










My SciELO
 Custom services
Custom servicesServices on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkVaccimonitor
On-line version ISSN 1025-0298
Vaccimonitor vol.19 no.3 Ciudad de la Habana Setp.-Dec. 2010
ARTICULOS ORIGINALES
Invasive Meningococcal Disease. Cuba, 1983- 2006.
Enfermedad meningocócica invasiva. Cuba, 1983-2006.
Antonio E. Pérez*, Félix Dickinson, Rafael Llanes
Instituto de Medicina Tropical "Pedro Kourí". Autopista Novia del Mediodía Km. 6 ½ P. O. Box 601, Marianao 13. La Habana. Cuba.email: antonio@ipk.sld.cu
* PhD. MD with specialization in Epidemiology. Institute of Tropical Medicine "Pedro Kourí".
ABSTRACT
Invasive Meningococcal Disease (IMD) is a worldwide health problem. In Cuba, vaccination against meningococcal B-C has been carried out since 1989. The study aimed at describing the epidemiology of IMD in Cuba from 1983 to 2006 and at contributing to the immunization strategy. A descriptive and analytical study was carried out. Epidemiological data was obtained from the National Surveillance System at the Institute "Pedro Kourí". More than 1 000 cases were reported in 1986 and the overall incidence was above 10/100 000 inhabitants. Since 1989 a remarkable and continuous decline in the incidence was observed. In the last nine years a strong association of IMD to boarding school students (OR=9.4; confidence interval 95%: 5.1-17.4), recluses (OR=5.9; CI 95%: 1.5 -24.3) and day students (OR=3.9; CI 95%: 2.8-5.6) was observed. Housewife (OR=4.9; CI 95%: 1.9-12.4) and pensioned (OR=4.5; CI 95%: 1.2-16.8) showed association with mortality. Previous vaccination was a protective factor against morbidity (OR=0.6; CI 95%: 0.4-1.0) and mortality (OR=0.4; CI 95%: 0.2-0.9) by IMD. Neisseria meningitidis B4:P1.15 was the main circulating strain. Incidence of IMD declined markedly in Cuba by using group BC strain-specific meningococcal vaccine.
Keywords: Invasive Meningococcal Disease, Epidemiology, Risk factors, Neisseria meningitidis, Immunization.
RESUMEN
La enfermedad meningocócica invasiva (EMI) es un problema de salud mundial. En Cuba, la vacunación antimeningocócica BC se ha llevado a cabo desde 1989. El propósito del presente trabajo fue describir la epidemiología de la EMI entre 1983-2006 y contribuir a la estrategia de prevención. Se realizó un estudio descriptivo y analítico de todos los casos confirmados y registrados. Los datos se obtuvieron del Sistema Nacional de Vigilancia en el Instituto «Pedro Kourí». En 1986 se registraron más de 1 000 casos de EMI con una incidencia de 10/100 000 habitantes. Desde 1989 se observó un notable y continuo descenso de la incidencia. En los últimos 9 años se observó una fuerte asociación en la ocurrencia de casos con estudiantes de régimen interno (OR=9,4; Intervalo de Confianza 95%: 5,1-17,4), reclusos (OR=5,9; IC 95%: 1,5-24,3) y estudiantes externos (OR=3,9; IC 95%: 2,8-5,6). Mostraron asociación con la mortalidad las amas de casa (OR=4,9; CI 95%: 1,9-12,4) y los jubilados (OR=4,5; CI 95%: 1,2-16,8). La vacunación previa mostró ser un factor protector para la morbilidad (OR=0,6; CI 95%:0,4-1,0) y la mortalidad (OR=0,4; CI 95%: 0,2-0,9). El principal fenotipo circulante de Neisseria meningitidis fue B4:P1.15. La incidencia de EMI se redujo notablemente en Cuba a partir del uso de la vacuna antimeningocócica específica del grupo B.
Palabras clave: Enfermedad meningocócica invasiva, epidemiología, factores de riesgo, Neisseria meningitidis, inmunización.
INTRODUCTION
Invasive Meningococcal Disease (IMD) is a severe bacterial infection caused by Neisseria meningitidis, a leading cause of bacterial meningitis and/or septicemia. It represents a relevant worldwide health problem.
In most countries, attack rates of endemic IMD is 1 to 5/100 000 inhabitants. In the sub-Saharan African meningitis belt the endemic incidence may be over 20/100 000 population (1).
In developed countries such as the United States, a substantial proportion of cases of meningitis and sepsis are caused by N. meningitidis (2). The incidence of IMD was estimated to be 0.7_1.4/100 000 population, and the case-fatality rate (CFR) is approximately 10%. Both the incidence rate and CFR have been relatively constant, with no major changes observed in the past decade (3).
The most common manifestations of IMD include meningitis (50-55% of cases), septicemia (5-20%), and meningitis accompanied by septicemia (20-30%) (4).
Left untreated, the disease can lead to fatality rates greater than 50% and despite treatment 10% of patients die quickly while 10-20% survivors develop neurological sequels (5).
Cuba is among the countries that were affected by an epidemic on meningococcal disease since 1976 for what has carried out different vaccination strategies. In 1979, there was a vaccine campaign using serogroup C polysaccharide vaccine, targeting age under 19 years old. After this, N. meningitidis serogroup B prevailed and based on encouraging results in efficacy trials (6), the Ministry of Public Health carried out in 1989 a mass vaccination campaign of two doses of a combined serogroup C and B vaccine. This vaccine, known as VA-MENGOC-BC® (Havana, Cuba) contains purified proteins from outer-membrane of group B meningococci from strain Cu385/83; B:4;P1.15 (7).
The vaccine was administered to the high risk population below 20 years of age achieving almost 95% coverage. Later, in 1991 vaccine was added to the National Immunization Program (NIP), targeting infants at the age of 3 and 5 months with an average coverage superior to 90% (8,9). Since then, Cuba have been registered the cumulative of 10 479 779 doses up to 2006 (10).
The present paper shows the main epidemiological features of IMD in Cuba during the last 23 years including results previous and after the immunization.
MATERIALS and METHODS
Data source
This study included all confirmed and registered cases of IMD (9429) from 1983 to 2006, on the basis of the following definition: "a clinical meningeal syndrome and/or septicemia, through the identification of N. meningitidis directly by culture of the cerebrospinal fluid (CSF), blood, petecchias and by Gram stain results or indirectly by latex agglutination techniques" (11). In view of the severity of IMD, the National Program for Control and Prevention of the Infectious Neurological Syndrome endorse hospitalization of all IMD cases in Intensive Care Units. The conventional bacteriologic diagnosis of N. meningitidis is available in hospital laboratories network along the country. On the other hand, Ministry of Public Health requires the mandatory report of IMD by all health-care providers, laboratories and health-care facilities.
A database on IMD was obtained from a full-coverage nationwide Surveillance System from 1983 by an epidemiological questionnaire processed at the Institute "Pedro Kourí" (IPK). Since 1998, improvement of the existing surveillance system (12) allowed the inclusion of other pathogen causing bacterial meningitis, as well as socio-demographic data (attendance to day care centers or boarding students, worker, unemployed, housewife, pensioned, military, recluses, and previous specific vaccination status considering that all people under 37 years old may be vaccinated in campaign or by NIP).
Laboratory methods
The strains isolate recovered were sent to the National Reference Laboratory for Neisseria (NRLN), IPK for microbiological confirmation and strain typing. All N. meningitidis isolated from normally fluid specimens (blood, cerebrospinal CSF or both) and received at NRLN-IPK were cultured using modified Thayer Martin medium, incubated at 37 °C, in 5-10% CO2, for 48-72 hours according to handbook of operations and proceedings on NRLN at IPK- Reference National Laboratory.
Identification of N. meningitidis colonies was made by glucose and maltose oxidation in cystine tripticase agar (CTA) medium base (Difco) and by the production of y-Glutamyl aminopetptidase enzymatic activity. Serogroups were determined by slide agglutination with polyclonal antiserum to serogroups A, B, C, W135, X, Y and Z (Difco, USA). Strain serosubtyping was based on the detection of outer membrane protein (porin) antigens of class 2/3 (designate serotypes) and OMP class 1 (define subtypes) using a standard set of monoclonal antibodies obtained from the National Institute for Public Health, The Netherlands (3).
Statistical methods
Based on chronological series of cases we estimated the incidence rate (/100 000 inhabitants) and CFR by age groups, per year using estimates of Cuban population data obtained from the National Office of Statistics.
Proportional differences were calculated as follows (Incidence Rate Initial - Incidence Rate ending) / Incidence Rate Initial * 100 taking 1989 as initial period and 2006 as the ending.
In order to assess the association of IMD with socio-demographic variables, a selective prevalence study (13) was used, including 1 716 cases of bacterial meningitis registered from 1998 to 2006 (377 cases of IMD and 1 339 cases of meningitis caused by both, Streptococcus pneumoniae and Haemophilus influenzae type b).
Associated variables (RR ³ 1.5) in the bivariate analysis and the vaccination status (population under 37 years olds vaccinated with VA-MENGOC-BC® since 1989) were additionally analyzed by using multiple logistic regression model. The model was fitted including all the exploratory variables and subsequently dropped one by one until only those that were associated (OR >2).
Similarly, the association of the above mentioned factors with mortality was made by comparing deaths versus survival and also assessed by bivariate and logistic regression model.
In Addition, 95% Confidence intervals and statistically significant (p<0.05) were also estimated.
A sample of 314 meningococcal strains was characterized out of 1 254 strains received at NRLN-IPK from 1989 to 2006.
EPIINFO 2000 version 3.3 and Excel (version 5.1) were used for statistical analysis.
Ethical considerations
The present study did not require approval from an Ethics Committee. The Cuban Ministry of Public Health is the governmental organization responsible for the collection of infectious disease notifications, hospital discharge records and population or laboratory surveillance. The management of these data for public health purposes requires neither a patient's informed consent nor any authorization regarding privacy laws in Cuba.
RESULTS
Morbidity
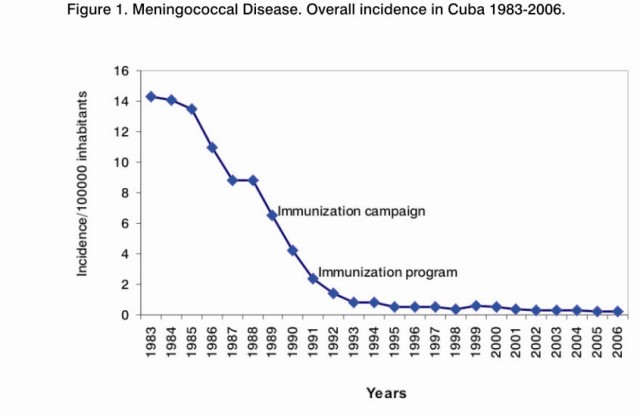
IMD epidemic caused by serogroup B started in Cuba during 1980, the number of cases reached the peak in 1983 with 1420 cases registered and an incidence rate of 14.3/100 000 inhabitants. Overall, IMD decreased over time and rates were decreasing slowly before vaccination (1989).
From 1984 to 1986, more than 1000 cases (annual incidence rate >10/100000 inhabitants) were reported annually. The annual incidence rate during 1987-1988 was 8.8/100 000 inhabitants (nearly 900 cases). An important reduction (26.1%) of overall incidence was observed between 1988 and 1989 (8.8 versus 6.5/100 000 inhabitants) respectively (Table 1 and Figure 1). Since 1993 the continuous decreasing trend reached rates <1/100 000 inhabitants.
Reduction of the overall incidence from 1989 to 2006 was 96.9% and the most important decrease was observed in children from 1 to 4 years (97.5%), 5 to 14 years (96.3%) and infants (94.5%).
Since 1998, infants continued with the highest rates although falling, but in 1 to 4 and 5 to 14 age groups incidence rates were nearly 1/100 000 inhabitants. The other groups had incidence rates <0.5/100 000 inhabitants (Table 1). When infants were excluded, mean age of patients was 21.9 years (standard deviation was 22.1) and the median age was 13 years.
Among infants the disease was reported more frequently at 6 months of age (13.8%) reaching 61.6% of cumulative percentage. Only two infant were less than 30 days old.
Nine socio-demographic variables were studied from 1998 to 2006. A total of 51 students attended boarding schools (IMD=34), 178 were day students (IMD=86), 8 were recluses (IMD=4), 2 military (IMD=1) and 1 041 may have received previous vaccination (IMD=292) (data not shown).
Bivariate and Multivariate analysis are shown in Table 2.
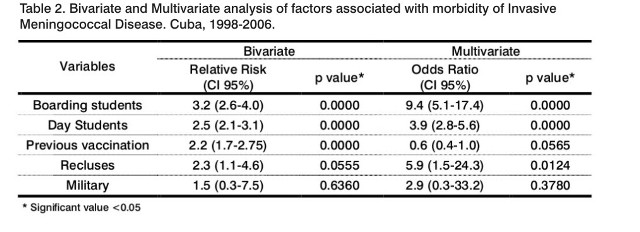
Logistic regression analysis showed association with boarding students, day students and recluses. Patients previously vaccinated (OR=0.6; CI 95%: 0.4-1.0) showed protection to IMD (Table 2).
Mortality
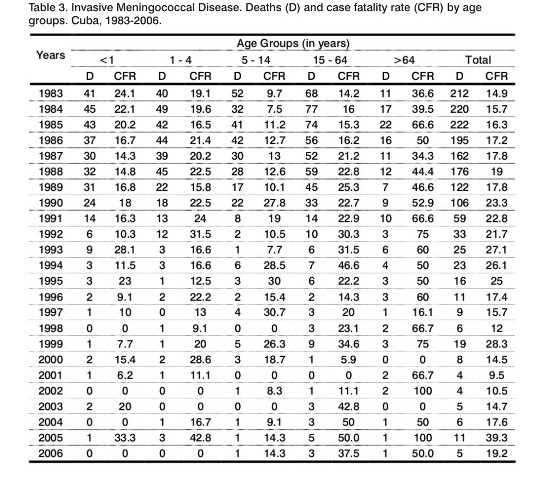
It was registered nearly 200 deaths during the peak of the epidemic, decreased continuously and reaching an annual average of 6 deaths since 2000 (Table 3). The highest CFR was observed in 2005, 1999, 1993 and 1994 with 39.3%, 28.3%, 27.1% and 26.1% respectively. In general, the elderly showed the highest CFR. Since 1998 the mean age of fatality (excluding infants) was 36.8 years old and the median was 36 years old. Only 7 infants died and four of them (57.1%) were six months of age or older.
Bivariate analysis only showed association with housewives (RR=3.8; CI 95% 2.5-5.7), pensioned (RR=3.5; CI 95% 2.0-5.9), workers (RR=1.7; CI 95% 1.0-2.9). Logistic regression analysis demonstrated association with housewives (OR=4.9; CI 95%: 1.9-12.4) and pensioned (OR=4.5; CI 95%:1.2-16.8). Previous immunization as a protective factor against mortality was also observed (OR=0.4; CI 95%: 0.2-0.9).
Laboratory surveillance
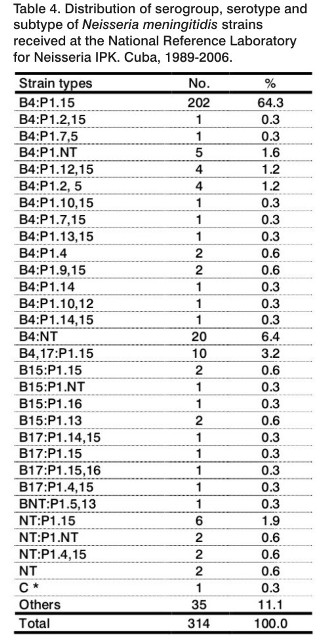
From 1989 to 2006, a sample of 314 meningococcal strains (25.0% of 1 254 strains received) was characterized at NRLN-IPK. All strains belonged to serogroup B except one (serogroup C) that was isolated in 2001 from a foreign patient. The majority of strains (64.3%) belonged to phenotype B4.P1.15. A lower frequency of strains with different sero-subtypes was detected (Table 4).
DISCUSSIÓN
The Cuban Health System is based on a nationwide free-health service with total access and equal opportunity for every citizen to access medical care, hospitalization, vaccination, social assistance and other services (8).
Incidence of IMD decreased slowly from 1984 to 1987. The incidence stabilized during 1987 and 1988, but a subsequent and marked decline was observed from 1989 following a mass vaccination campaign in population < 20 year old, demonstrating the impact of this intervention. A continuous and high coverage vaccination through NIP allowed keeping low incidence (8). Nevertheless, we wonder what would have happened (a hyper endemic or a re-emergence epidemic) if the referred strategy with specific meningococcal vaccine under these circumstances had not been used.
In a different strategy aiming to reduce the incidence of an epidemic caused by phenotype B4:P1:15 in Sao Paulo, Brazil, only children aged from 3 months to 6 years were vaccinated (1989-1990) with the same specific vaccine used in Cuba, a little or no measurable effect on this outbreak was observed (14). Recently, the Global Advisory Committee on Vaccine Safety recognized the safety of outer membrane-vesicle meningococcal B vaccines based on their usage in Cuba, France, New Zealand and Norway (15).
In 2007, it was estimated that 1 000 cases of IMD occurred in the United States, with 130 (13%) case fatalities and equal rate of morbidity, including primarily amputations and hearing loss. It was considered that protection against IMD will require eliciting durable serum antibody present at the time of acquisition of N. meningitidis, and sufficient antibody to decrease colonization in adolescents and young adults, if the goal of population-based reduction in disease is to be achieved (16). Serogroup B prevails in Cuba as observed in other studies developed in the United Kingdom, where the majority of strains belong to serogroup B or C (17), and in Germany (18), where 70% of N. meningitidis strains belong to serogroup B. In spite of the low incidence in Cuba, it is necessary to observe the future behavior of IMD very close, considering that the vaccination program is only addressed to serogroup B and C, and an emerging serogroup or new mutant strains may arise (19).
It has been reported that after 12 years of the immunization with VA-MENGOC-BC® (Havana, Cuba) in teenagers, only 42% had ³ 1:4 of bactericidal antibodies titers against N. meningitidis B4:P1.19.15, and a booster dose response achieved 57% of seroconvertion of the antibodies titers (20). The possible association between previous vaccination and IMD found with the bivariated analysis could be explained taking into account the wide coverage of the Cuban immunization program, and that the most population has been vaccinated with VA-MENGOC-BC®. On the other hand, multivariate analysis proved protection with previous vaccination showing the real behavior of a complex phenomenon. These results permit the development of accurate and timely adjustments to both the immunization program and the policy to ensure their ultimate success.
An important and recent result of our surveillance system is the assessment of socio-demographic factors associated to IMD. Strong association with attendance to boarding school, recluse, day attending student, is coincident with reports in close settings. (21, 22). Mortality was strongly associated with housewives and retired people, which are unvaccinated and regularly older people have predisposing conditions. CFR is more related with health care and other factors beyond the purpose of this paper. Previously, we pointed out that vaccination is important to reduce mortality and severe clinical forms. High CFR observed among the elderly might be likely due to poorly recognizable clinical features in this vulnerable group (23). On the other hand, it is important to highlight that the main circulating N. meningitidis type B4:P1.15, belonging to the ET5 complex is characterized by a high virulence (24).
A new meningococcal B vaccine in a nationwide vaccination program was recently assessed in New Zealand, showing an effectiveness of 73%. The conclusion was that further observation is needed to determine whether the three-dose will provide longer lasting protection, although in infant a fourth dose was recommended (25).
In the United States IMD is more frequent between the ages of 2 to 18 years old, therefore meningococcal vaccine is recommended in the immunization schedules at different range of age (2 to 6 years old and 11 to 12 years old) (26). Recently the Advisory Committee on Immunization Practices (ACIP) recommends meningococcal vaccination with MCV4 at 3 years after receipt of MPSV4 for children 2-10 years who are at increased risk for IMD (27). In Cuba, the last autochthonous meningococci strains different to serogroup B (serogroups A and C) were confirmed by the NRLN in 1986. Therefore, now it is the moment to consider the use of a booster dose to provide longer lasting protection for serogroups B and C in target groups as toddlers and adolescents.
Acknowledgments
We thank Irene Toledo and Oderay Gutiérrez for their technical contribution to the surveillance system and to the National Reference Laboratory.
We are also grateful to epidemiologists and microbiologists from different provinces for providing information and strain collection.
We also thank Dr. Caroline Trotter for the advice and comments on the manuscript.
REFERENCES
1. WHO.World Health Organization. Control of epidemic meningococcal disease. WHO practical guidelines. 2nd Edition. WHO/EMC/BAC/98.3;1998.
2. Rosenstein NE, Perkins BA, Stephens DS, Popovic T, Hughes JM. Meningococcal disease. N Engl J Med 2001;344:1378-88.
3. Rosenstein NE, Perkins BA, Stephens DS, Lefkowitz L, Cartter ML, Danila R, et al. The changing epidemiology of meningococcal disease in the United States, 1992-1996. J Infect Dis 1999;180:1894-901.
4. Connolly M, Noah N. Is group C meningococcal disease increasing in Europe?.A report of surveillance of meningococcal infection in Europe 1993-6. European Meningitis Surveillance Group. Epidemiol Infect 1999;122:41-9.
5. WHO.World Health Organization. Enhanced surveillance of epidemic meningococcal meningitis in Africa: a three-year experience. Weekly Epidemiological Record 2005;80:313-20.
6. Sierra G, Campa C, Varcárcel M, García L, Izquierdo L, Sotolongo F, et al. Vaccine against group B Neisseria meningitidis: Protection trial and mass vaccination results in Cuba. NIPH Annals 1991;14:195-207.
7. Sierra G, Campa C, García L, Sotolongo F, Izquierdo L, Valcárcel M, et al. Efficacy evaluation of the Cuban vaccine VA-MENGOC-BC against disease caused by serogroup B Neisseria meningitidis. In: M Atchman et al. Neisseria. Berlin:Walter Gruyter; 1990 p. 129-34.
8. Pérez A, Dickinson F, Baly A, Martínez R. The epidemiological impact of antimeningococcal B vaccination in Cuba. Mem Inst Oswaldo Cruz 1999;94:433-40.
9. Pérez A, Dickinson F. Resultados del Programa Nacional de Inmunización antimeningocócica BC en menores de 1 año en Cuba. Rev Cub Pediatr 1998;70:133-40.
10. MINSAP.Ministerio de Salud Pública. Morbilidad. Total de dosis aplicadas según tipo de vacuna. En: Anuario Estadístico de Salud 2006. Dirección Nacional de Estadística. Ciudad Habana. Cuba, 2007 p. 102.
11. WHO recommended surveillance standards for surveillance of selected vaccine preventable diseases. World Health Organization. 2003.Available at: http://www.who.int/vaccines-documents/DocsPDF06/843.pdf.(Accessed: 13 January 2009).
12. Pérez A, Dickinson F, Tamargo I, Sosa J, Quintana I, Ortíz P, et al. Resultados y experiencias del sistema nacional de vigilancia de meningitis bacterian en Cuba. Biotecnología Aplicada 2003;20:1-5.
13. Kleinbaum D, Kupper L, Morgenstern H. Hybrid designs. Typology of Observational Study Designs. In: Epidemiologic research: principles and quantitative methods. Chapter 5. New York: Wiley & Sons, Inc; 1982. p. 70-6.
14. Sacchi CT, de Lemos AP, Camargo MC, Whitney AM, Melles CE, Solari CA, et al. Meningococcal disease caused by Neisseria meningitidis serogroup B serotype 4 in Sao Paulo, Brazil, 1990 to 1996. Rev Inst Med Trop Sao Paulo 1998;40:65-70.
15. WHO.World Health Organization. The Global Advisory Committee on Vaccine Safety, 12-13 December 2007. Safety of meningococcal B vaccines. Weekly Epidemiological Record 2008; 83:42-43.
16. Pelton SI. Prevention of Invasive Meningococcal Disease in the United States. Pediatr Infect Dis J 2009; 28:329-32.
17. Stuart J, Smyth GB, Ramsay M, Patterson CW, Monk P, Mackenzie R, et al. Guidelines for public health management of meningococcal disease in the UK. Commun Dis Public Health 2002;5:187-204.
18. Reintjes R, Kajueter H, Ehrhard I, Van Treeck U, Ammon A. Applying a case cross-cover study design to examine transient exposures in the transmission of Neisseria meningitidis. Europ J Epidemiol 2005;20:629-33.
19. Maiden MCJ, Caugant DA. The population biology of Neisseria meningitidis: implications for meningococcal disease epidemiology and control. In: Frosch M, Maiden MCJ, Wiley-VCH, editors. Handbook of Meningococcal Disease. Weinheim, Germany: Verlag GmbH & Co. KGaA; 2006. p.17-34.
20. Camaraza M, Martínez I, Ochoa R, Arnet A, Sotolongo F, Hernández D, et al. Respuesta de anticuerpos inducidos por la vacuna antimeningocócica cubana VA-MENGOC-BC frente a la cepa de Neisseria meningitidis B:4:P1.19,15 en adolescentes después de 12 años de inmunizados. VacciMonitor 2006;15(3):1-4.
21. Baltimore RS, Jenson HB. Meningococcal vaccine: new recommendations for immunization of college freshmen. Curr Opin Pediatr 2001;13:47-50.
22. Harrison LH, Dwyer DM, Maples CT, Billmann L. Risk of Meningococcal Infection in College Students. JAMA, 1999;281:1906-10.
23. Pérez A, Dickinson F, Baly A, Martínez R. Repercussion of VA-MENGOC-BC on the mortality by meningococcal disease in Cuba. Rev Panam Infectol 1999;3:56-63.
24. CDC.Centers for Disease Control and Prevention. Serogroup B meningococcal disease-Oregon, 1994. MMWR 1995;44:121-24.
25. Kelly C, Arnold R, Galloway Y, O'Hallahan J. A prospective study of the effectiveness of the New Zealand meningococcal B vaccine. Am J Epidemiol 2007;166:817-23.
26. CDC.Centers for Disease Control and Prevention. Recommended immunization schedules for persons aged 0-18 years-United States. MMWR 2007;55:1-6.
27. CDC.Centers for Disease Control and Prevention. Report of the Advisory Committee Immunization Practices (ACIP): Decision Not to recommend Routine Vaccination of all children aged 2-10 years with Quadrivalent Meningococcal Conjugate Vaccine (MCV4). MMWR 2008;57:462-5.
Recibido: Marzo de 2010
Aceptado: Junio de 2010


{kind=link}
{kind=link}
{kind=link}
{kind=link}