unfractionated heparin were administered for diagnostic studies and up to 10,000 IU in ICP.
Catheter advancement was achieved with a Teflon guide with a J tip of 0.035 inches. For the coronary angiography, left Judkins diagnostic catheters were used for the left and right coronary arteries (Medtronic) for the right coronary 4.0 or 4.5 5Fr for the PCI left or right Judkins guide catheters (Launcher, Medtronic) according to the vessel to be revascularized 3.5, 4.0 6Fr.
Upon completion of the procedure, the radial introducer sheath was removed and early hemostasis is performed. Using manual compression and compression bandage for 15 minutes for coronary angiography and 30 minutes in PCI, then a non-compressive bandage with a gauze swab was left on the access site for 6 h. The pulse of the left radial artery was checked by palpation after the procedure and on discharge.
Quantitative variables considered relevant for the study (failed access, failed procedure, change for femoral access, radial spasms and bleeding according to the B.A.R.C scale) were analyzed. Categorical variables were reported as absolute and relative frequencies and quantitative variables as mean and standard deviation.
Results
The court is composed of 6 patients who underwent coronary angiography by means of the left distal radial access by the anatomical snuffbox, of which in 4, PCI was performed successfully. The average age was 72 years (standard deviation 10 years, minimum age 60 years and maximum 84 years), 5 were man (83.3%). In 1 patient (16.7%), vascular access was failed due to spasm of the distal radial artery, so it was necessary to change to the proximal radial path of the same arm, without having to go to TFA. In all, the angiographic and therapeutic procedure was successfully completed (Table 1).
In no patient was hematoma identified in the anatomical snuffbox or numbness of the hand. In 3 (75%) patients, ICP was successfully performed on the right coronary and only one on the anterior descending. The 10 procedures performed (6 coronary angiography and 4 PCI) were successfully achieved. No patient required hospital readmission or documented vascular or neural complications after the procedure (Table 1).
Characteristics of the procedure
Table 1 Demographic and procedural characteristics of the first patients who underwent coronary angiography and PCI in the ICCCV through the distal radial access.
| Variables | n=6 |
|---|---|
| Middle age years (± DE) | 72 (± 10) |
| Male sex | 5 (83.3%) |
| Vascular access failed n (%) | 1 (16.47%) |
| Failed procedure n (%) | 0 (0) |
| Bleeding B.A.R.C greater than 1 | 0 (0) |
| Radial spasm n (%) | 1 (16.7%) |
| Difficulty advancing catheters in the snuffbox n (%) | 0 (0) |
| Failed Coronary angiography n (%) | 0 (0) |
| Failed PCI n (%) | 0 (0) |
| Hospital readmission n (%) | 0 (0) |
| Vascular complications n (%) | 0 (0) |
| Neural complications n (%) | 0 (0) |
Discussion
The distal radial artery is small, the careful selection of the patient guarantees success in cannulation. For the location of the anatomical snuffbox, the extension of the patient's thumb is indicated (Fig. 1A). This maneuver allows identifying its path and anatomical relationship with neighboring structures.
It is surrounded laterally by the tendons of the abductor of the long thumb, by the extensor of the short thumb and medially by the tendon of the extensor of the long thumb (Fig. 1B). The base and lateral sides of this triangular structure are formed by the distal retinaculum of the extensor muscles and the insertion of the tendons of the extensor of the long thumb, the abductor and the short thumb respectively (Fig. 1A, 1B). The styloid process of the radius, the scaphoid bone, trapezium and the base of the first metacarpal bone constitute the basis of this triangular area (Fig. 1C).8 The distal part of the radial artery it goes deep through the shallow arch. Distally it follows as the deep palmar branch of the radial artery and joins the distal part of the ulnar artery, thus forming the deep palmar arch (Fig. 1C). The distinctive feature of this artery is that its location is distal to the superficial palmar branch, a branch that joins the superficial palmar arch. There are collateral vessels that communicate with the deep palmar arch. So if any occlusion occurs at the site of the superficial artery, tissue ischemia is prevented, due to the maintenance of antegrade flow through the surface between the palmar arch and the communicating collaterals.17
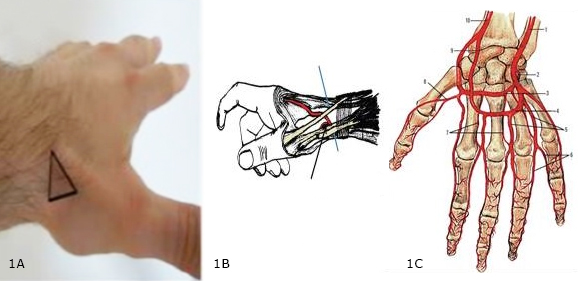
Fig. 1A, 1B y 1C 1A: The left anatomical snuffbox (triangular area) surrounded by the palmar side by the tendons of the long thumb abductor and short extensor of the thumb, and on the dorsal side the tendon of the long thumb extender. 1B: Anatomical snuff catheter site surrounded by tendons, long thumb extender (long blue arrow), short thumb extender and long thumb abductor (short blue arrow). The black arrow shows the radial artery in its distal segment where the puncture is performed. 1C: Blood vessels of the distal forearm and hand: 1 - ulnar artery; 2, 3 - deep palmar branch of the radial artery; 4, 9- superficial palmar arch; 5-digital arteries; 8 - thumb artery; 10 - radial artery. Taken from Soydan et al. Anatol J Cardiol 2018; 19: 243-8 244. (With the permission Sir.Ebru Boz of The Anatolian Journal of Cardiology official journal of the Turkish Society of Cardiology. ISSN 2149-2263 E-ISSN 2149-2271)
This is a small sample, but it is the initial experience of a month of work of the ICCCV, where since its inception the TFA has been and is the preferred one. If we keep in mind that the distal left radial access path through the anatomical snuffbox requires training and a learning curve in operators trained in catheterization by the conventional anterior radial pathway.16 In the figure 2 shows the left distal TRA performed in our catheterization laboratory. Then we will understand the value of the first series until the moment published in Cuba.

Fig. 2 Radial introducer 6 Fr (Terumo) in left distal radial artery. Laboratory of hemodynamics and interventional cardiology of ICCCV.
Among the advantages of the ldTRA over conventional anterior radial, it is mentioned that it has been associated with less radiation for both the patient and the operator18 and may be the preferred access site in patients with internal mammary artery grafts left or in those with a higher risk of failure of the correct TRA such as patients who are <64 inches tall or> 75 years old.18,19
However, the conventional left TRA is associated with greater operator discomfort compared to the right TRA and therefore is not commonly used as the default access site.20) The distal radial access ("anatomical snuffbox") can allow greater optimization of the access site ergodynamics.21,22
The left distal transradial approach (LeDRA) trial was a prospective, observational registry. Between October 2017 and January 2018, 200 patients with a palpable left distal radial artery were consecutively enrolled in a single centre. This study demonstrated very low complication rates. No major haematoma occurred and 7.4% of patients had a minor haematoma. Thirteen (6.8%) patients needed recompression.22
The prospective national registry from the British Cardiovascular Intervention Society (BCIS) including 342,806 cases illustrated that the left RA and right RA had no significant difference in terms of clinical adverse events regarding in-hospital mortality, 30-day mortality, major adverse cardiovascular events or major bleeding. Interestingly, the procedure-related stroke rate was reduced in the left RA according to propensity-matched analysis. Therefore, the use of left distal transradial (ldTRA) approach could reduce procedure-related stroke where operators are proficient in the right RA. A randomised comparison study is needed to uncover the potential benefits and complications of ldTRA.23
The proven benefit of ldTRA compared to the RA or femoral approach is uncertain. However, the absence of radial injury can have a potential benefit in patients requiring arteriovenous fistula and in patients where the radial artery is used as a conduit for coronary artery bypass graft. The distal radial approach (DRA) can also reduce the incidence of potential bleeding complications in patients with a heavily calcified and diseased femoral artery. Whether the DRA can reduce arterial occlusion and bleeding complications requires further investigation.
A newly meta-analysis where 12 randomized studies were found, with a total of 6,450 patients of which 3,217 patients underwent coronary procedures by conventional right radial approach and 3,233 patients by left TRA were distant. The primary end point was the comparison of fluoroscopy time, procedure time, contrast use and crossing rates between two radial accesses. The right radial approach was found to be associated with minimally longer fluoroscopy times (5.8 ± 4.4 min vs. 5.3 ± 4.2 min, mean SD = 0.157, p <0.001) and increased contrast use (84 ± 35 mL vs. 82 ± 34 ml, mean SD = 0.082, p = 0.003). The difference is small but statistically significant in terms of use of contrast and fluoroscopy time in favor of coronary procedures performed by left distal TRA compared to the conventional right radial approach, with no significant difference with the access site or other complications. related to the procedure between the two radial accesses.24
Within the limitations that should be mentioned, it is important to recognize the reduced sample, the descriptive character and the performance in a single center.
The long-term effects of distal radial access are currently unknown, more studies will be necessary to better argue this novel access.
Conclusions
The ldTRA provides an option for access in a subset of patients. However, it requires a learning curve. Patient selection and knowledge of anatomy are crucial to success. More randomized controlled clinical trials comparing different types of access sites (ldTRA with conventional anterior radial) are necessary to evaluate patient outcomes.

