










 Custom services
Custom services English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
PermalinkINTRODUCTION
Systemic Lupus Erythematosus (SLE) is a relatively frequent disease of universal distribution. Its incidence varies according to the characteristics of the studied population such as age, gender and ethno.
It is a chronic and autoimmune disease, which cause is not clear at all, although some ethiopathogenic factors are invoked, existing a production of autoantibodies against auto antigens with the consequent formation of multiple immunocomplexes that lead to inflammatory answers once they get diverse organs and tissues. The patients can present a wide range of clinical manifestations and of laboratory that go from symptoms and characteristic parameters that can be a diagnosis occasionally to unspecific findings common to other diseases. 1-3)
The SLE goes with exacerbations and remissions that can be related with risk factors, increasing the frequency of reactivation of the disease, such as exposition to sun, infections, surgical procedures, stress situations, pregnancy, oral contraceptives intake. It is difficult in occasions to determine whether it is an outbreak, an infection, a complication of the treatment or an undercurrent disease.4,5)
The SLE can appear at any age, but in the majority of patients it stars between 15 and 40 years of age, with a female predominance of 9-10:1. The disease appears before 15 years of age in a 10-15 % of cases and in a similar percentage after 50-55 years of age. The age of the starting symptoms may modify the clinical and immunologic characteristics of the patients. In patients with starting age before 15, the relation female/male is 7:1 and usually suffer from more severe ways of the disease mainly nephropathy, neurologic affection and thrombopenia.
In the SLE of delayed beginning (above 50-55 years of age) the relationship between the sexes is of 4-6:1, due probably to the appearance of menopause and the resulting diminish of estrogens production.1,5,6
The global incidence varies between1-10 cases per 100.00 inhabitants/ year. In Europe, the rate spreads since 2, 2 new cases in Spain to 5 cases in France, while in United States the rate spreads from 0,7 to 7,2 new cases due mainly to ethnic differences of the population.1,2,7-9
The measure of real prevalence is difficult to establish because it varies mainly according to considered ethnic communities. In Europe patterns have been reported from 25 cases per 100.000 inhabitants on Ireland to 40 in France and 91 in Spain. In Unites States figures have been reported between 7 and 253 cases per 100.000 inhabitants depending on variables such as methodology used, sex and ethnicity.1,8,9
The measures of incidence and prevalence are 2-3 times higher among Afro-American, Asian and Spanish populations than in Caucasians and the highest rates are observed between native North Americans and aboriginal Australians. Equally, ethnicity is also associated with differences in the clinical course of the disease and the patients of Afro-American, Latino American and eastern origin present more severe forms with a major renal affection and an increased morbimortality.1,8-10
Approximately 4 to 5 decades, the patients diagnosed with Systemic Lupus Erythematosus had a life expectancy below 5 years, however, with the improvement of new diagnostic tests and the applying of new therapies, the surviving of these patients has increased a lot.1,9-12
Cuba shows rates of incidence and prevalence very similar and an increase of new cases per year can be seen. The evolution of the patients is variable depending on the ethno and the region.
The present study has been designed with the general objective of characterizing of clinical and epidemiological way the patients with diagnosis of SLE at Arnaldo Milián Castro University Hospital of Villa Clara, Cuba. The frequency of appearance according to sex, age, previous history and toxic habits will be pointed out as well as the more affected systems. Used treatments and main causes of death will be taken into account.
METHODS
A developmental, observational, descriptive and transversal investigation was carried out at Arnaldo Milián Castro University Hospital of Villa Clara, Cuba from September 2016 to September 2018. The population of study was formed by all the patients with diagnosis of systemic lupus erythematosus older than 18 years of age that were assisted from January 2008 to December 2017 in the clinical services of the previously mentioned institution. The sample was selected of unprovable way by criteria being formed by 112 patients that accomplished the following conditions:
Criteria of inclusion:
To be a patient with diagnosis of systemic lupus erythematosus.
Criteria of exclusion were related with:
Patients with diagnosis of this disease that were assisted due to other causes not related with SLE.
Techniques and procedures:
The documented analysis served as support of the investigation. Its object was the personal clinical chart and the clinical chart of the hospital. Its objective was the gathering of information related to socio-demographic and clinic variables associated to the diagnosis of the patients that formed the sample. All the data were collected in a guide of documented review made by the main author. Variables such as age, sex, personal pathologic antecedents, toxic habits, more affected systems, treatments carried out and more frequent causes of death were used.
For the statistical process of information, the data obtained were put in a card index, using the electronic tabulator Microsoft Excel 2016, including the data corresponding to the variables of study that were put in a data base of SPSS version 19.0 which permitted to make tables and/or graphs; showing distributions of absolute and relative frequencies as well as average among ages and maximum and minimal values. From the inferential point of view Square Chi (X2) was applied to demonstrate significant differences among percent in tables on only one entrance, through a test of B.
Pearson´s correlation coefficient was used as a measure of lineal association to confirm the relation among variables. Together with the value of Square Chi (X2) its corresponding significance was shown. (p)
According to the value p, its difference or association was classified in:
Very significant: If (p) is ˂ 0.01
Significant: If 0.01 ˂ (p) ˂0.05
Not significant: If (p) ≥ 0.05
Bioethical considerations: During the development of the investigation, ethic and legal structures were considered in the obtaining of information, according to Helsinki statement and the established by the commission of international ethics (autonomy, beneficence, not evil talk and justice). The information of the cases was only used by the authors; also, the results are only for scientific purposes, data that could serve to identify the studied sample were not included.
RESULTS
Table 1 shows the distribution of patients according to age groups and sex, where it can be seen that the female sex prevailed with 105 patients, for a 93,7 % and the age group of 39-44 patients for a 39,3 %.
There were very significant differences when comparing the rate of patients by sex.
There were very significant differences when comparing the rate of patients by age groups.
Table 1 Distribution of patients by sex and age groups.

Source: clinical charts. Sex: X2( 85, 75 p(0,000 Age groups: X2( 31, 40 p(0,000
As is shown in Table 2, the results of the study appear according to personal previous history, where it was found a predominance of arterial hypertension with 27 patients that represented a 24,1%.
When comparing the patients´ ratio according to personal previous history very significant differences were found.
Table 2 Distribution of patients according to personal previous history.
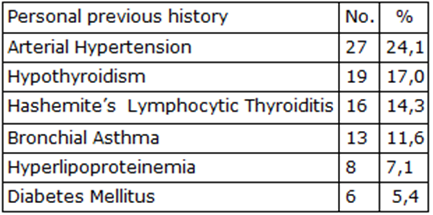
Source: clinical charts. X2( 19, 87 p(0,001
It is shown in Table 3 the distribution of patients according to toxic habits where it can be observed that the first place was occupied by coffee intake in 41 patients for a 36,6 %.
When comparing the rate of patients according to toxic habits very significant differences were found.
Table 3 Distribution of patients according to toxic habits.
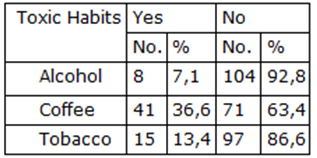
Source: clinical charts. X2( 28, 34 p(0,001
As can be seen in Table 4 in the distribution of patients according to more affected systems, the osteomyoarticular one had the highest representation of cases with 42 patients, demonstrating the 38,0%, followed by skin and mucosa affection with 33 patients for a 29,5 % of the total of the sample. When comparing the ratio of patients with more affected systems very significant differences were found.
Table 4 Distribution of patients according to more affected systems.

Source: clinical charts. X2( 70, 76 p(0,00
It is shown in Table 5 the combinations of medication more used throughout the disease where it is observed that the most used combination was prednisone plus azathioprine in 86 patients representing a 76,8 %.
When comparing the proportion of patients by combinations of more used medication in a year after diagnosis very significant differences were found.
Table 5 Combinations of medication more used throughout the disease.
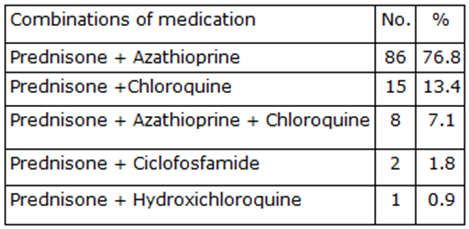
Source: clinical charts. X2( 166, 08 p(0,000
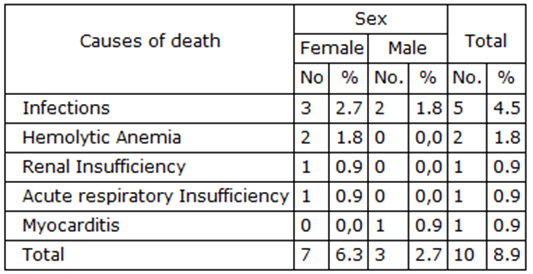
Table 6 shows the distribution of patients by causes of death and sex, where it can be observed that from the sample of study only10 patients died, representing an 8,9 %; 7 of the female sex for a 6,3 % and 3 of the male sex for a 2,7 %.In both sexes infection prevailed with a total of 5 patients representing the 4,5 % of dead people due to this cause.
When comparing the amount of patients by causes of death and sex significant differences were not found.
DISCUSSION
It is shown in table 1 the relation of patients according to age groups and sex, where the female sex and ages from 30 to 39 years old prevailed greatly. The obtained data coincide with the statements that appear in the literature, as it designates that the clinical picture of SLE tends to appear at any age , but in the majority of patients it starts between 15 and 40 years of age with a peak if incidence in 29-32 years of age. It has a female predominance with a relation woman/man of 9-10:1. The disease appears before 15 years of age in a 10-15 % of cases with a similar percentage over 50-55 years of age. The starting age of symptoms can vary the clinical and immunologic characteristics of the patients. In patients with a starting age below 15 years old the relation woman/man is 7:1 and they usually suffer from more severe forms of the disease.
In the delayed appearance of SLE (over 50-55 years of age) the relationship between sexes is 4-6:1, possibly due to the appearance of menopause and the consequent diminish of estrogens production.1,5,6
Several studies have been focused in the influence of the sex during the course of the disease. There is a controversy in United States and Canada about this topic, although when it is present in the masculine sex it has a tendency to be more aggressive. In Latin America the disease has a more obscure course in men.1,6,13
According to a study carried out by Dra. Guibert Toledano, the SLE the same as other autoimmune diseases, appears with a highest frequency in women. In general, the percentage of affection of the female sex fluctuates between 78 and 96 % in various sequences, figure that remains in Spanish series. Moreover, sex can also modify the way of presentation of SLE. 14
These results also coincide with a studied performed in Colombia about defects of expression, where the female sex prevailed and there was a similar correspondence in relation to age groups.15
In Mexico the prevalence of SLE in higher in women than in men, the same in white as in black people.(11.16)
Estevez del Toro developed a study at Hermanos Ameijeiras Hospital where it was stated that 76 patients belonged to the female sex (95 %) and 4 of the male sex (5 %). The middle age of the cases was of 29 ±10 years. 16. This study coincides with the investigation performed where the female sex is also more frequent.
According to the author’s criteria and based on observational studies carried out, sex has a great influence in the evolution of SLE and in many occasions it is related with severe forms of the disease above all in the male sex.
It has been observe in practical medicine that male patients with a diagnosis of SLE have a higher incidence of pericarditis than women.
Table 2 shows the distribution of patients according to personal previous history where it can be seen that patients with arterial hypertension prevailed. In the consulted literature the variable arterial hypertension is referred as personal previous pathological history and it is stated that arterial hypertension is very frequent as a cause of renal compromise and the treatment with glucocorticoides and nonesteroidal antinflammatory drugs (NSAD). Renal involvement occurs in the 60-75 % of patients.17
It is known that environmental factors play a vital role as they can act as trigger factors of the disease, above all in individuals genetically susceptible; moreover, genetic factors develop a significant role in the development and the presentation of Systemic Lupus Erythematosus. (10, 17-20)
According to author´s criteria arterial hypertension is not a predisposing factor for the development of SLE that is a chronic disease with a high incidence and prevalence in Cuba, that’s why in the majority of epidemiological studies indicate a high incidence and prevalence in the population. The truth is that the treatment of Lupus may determine the appearance of arterial hypertension when high doses of steroids and antinflammatory drugs are taken. Also, studies done to rule out renal damage should be taken into account. Sometimes there are hypertensions resistant to treatment.
Table 3 shows the distribution of patients according to toxic habits. It can be observed that coffee intake predominated with 41 patients for a 36,6 % of the studied sample, in relation with alcohol and tobacco consumption, existing very significant differences.
Toxic habits are predisposing factors of many diseases that´s why they are a variable to be considered in any study carried out on adult populations.
This result coincides with what is stated in the literature and with studies carried out in Philadelphia an in the Section of Immunology and Allergology of the University of Chile where it is confirmed the high incidence of people who tale coffee, including people with SLE, but the direct relationship between this toxic habit and the appearance of SLE has not been proved.
In other developed studies the presence of toxic habits in patients with SLE has been confirmed, that could be in relation with an aggravation of patients, but depending on the consumed toxic habit.22-24)
According to the author´s criteria, although coffee represents a risk factor for the appearance of many diseases, it doesn´t have direct relationship with the lupus.
Table 4 represents the distribution of patients according to more affected systems. It can be seen that the system with a higher representation was the oateomyoarticular with 42 patients for a 38,0 %, followed by the cardiovascular with 33patients for a 29,5 % of the whole sample.
These results coincide in order of frequency with the studied carried out by Dr. Estévez del Toro at Hermanos Ameijeiras Hospital and the literature described by other authors, who state that the Systemic Lupus Erythematosus is a chronic inflammatory disease, of unknown cause that courses with cutaneous-mucosa and ostoemyoarticular affection in more than the 60% of cases, although it also affects other systems with a high frequency.16
Updated literatures state that the 90 % if the patients with SLE have an affection of the motor apparatus throughout the disease, above all, arthritis and arthralgias.1,2,5,9,25
The higher skin affection could be due to the ultraviolet light that could alter the DNA structure, increase its antigenicity and induce apoptosis of the keratinocytes, getting free a great quantity of antigens.1,9,18,20,26
In other studies carried out skin lesions have been found in the 80 % of patients, and are part of the criteria of the disease classification (photosensitivity, mouth aphta, malar exanthema and discoid lesions)
Photo sensibility is generally associated with the presence of antibodies anti Ro and both are frequent manifestations together with the mouth aphta. Raynaud phenomenon appears to be present in the 60 % of the cases.14,27-29)
According to the author´s criteria the fact the Cuba is a tropical country influences in a high degree because the ultraviolet rays fall stronger, affecting the skin directly.
It is shown in table 5 the distribution of patients according combinations of medication more used throughout the disease where it can be seen that the highest representation of this variable was the combination of prednisone with Azathioprine found in 86 patients which represented the 76,8 % of the whole sample.
Ortega carried out an epidemiological study where the frequency of infections was evaluated in relation with the use of immune suppressor treatments in patients with lupus.
It was confirmed that the 80 % of the patients had designated a treatment combined by azathioprine and prednisone although in flexible doses. In this study it was also proved that the 96,5 % of the patients had a treatment with prednisone.29
This corresponds with the results obtained in the present study, as well as other multicenter investigations where the frequent use of steroids and conventional anti rheumatic medication has been recorded. Generally, steroids were used in low doses, but in severe cases, doses of 1-2mg/kg.14,16,27-29
These results coincide with the ones obtained in the study performed in the Unit of Rheumatology at Roosevelt Hospital that consisted in the administration of combinations of medication in patients with lupus, with the purpose to evaluate the answer to treatment. The patients received systemic steroids: metilprednisolone 1g/day and prednisone 1mg/kg/day, the modifier drugs of the disease were: methotrexate, azathioprine and cyclophosphamide. The more effective long term combination was prednisone and azathioprine.30
In other investigations the studied samples have used biological therapies with cheering and satisfactory results.31) The truth is that these therapies have revolutioned the patients´ evolution and prognosis, their use in the majority of cases is reserved for those that do not respond to conventional therapies. Belimumab is the prescribed one in patients with SLE.
According to the author´s criteria these drugs combinations are related with the organ or system affected, with the intensity of clinical manifestations and patient’s answer to a determined medication, that is, according to therapeutic adherence and with the level of accessibility of the patients to different treatment options.
In table 6 from the results about the distribution of patients by causes of death and sex, it can be observed that from the total of the sample only 10 patients died representing an 8,9 %, 7 of the female sex for a 6,3 % and 3 of the male sex for a 2,7 %. In both sexes infections prevailed for a total of 5 patients that represented the 4,5 % of dead patients by this cause.
Infections constitute the more frequent complication in patients with SLE, which could be greatly due to the immunosuppressor treatment that they receive. The recurrence of infections in these patients tend to be a frequent and complex phenomenon with severe consequences for the patient.13,32,33
In a multicenter study that included 1000 patients of seven European cities, infections were present in 270 people (27 %) that represented the 28,9 % of deaths. Similarly, a retrospective study carried out in Brazil, where the result of 113 autopsies of patients with SLE were evaluated, it was found that infection was the cause of death in the 58 % of cases.13
In a study carried out by Dr. Yamelis Ortega in Villa Clara province, where morbidity of SLE was evaluated, it was demonstrated that 65 patients had been admitted at the Rheumatology Service due to any kind of infection, after being their first cause of death up to 70 % of the cases.29
Other studies demonstrate that approximately a 10% of the patients die after 5-10 years of diagnosis, in which infections play an essential role.1,34
Rua- Figueroa state in studies done that morbidity in patients with lupus is associated to high doses of immunosuppressor treatment as well as the frequency of infections; also, in some cases it is related to treatment abandon.9)
Other literatures validate that the surviving of SLE after 10 years is 75-85 % according to sequences. Prognosis is much better because the diagnosis is earlier every time, there are less severe forms of lupus and also more effective therapies have been developed. Apart from complications due to infections, patients can present aggravation due to lung damage, renal damage among others.1,32-34
The author considers that whenever possible and taking into account the relationship risk-benefit, low doses of steroids and in the least possible time, to reduce this way the risk of infections. The routine checking of the patients permits the finding of possible complications on time, taking actions in the least possible time, reducing this way the morbidity and the mortality.
CONCLUSION
Patients between 30 and 39 years of age were the most representative, with a higher incidence in the female sex. Arterial hypertension prevailed as personal pathologic antecedent. Coffee was the most represented habit .there was a major affection of the osteomyoarticular system followed by skin and mucosa. Prednisone and Azathioprine were the most used medications. Infections were the main cause of death.

