










My SciELO
 Custom services
Custom servicesServices on Demand
Journal

Article
 Spanish (pdf)
Spanish (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkRevista Archivo Médico de Camagüey
On-line version ISSN 1025-0255
AMC vol.19 no.4 Camagüey July.-Aug. 2015
ARTÍCULOS DE REVISIÓN
Fracturas por compresión vertical de columna lumbar
Vertical compression fracture of the lumbar spine
Dr. C. Alejandro Álvarez López I; Dra. Yenima de la Caridad García Lorenzo II
I Hospital Universitario Manuel Ascunce Domenech. Camagüey, Cuba.
II Policlínico Universitario Tula Aguilera. Camagüey, Cuba.
RESUMEN
Fundamento: las fracturas de columna por el mecanismo de compresión axial sin lesión neurológica, constituyen un paradigma en relación a su tratamiento conservador o quirúrgico. Existen controversias en la literatura sobre el tipo de tratamiento de esta lesión.
Objetivo: realizar una revisión sobre los criterios de selección de ambos tipos de tratamiento.
Métodos: se realizó una revisión bibliográfica de un total de 330 artículos publicados en Pubmed, Hinari y Medline mediante el localizador de información Endnote, de ellos se utilizaron 52 citas seleccionadas para realizar la revisión, 46 de ellas de los últimos cinco años donde se incluyeron dos libros.
Desarrollo: se analizaron diferentes factores para decisión del tipo del tratamiento, entre los que se encontraron: la escala de severidad de las fracturas del segmento lumbosacro propuesta por Vaccaro AR, los grados de cifosis, la usurpación del canal medular. Por otra parte se realizó una comparación de diferentes autores en relación al tipo de tratamiento empleado en sus investigaciones y las indicaciones quirúrgicas para sus pacientes.
Conclusiones: basado en la revisión realizada y los estudios consultados, los pacientes con fractura de columna sin lesión neurológica pueden ser tratados de forma conservadora independientemente del grado de inestabilidad mecánica que presenten.
DeCS: PLEXO LUMBOSACRO/lesiones; FRACTURAS DE LA COLUMNA VERTEBRAL; CIFOSIS/terapia; TRATAMIENTOS CONSERVADORES DEL ÓRGANO; LITERATURA DE REVISIÓN COMO ASUNTO.
ABSTRACT
Background: fractures of the spine by axial compression mechanism without neurological lesion are a paradigm in connection with its conservative or surgical treatment. There is controversy in the literature about the type of treatment of this lesion.
Objective: to make a review about the selection criteria of both types of treatment.
Methods: a bibliographic review of 330 articles published in Pubmed, Hinari and Medline by means of the reference management software Endnote was made. Fifty-two citations were selected for the review, 46 of them from the last five years; two books were included.
Development: different factors for deciding the type of treatment were analysed. Some of the factors were the following: severity scale of the fractures of the lumbosacral segment proposed by Vaccaro AR, kyphosis degree, and medullary channel. On the other hand, a comparison of different authors was made according to the treatment applied in their researches and the surgical indications for their patients.
Conclusions: according to the review made and the studies consulted, the patients with fractures of the spine without neurological lesion can be treated conservatively in spite of the degree of mechanical instability they present.
DeCS: LUMBOSACRAL PLEXUS/injuries; SPINAL FRACTURES; KYPHOSIS/therapy; ORGAN SPARING TREATMENTS; REVIEW LITERATURE AS TOPIC.
INTRODUCCIÓN
Las fracturas de la columna (FC) ocupan el 6 % de todas las fracturas y de ellas aproximadamente el 90 % ocurren en las columnas dorsal y lumbar, según plantean Whang PG y Vaccaro AR. 1
Aproximadamente un 20 % de los enfermos presenta algún tipo de lesión neurológica asociada y la mortalidad al año es del 7 % de manera general. 2-4 Los mecanismos de producción de las lesiones de la columna pueden ser simples o combinados entre sí, los tipos de mecanismos más frecuentes son: compresión axial, flexión, extensión, cizallamiento y movimientos rotacionales. 5-7
Al ser las FC provocadas por traumas de alta energía, se asocian por lo general a otras lesiones, en un 30 % se afecta otro órgano o sistema, en un 20 % dos sistemas y en un 5 % tres sistemas o más. 8-10 Para el diagnóstico de esta entidad traumática, se parte desde una exploración física detallada, apoyada en el uso de radiografías simples, tomografías axiales computarizadas y en ocasiones de las imágenes de resonancia magnética. 11-13
Existe un grupo de clasificaciones disponibles para los pacientes con FC y una de las más usadas es la propuesta por Denis F, 14 que divide las fracturas en cuatro grandes grupos: por compresión, compresión axial, flexión distracción y fracturas luxación, que a la vez se subdivide en 16 subgrupos.
Las fracturas por compresión axial son una de las variedades más encontradas y constituyen un verdadero paradigma por su tratamiento, 15-17 en especial cuando no existe daño neurológico, de allí que el principal objetivo de este trabajo es realizar una revisión del tratamiento de esta enfermedad en cuanto a la conducta conservadora o quirúrgica.
MÉTODOS
Se realizó una revisión bibliográfica de un total de 330 artículos publicados en Pubmed (130), Hinari (110) y Medline (90) mediante el localizador de información Endnote, de ellos se utilizaron 52 citas seleccionadas para realizar la revisión, 46 de ellas de los últimos cinco años donde se incluyeron dos libros.
DESARROLLO
Las FC por compresión vertical se caracterizan por fallo de dos de las tres columnas descritas por Denis F, 14 en específico de las columnas anterior y media. Según Ghobrial GM, et al, 18 la incidencia de FC por compresión axial es del 45 % y de ellas el 50 % no presentan lesión de tipo neurológica.
La indicación quirúrgica en pacientes con FC por compresión axial está bien justificada en pacientes que presentan lesión neurológica, sin embargo, cuando no existe esta complicación la selección entre el tratamiento conservador y el quirúrgico es muy difícil. 19-21 Para seleccionar el tipo de tratamiento a emplear se deben tener en cuenta una serie de factores: 22-24
Escala de severidad de las fracturas del segmento lumbosacro: este escala fue descrita por Vaccaro AR, et al, 25 en el año 2005 e incluye un sistema de puntuación basado en tres elementos que son: morfología de la fractura o daño óseo, estado neurológico e integridad del complejo ligamentoso posterior (tabla 1).
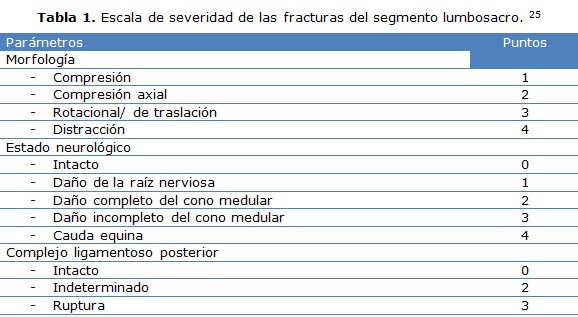
Como resultado de la puntuación de este sistema, todos aquellos enfermos con puntuación menor a cuatro puntos es tratado de manera conservadora y los enfermos con puntuación de cinco son operados, la contradicción fundamental surge cuando el paciente tiene una puntuación de cuatro, situación que por lo general ocurre en pacientes con FC por compresión vertical o axial. 26-28
De allí que todo el interés en este caso recae sobre la integridad del complejo ligamentoso posterior, ya que si la ruptura es indeterminada el valor es de dos puntos, pero si está confirmada es de tres. 29-31
Existen elementos clínicos e imaginológicos que ayudan en determinar esta situación, desde el punto de vista clínico en caso de ruptura de este complejo ligamentoso se puede detectar dolor en la zona afectada de la columna, escalones óseos y edema. 32-34 La imaginología por su parte aporta elementos que hacen sospechar esta lesión, como es el caso de fracturas horizontales a través de los elementos posteriores, aumento del espacio entre las caras articulares y pedículos y la imagen de resonancia magnética, que define la integridad de esta estructura anatómica. 35-37
Joaquim AF, et al, 38 considera la escala de severidad de las fracturas del segmento lumbosacro como no útil, para pacientes con FC por compresión axial.
Cifosis: los grados de cifosis son considerados por algunos autores como determinantes en la selección del tratamiento quirúrgico en pacientes con FC por compresión axial, en especial en enfermos con más de 30 grados y en aquellos con disminución de la altura mayor del cuerpo vertebral mayor al 50 %. Sin embargo, este parámetro por sí solo, sugiere la ruptura asociada del complejo ligamentoso posterior. Los grados de cifosis por sí solo, no justifican la intervención quirúrgica en estos enfermos, ya que los resultados de ambas formas de tratamiento basados en los grados de cifosis son muy similares. 39-41
Usurpación del cana medular: la usurpación del canal medular mayor a un 50 % ha sido considerada por algunos autores 42, 43 como una indicación quirúrgica, sin embargo, este concepto no es aplicable para pacientes sin lesión neurológica, en especial en pacientes con fracturas ostoporóticas. 42-44 Se ha demostrado que pacientes con usurpación de canal mayor al 50 % sin compromiso neurológico, son capaces de tener un proceso de remodelación del canal sin complicaciones posteriores, de allí que este parámetros por sí solo no determina la indicación del tratamiento quirúrgico. 45-47
A continuación se muestra el tipo de tratamiento seleccionado por varios autores en pacientes con FC por compresión axial (tabla 2). 48-50

Al analizar este cuadro se observa que todos los autores coinciden en que los pacientes con FC por compresión axial y lesión neurológica parcial o total, deben ser tratados de manera quirúrgica, ocurre lo mismo cuando se trata de los grados de cifosis y usurpación del canal medular. 51, 52
CONCLUSIONES
Las FC por compresión axial sin lesión neurológica son tratadas de manera conservadora por la mayoría de los autores en la actualidad, el tratamiento quirúrgico no ofrece ventajas sobre el conservador en estos casos, por lo contrario aumenta la estadía hospitalaria, el índice de complicaciones en especial las transoperatorias y el costo para el enfermo.
REFERENCIA BIBLIOGRÁFICAS
1. Whang PG, Vaccaro AR. Thoracolumbar spine fractures and dislocations. En: Bucholz RW, Heckman JD, Court Brwon CM, Tornetta P, editores. Rockwood and Green's Fractures in Adults. 7 th ed. Philadelphia: Williams & Wilkins; 2010. p. 1378-1411.
2. Chen T, Long L, Cao G, Cai Y, Liao W. Treatment of thoracolumbar burst fractures by posterior laminotomy decompression and bone grafting via injured vertebrae. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2014 Oct;28(10):1236-40.
3. Harris MB. Commentary: Thoracolumbar spine fractures: is more knowledge better? Spine J. 2013 Mar;13(3):222-3.
4. Schmidt JH, Sheets NW, Reyes B, Emmett M, Dean S, Snelling B, et al. Thoracolumbar burst fractures treated with the Verte-Span titanium cage. W V Med J. 2012 Nov-Dec;108(6):6-10.
5. Zhang L, Zou J, Gan M, Shi J, Li J, Yang H. Treatment of thoracolumbar burst fractures: short-segment pedicle instrumentation versus kyphoplasty. Acta Orthop Belg. 2013 Dec;79(6):718-25.
6. Jindal N, Sankhala SS, Bachhal V. The role of fusion in the management of burst fractures of the thoracolumbar spine treated by short segment pedicle screw fixation: a prospective randomized trial. J Bone Joint Surg Br. 2012 Aug;94(8):1101-6.
7. Ko SB, Lee SW. Result of posterior instrumentation without fusion in the management of thoracolumbar and lumbar unstable burst fracture. J Spinal Disord Tech. 2014 Jun;27(4):189-95.
8. Kaufman RP, Ching RP, Willis MM, Mack CD, Gross JA, Bulger EM. Burst fractures of the lumbar spine in frontal crashes. Accid Anal Prev. 2013 Oct;59:153-63.
9. Proietti L, Scaramuzzo L, Schirò GR, Sessa S, D'Aurizio G, Tamburrelli FC. Posterior percutaneous reduction and fixation of thoraco-lumbar burst fractures. Orthop Traumatol Surg Res. 2014 Sep;100(5):455-60.
10. Xu G, Fu X, Du C, Ma J, Li Z, Ma X. Biomechanical effects of vertebroplasty on thoracolumbar burst fracture with transpedicular fixation: a finite element model analysis. Orthop Traumatol Surg Res. 2014 Jun;100(4):379-83.
11. Machino M, Yukawa Y, Ito K, Kanbara S, Kato F. The complement of the load-sharing classification for the thoracolumbar injury classification system in managing thoracolumbar burst fractures. J Orthop Sci. 2013 Jan;18(1):81-6.
12. Hofstetter CP, Wang MY. Burst fractures. J Neurosurg Spine. 2014 Feb;20(2):148-9.
13. Nakano M, Kawaguchi Y, Kimura T, Hirano N. Transpedicular vertebroplasty after intravertebral cavity formation versus conservative treatment for osteoporotic burst fractures. Spine J. 2014 Jan;14(1):39-48.
14. Denis F. The three columns of the spine and its significance in the classification of acute thoracolumbar spine injuries. Spine. 1983 Nov-Dic;8(8):817-831.
15. Chen C, Lv G, Xu B, Zhang X, Ma X. Posterior short-segment instrumentation and limited segmental decompression supplemented with vertebroplasty with calcium sulphate and intermediate screws for thoracolumbar burst fractures. Eur Spine J. 2014 Jul;23(7):1548-57.
16. Lee GJ, Lee JK, Hur H, Jang JW, Kim TS, Kim SH. Comparison of Clinical and Radiologic Results between Expandable Cages and Titanium Mesh Cages for Thoracolumbar Burst Fracture. J Korean Neurosurg Soc. 2014 Mar;55(3):142-7.
17. Shawky A, Kroeber M. Shortening spinal column reconstruction through posterior only approach for the treatment of unstable osteoporotic burst lumber fracture: a case report. Arch Orthop Trauma Surg. 2013 Feb;133(2):167-9.
18. Ghobrial GM, Jallo J. Thoracolumbar spine trauma: review of the evidence. J Neurosurg Sci. 2013 Jun;57(2):115-22.
19. Bijukachhe B, Banskota B, Shrestha BK, Banskota AK. Closed internal degloving associated with a thoracolumbar burst fracture: a case report. Eur J Orthop Surg Traumatol. 2013 Nov;23 Suppl 2:S145-8.
20. Joaquim AF, Daubs MD, Lawrence BD, Brodke DS, Cendes F, Tedeschi H, et al. Retrospective evaluation of the validity of the Thoracolumbar Injury Classification System in 458 consecutively treated patients. Spine J. 2013 Dec;13(12):1760-5.
21. Shamji MF, Roffey DM, Young DK, Reindl R, Wai EK. A pilot evaluation of the role of bracing in stable thoracolumbar burst fractures without neurological deficit. J Spinal Disord Tech. 2014 Oct;27(7):370-5.
22. Zheng GQ, Wang Y, Tang PF, Zhang YG, Zhang XS, Guo YZ, et al. Early posterior spinal canal decompression and circumferential reconstruction of rotationally unstable thoracolumbar burst fractures with neurological deficit. Chin Med J (Engl). 2013 Jun;126(12):2343-7.
23. Jiménez-Ávila JM, Ortiz-García V, Ortiz-Soto R. Thoracolumbar spine burst factor. Screw fixation. Acta Ortop Mex. 2013 May-Jun;27(3):170-6.
24. Liao G, Lin J. Letter regarding article by Xu et al. Anterior versus posterior approach for treatment of thoracolumbar burst fractures: a meta-analysis. Eur Spine J. 2014 Apr;23(4):940.
25. Vaccaro AR, Lehman RA Jr, Hurlbert RJ, Anderson PA, Harris M, Hedlund R, et al. A new classification of thoracolumbar injuries: the importance of injury morphology, the integrity of the posterior ligamentous complex, and neurologic status. Spine. 2005 Oct;30(20):2325-33.
26. He D, Wu L, Sheng X, Xiao Q, Zhu Y, Yu W, et al. Internal fixation with percutaneous kyphoplasty compared with simple percutaneous kyphoplasty for thoracolumbar burst fractures in elderly patients: a prospective randomized controlled trial. Eur Spine J. 2013 Oct;22(10):2256-63.
27. Lee JK, Jang JW, Kim TW, Kim TS, Kim SH, Moon SJ. Percutaneous short-segment pedicle screw placement without fusion in the treatment of thoracolumbar burst fractures: is it effective?: comparative study with open short-segment pedicle screw fixation with posterolateral fusion. Acta Neurochir (Wien). 2013 Dec;155(12):2305-12.
28. William KD. Fractures, dislocations and fractures-dislocations of the spine. En: Canale ST, Beaty JH, editor. Campbell's Operative Orthpaedics. 12 th ed. Philadelphia: Elsevier; 2013. p. 1605-27.
29. Hitchon PW, He W, Viljoen S, Dahdaleh NS, Kumar R, Noeller J, et al. Predictors of outcome in the non-operative management of thoracolumbar and lumbar burst fractures. Br J Neurosurg. 2014 Oct;28(5):653-7.
30. Wu H, Fu C, Yu W, Wang J. The options of the three different surgical approaches for the treatment of Denis type A and B thoracolumbar burst fracture. Eur J Orthop Surg Traumatol. 2014 Jan;24(1):29-35.
31. Zhang S, Thakur JD, Khan IS, Menger R, Kukreja S, Ahmed O, et al. Anterior stabilization for unstable traumatic thoracolumbar spine burst fractures. Clin Neurol Neurosurg. 2015 Mar;130:86-90.
32. Jeong WJ, Kim JW, Seo DK, Lee HJ, Kim JY, Yoon JP, et al. Efficiency of ligamentotaxis using PLL for thoracic and lumbar burst fractures in the load-sharing classification. Orthopedics. 2013 May;36(5):e567-74.
33. Scheer JK, Bakhsheshian J, Fakurnejad S, Oh T, Dahdaleh NS, Smith ZA. Evidence-Based Medicine of Traumatic Thoracolumbar Burst Fractures: A Systematic Review of Operative Management across 20 Years. Global Spine J. 2015 Feb;5(1):73-82.
34. Wood KB, Li W, Lebl DR, Ploumis A. Management of thoracolumbar spine fractures. Spine J. 2014 Jan;14(1):145-64.
35. Ray WZ, Krisht KM, Dailey AT, Schmidt MH. Clinical outcomes of unstable thoracolumbar junction burst fractures: combined posterior short-segment correction followed by thoracoscopic corpectomy and fusion. Acta Neurochir (Wien). 2013 Jul;155(7):1179-86.
36. Kang CN, Cho JL, Suh SP, Choi YH, Kang JS, Kim YS. Anterior operation for unstable thoracolumbar and lumbar burst fractures: tricortical autogenous iliac bone versus titanium mesh cage. J Spinal Disord Tech. 2013 Oct;26(7):E265-71.
37. Xu GJ, Li ZJ, Ma JX, Zhang T, Fu X, Ma XL. Anterior versus posterior approach for treatment of thoracolumbar burst fractures: a meta-analysis. Eur Spine J. 2013 Oct;22(10):2176-83.
38. Joaquim AF, Daubs MD, Lawrence BD, Brodke DS, Cendes F, Tedeschi H, et al. Retrospective evaluation of the validity of the Thoracolumbar Injury Classification System in 458 consecutively treated patients. Spine J. 2013 Dec;13(12):1760-5.
39. Chou PH, Ma HL, Wang ST, Liu CL, Chang MC, Yu WK. Fusion may not be a necessary procedure for surgically treated burst fractures of the thoracolumbar and lumbar spines: a follow-up of at least ten years. J Bone Joint Surg Am. 2014 Oct 15;96(20):1724-31.
40. Mattei TA, Hanovnikian J, H Dinh D. Progressive kyphotic deformity in comminuted burst fractures treated non-operatively: the Achilles tendon of the Thoracolumbar Injury Classification and Severity Score (TLICS). Eur Spine J. 2014 Nov;23(11):2255-62.
41. Freedman BA, Serrano JA, Belmont PJ, Jackson KL, Cameron B, Neal CJ, et al. The combat burst fracture study-results of a cohort analysis of the most prevalent combat specific mechanism of major thoracolumbar spinal injury. Arch Orthop Trauma Surg. 2014 Oct;134(10):1353-9.
42. Wang J, Zhou Y, Zhang ZF, Li CQ, Zheng WJ, Liu J. Radiological study on disc degeneration of thoracolumbar burst fractures treated by percutaneous pedicle screw fixation. Eur Spine J. 2013 Mar;22(3):489-94.
43. Schouten R, Lewkonia P, Noonan VK, Dvorak MF, Fisher CG. Expectations of recovery and functional outcomes following thoracolumbar trauma: an evidence-based medicine process to determine what surgeons should be telling their patients. J Neurosurg Spine. 2015 Jan;22(1):101-11.
44. Shang J, Ling XD, Liu YC, Liu W, Xiao XG, Yuan SH. Biomechanical effects of pedicle screw adjustments on the thoracolumbar burst fractures. Chin Med J (Engl). 2013 Jan;126(2):300-5.
45. Soultanis KC, Mavrogenis AF, Starantzis KA, Markopoulos C, Stavropoulos NA, Mimidis G, et al. When and how to operate on thoracic and lumbar spine fractures? Eur J Orthop Surg Traumatol. 2014 May;24(4):443-51.
46. Suzuki T, Abe E, Miyakoshi N, Murai H, Kobayashi T, Abe T, et al. Anterior Decompression and Shortening Reconstruction with a Titanium Mesh Cage through a Posterior Approach Alone for the Treatment of Lumbar Burst Fractures. Asian Spine J. 2012 Jun;6(2):123-30.
47. Howard BM, Sribnick EA, Dhall SS. Complete neurologic recovery of spinal cord injury after posterior transpedicular reconstruction for traumatic lumbar burst fracture. Spine J. 2013 Feb;13(2):204-5.
48. An HS, Vaccaro A, Cotler JM, Lin S. Low lumbar burst fractures: comparision among body cast, Harrington rod, Luque rod, and Steffee palte. Spine. 1991 Aug;16(Suppl 8):S440-4.
49. Mick CA, Carl A, Sachs B, Hresko MT, Pfeifer BA. Burst fractures of the fifth lumbar vertebra. Spine. 1993 Oct;18(13):1878-84.
50. Huang TJ, Chen JY, Shih HN, Chen YJ, Hsu RW. Surgical indications in low lumbar burst fractures: experience with anterior locking plates system and the reduction fixation system. J Trauma. 1995 Nov;39(5):910-4.
51. Butler JS, Fitzpatrick P, Ni Mhaolain AM, Synnott K, O'Byrne JM. The management and functional outcome of isolated burst fractures of the fifth lumbar vertebra. Spine. 2007 Feb;32(4): 443-7.
52. Xu XY, Yan ZJ, Ma Q, Chen L, Ke ZY, Chen F, et al. Clinical application of the paraspinal erector approach for spinal canal decompression in upper lumber burst fractures. J Orthop Surg Res. 2014 Nov 13;9(1):105.
Recibido: 1ro de abril de 2015
Aprobado: 20 de mayo de 2015
Dr. C. Alejandro Álvarez López. Especialista de segundo grado en Ortopedia y Traumatología. Profesor titular. Hospital Universitario Manuel Ascunce Domenech. Investigador agregado del CITMA. Máster en Urgencias Médicas. Doctor en Ciencias Médicas. Camagüey, Cuba. E-mail:
yenima@finlay.cmw.sld.cu

