










My SciELO
 Custom services
Custom servicesServices on Demand
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkPodium. Revista de Ciencia y Tecnología en la Cultura Física
On-line version ISSN 1996-2452
Rev Podium vol.17 no.3 Pinar del Río Sept.-Dec. 2022 Epub Sep 12, 2022
Original article
Biokinematic analysis of gait in patients with hemiplegia
1Facultad de Cultura Física. Universidad de Holguín. Holguín, Cuba.
2Centro Provincial de Rehabilitación de las Ataxias Hereditarias. Cuba.
3Universidad Central del Ecuador. Ecuador.
4Unidad Educativa del Milenio" Jatun Kuraka Otavalo". Ecuador.
Introduction:
A biokinematic analysis of gait was performed in patients with hemiplegia, which is the paralysis of one side of the body, recognized in the context of medical sciences and therapeutic physical culture as hemiplegic syndrome.
Objective:
It consisted of determining the biokinematic modifications that are manifested in the gait of patients with hemiplegia in the "Pedro Díaz Coello" health area of Holguín.
Materials and methods:
The sample consisted of five patients who received systematic care in the rehabilitation room of the health area of the " Pedro Díaz Coello" polyclinic in the municipality of Holguín. The interviews conducted with medical and physical rehabilitation personnel who work in the health area, with researchers from the Faculty of Physical Culture and Sports of the University of Holguín, the review of normative documents on multidisciplinary work and the observation of rehabilitation sessions, showed the need to address the issue from biomechanics, given the limited quantification of its indicators. In order to analyze the behavior of biokinematic indicators of pathological gait, the videographic technique was used. With the Kinovea software, in version 0.8.27, the controlled indicators were quantified.
Results:
Together with the qualitative study for each patient, it allowed a comparison of the characteristics of their gait with the normal pattern and the elaboration of a group of recommendations to be considered during the physical rehabilitation process.
Conclusions:
It was possible to analyze the behavior of the biokinematic indicators of hemiplegic gait in the patients studied, their comparison with normal gait, as well as a set of recommendations to be taken into account in the rehabilitation process
Key words: Biomechanical control; Gait; Hemiplegia; Rehabilitation; Videography.
INTRODUCTION
Hemiplegia means complete paralysis of one half of the body, including the arm and leg. One of the most frequent causes of hemiplegia is a cerebrovascular accident, an injury caused by the interruption of the blood supply to any of the parts of the brain." A stroke can lead the person who suffers it to a great disability and limitation in activities of daily living, especially in motor activity" (Dutill, Echemendía, Núñez, 2020. p.2). It is also called brain attack, brain attack, brain infarction, stroke, embolism or cerebral thrombosis, which interrupts the blood supply to a certain region of the brain and, as a consequence, causes death of the brain tissue corresponding to the affected artery. However, there are other causes that produce it such as: cerebral hemorrhage, arterial thrombosis, arterial embolism and trauma. "One of the main sequelae caused by cerebrovascular diseases is the decrease in voluntary motor function and strength in the hemibody contralateral to the injured hemisphere, known as hemiparesis or hemiplegia" (Fitz-Allan, Lozada. 2022. p 58).
Hemiplegia is defined as a sequela of cerebrovascular accident (CVA) characterized by loss of voluntary movements in one half of the body together with postural tone disorder that may be increased (spasticity), decreased (flaccidity), or both at the same time (Taro and Gómez, 2019. p 73). Hemiplegia "should be approached as the beginning of a set of changes in the neurological condition, functional and social capacity of the individual, subject to modifications by multiple factors" (Lombillo at al., 2014).
The most relevant affectations of the person with hemiplegia are the stability, alignment and posture of the body, which is why difficulties appear in walking. Since these people must undergo a rehabilitation process, from the physical point of view, it is necessary to know the behavior of the biokinematic indicators that characterize walking.
On the human walk, a large number of research have been carried out. In the bibliographic search, many works appear aimed at improving the social life of patients with hemiplegia. Within physical activity, there are the works of Martínez and Hernández (2012), related to therapeutic physical exercises for the rehabilitation of adult patients with hemiplegia in Santa Rita de Zulia; Dominguez, et al. (2013), related to cerebral palsy and cerebrovascular accidents; Taro, Gómez and Hernández (2018), on the training of physical activity professionals at work with people suffering from hemiplegia; Dutill, et al. (2020), on exercises to improve strength and balance in patients with ischemic stroke, as well as Mushett, et al. (2021), on physical-therapeutic exercises to rehabilitate hemiplegic patients. More recently Herrera and Gómez (2018) studied from the biokinematic point of view a case with hemiplegia operated on a benign tumor in the right parietal. Other works have been reported: Novo et al. (2016) and Ramírez et al., (2019) related to biomechanical studies of gait, but in patients with spinocerebellar ataxia type 2.
As can be seen, the study of this type of gait, from Biomechanics, is still insufficient. This, together with the results of interviews with medical and physical rehabilitation personnel who work in health areas of the " Pedro Díaz Coello" polyclinic in Holguín and with researchers from the Faculty of Physical Culture and Sports of the University of Holguín, the review of normative documents on the multidisciplinary work complemented by observations to rehabilitation sessions of patients with Hemiplegia allows to show that there are deficiencies, such as:
Insufficient studies from the kinematic point of view of gait in patients with hemiplegia.
Limited quantification of kinematic indicators that allow identifying the level of gait disturbance in patients with hemiplegia.
The foregoing evidences a problematic situation given between the need to know the behavior of the kinematic indicators of gait in patients with hemiplegia and its comparison with the normal gait pattern in order to characterize them from the physical point of view, in order to individualize their process. rehabilitation. Thus, the purpose of the research lies in determining the biokinematic modifications that are manifested in the gait of patients with hemiplegia in the "Pedro Díaz Coello" health area of Holguín. Thus, their results can be taken into account to propose more objective and personalized rehabilitation programs, given that, as we know, not all patients with the same diagnosis walk with the same gait pattern.
MATERIALS AND METHODS
In coordination with the rehabilitators, it was worked with the five patients who participate in the rehabilitation services of the aforementioned health area. All of them present hemiplegia where the involvement of the right lower limb predominates, caused by an ischemic (1) and hemorrhagic (4) stroke. The time of evolution of the disease ranges between 9 and 14 months.
In the following table, a set of data is collected that shows some characteristics of the population, which offer information to complement the study carried out (Table 1).
Table 1. - Some characteristic data of the sample to be studied
| No. _ _ | Age | Sex | type of accident vascular brain | Characteristic | Time (months) |
| 1 | 65 | F | Hemorrhagic | Right lower limb predominance | 9 |
| 2 | 66 | M | ischemic | Right lower limb predominance | 9 |
| 3 | 72 | M | Hemorrhagic | Right lower limb predominance | 11 |
| 4 | 69 | F | Hemorrhagic | Right lower limb predominance | 14 |
| 5 | 67 | M | Hemorrhagic | Right lower limb predominance | 8 |
Videography was used as an analysis technique that allows obtaining a film record from a real movement and studying different parameters of the movement performed, previously defined. It made it possible to collect information for data processing with the help of Kinovea 0.8.27 software for movement analysis. Using this technique, functional alterations can be assessed in the different segments of the lower and upper extremities, the spine and different phases of walking.
The results obtained by this method also allow comparisons to be made and assessments to be made regarding the evolution of prescribed rehabilitation treatments, which make it possible to know whether they have been effective or not, from its own quantification.
Video recording process and data collection
To obtain the video record of the patients during the gait, the necessary means and resources were selected:
Two NIKON video cameras with their tripods, horizontal level, manipulators and couplers (1/3 Exmor X CMOS Image Sensor. Fast f/1.7-3.4 Lens with 12 x Zoom Ratio, HD 1080/50i and 720/50p; COOLPIX L720, Full HD video recording, 1820p LSD screen 7.5 cm, 9921000 points EXPEDDC2 image processing system, 13 mega pixel, 20x zoom)
Measurement scale (distance measured on the support surface within the same filming plane), necessary to contrast in the motion analysis software.
A Pentium IV microprocessor computer for data analysis and Kinovea motion analysis software version 0.8.27 installed.
Informed consent of the patients who agree to be part of the research.
The following protocol was followed in the filming process:
Three recordings corresponding to the same movement were made, one in the sagittal plane and the other in the frontal plane, separated by a brief period of rest.
The cameras were placed fixed on the tripod without oscillations or magnification. Its arrangement is illustrated in Figure 1 (Figure 1).
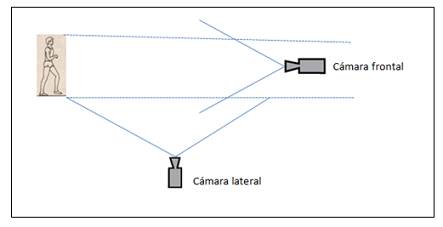
Fig. 1. - Simplified diagram showing the arrangement of the cameras with respect to the subject under study for filming
In the sagittal plane, it was filmed from a distance of 3.7 meters and a height of 1.12 meters, so that a complete cycle of the patient's gait could be visualized at a reasonable distance.
In the frontal plane, the camera was placed at a distance of 3.7 meters and a height of 1.01 meters, which would allow complete observation of the patient from a better position.
The distance traveled by the patient was 4 m, useful for analyzing various gait cycles.
RESULTS AND DISCUSSION
For data collection, patients were asked to walk back and forth, a reasonable distance (approximately 4 m.) indicated by the researcher, just as they do in daily life, with the aim of being able to use the most useful part of filming. This process was performed three times, as indicated above.
Once the useful video for the study was selected, using the Kinovea 0.8.27 human movement analysis software, the following previously selected indicators were measured:
Stride length: Distance between two equal and successive events of the same limb. Range for normal walking: 1.55 1.58 m.
Step length: Distance that separates the initial support of one foot from the initial support of the other. Range for normal walking: 0.77 0.78 m.
Step width: Linear distance between two equal points of both feet (eg distance measured between both heels). For normal walking up to 10 cm.
Step angle: It refers to the orientation of the foot during the support with respect to the line of progression (translation direction). approximately 15º
Articular angle of the knee for each phase. Angle formed between the projection of the leg and the thigh segment. In the support phase approximately 15º 20º (foot flat on the ground)
Time: Moments and duration of the movement. (Duration of stance phases, swing phases, and stride phases)
Cadence or frequency: Number of steps per unit of time that is generally set at one minute: For normal walking 90 140 steps per minute.
Gait speed: Ratio of the distance traveled in the direction of the march per unit of time. For normal walking. 1.25 1.33 m/s [meters/seconds] (Figure 2).
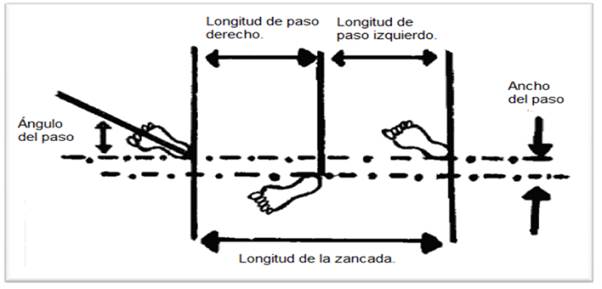
Fig. 2. - Illustrative example of a stride and some of the kinematic indicators of normal human walking
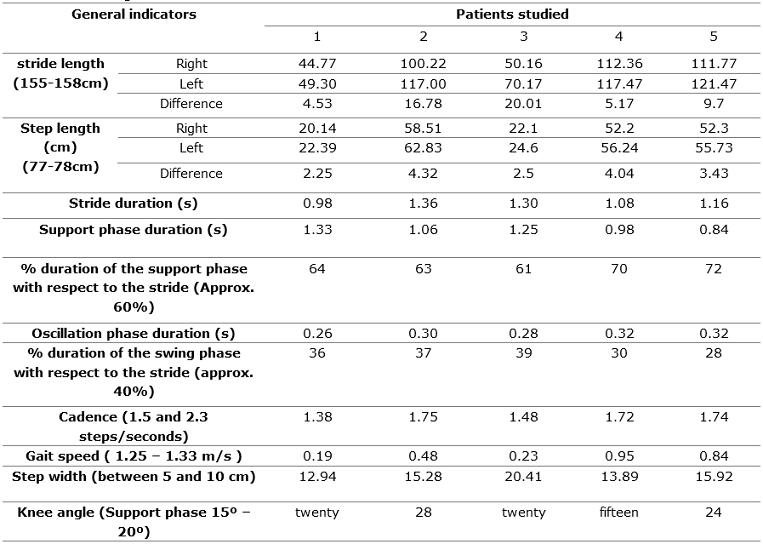
On the other hand, it is necessary to limit that, according to the currently most widespread criterion regarding the time spent during each phase of the gait cycle, at a normal speed, it is approximately 60 % of the cycle in the support phase and 40 % % of the cycle in the oscillation or swing phase (Table 2).
Table 2. - Values of the general biokinematic indicators determined in movement and their references for normal walking
To illustrate part of the measurements made, the following figure is included (Figure 3).
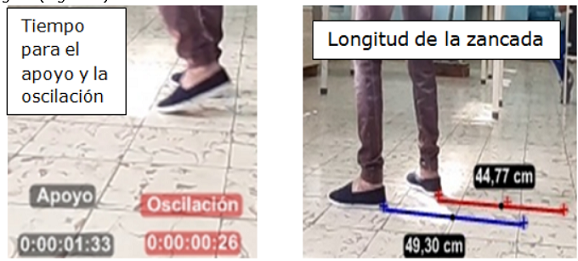
Fig. 3 Representative example of some of the measurements made using the filmic record of the patients and the Kinovea 0.8.27 movement analysis software
From the analysis of the previous results, it was possible to infer that:
Gait speed indicates the ability of patients to walk. Although it is known that this declines with age, which is more noticeable in the seventh decade of life, all patients have gait speed well below established values. This requires more energy to keep moving, since when the speed decreases, the kinetic energy is lost, and it is as if the patient started the movement from scratch.
Regarding the percentage of duration of both the support phase and the oscillation phase, although all the patients show affectations, the most critical turn out to be 4 and 5, since their values differ greatly from those established as normal. It is considered to be a logical behavior, having to guarantee stability to take the next step.
Regarding the width of the step, all patients are above the values reported in theory (5-10 cm) as normal, an indicator closely related to stability and balance. Patient 1 had the best result. The foregoing talks about the need to adopt positions that guarantee a greater support area and therefore greater stability in order to achieve balance.
The cadence is used to assess the rhythm and speed of the gait that each person self-selects to walk. During normal walking, values that oscillate around 2 steps/s are recorded. The patients that are closest to what is referenced are 2, 4 and 5, being above 1.72 steps/s. While patients 1 and 3 are below 1.5 steps/s. Patient 2 has the highest value and patient 1 the lowest.
Regarding the joint angle of the knee, it was analyzed in the support phase. Patients 1, 3 and 4 present values within the normal range, but not so in patients 2 and 5, in which the angle is higher, demonstrating difficulties in flexion-extension of the leg.
Methodological recommendations derived from the analysis of the behavior of biokinematic indicators in gait in patients with hemiplegia.
The previous results show the main factors that, from the physical point of view, determine the affectations of gait in hemiplegic patients. They were discussed with the medical and physical culture personnel who work in the rehabilitation room.
In order to improve the process of gait involvement in the patients studied, the following methodological recommendations are proposed to be taken into account for their inclusion in the physical rehabilitation process:
Increase actions aimed at the mobility of the lower limbs because limitations are observed in the performance of oscillatory movements in the lower limbs, typical of normal walking, accentuated in patients 1 and 2.
Perform exercises that lead to improving balance given that the width of the step was in all cases greater than the recommended values, standing out to a greater extent in patient 3
Systematically control the behavior of the indicators by phases, so that adjustments can be made to the physical rehabilitation process for each patient.
Implement strengthening exercises of the muscular planes of the affected limbs, given that:
Although in all cases the gait is not symmetrical, that is, they tend to deviate the body towards the right side due to the fact that the step towards this side is shorter, this is accentuated in patients 2, 4 and 5.
They require more support time than normal (above the 60% recommended approximately), evidenced in patients 4 and 5, which causes the speed of walking to decrease and requires more energy during movement.
The knee flexion angle is greater than that recommended in patients 2 and 4, which implies a longer time in the support phase and a greater energy expenditure to continue walking. Patient 1 is at the lower limit. This constitutes an alert since, when this occurs, it is due to poor strength in the lower limbs or muscle contractures that make it possible to maintain the march in a coordinated manner. Remember that the weakness of the quadriceps generates an excessive flexion of the knee joint, while the spasticity of the quadriceps generates a hypertonic response with the consequent premature extension of the knee.
As no references were found for biomechanical studies, in this case kinematic, aimed at carrying out a quantitative evaluation of gait indicators in hemiplegic patients, as stated in the introduction, the comparison made was with normal walk, taking as reference the set of values proposed by Ramírez, Gómez, Vázquez and Ramírez (2019), for each indicator studied and which are listed in Table 2.
CONCLUSIONS
Summarizing the above on the basis of the results obtained in the research, it was possible to analyze the behavior of the biokinematic indicators of hemiplegic gait in the patients studied, their comparison with normal gait, as well as a set of recommendations to be taken into account in the rehabilitation process, with what will be achieved, from the physical point of view Therapeutic, a functional re-education of your physical state, for example, corrections in posture, greater self-control of movements, better coordination in a general sense (static and dynamic balance), together with the modification of psychological factors that affect your personality.
REFERENCIAS BIBLIOGRÁFICAS
Domínguez, J; Lemos, R., y Vizaguirre, R. (2013). Conocimiento de la población sobre Accidentes Cerebro Vasculares. Biblioteca Digital UNCUYO. Mendoza. Universidad nacional de cuyo. Facultad de ciencias médicas. Escuela de enfermería. https://bdigital.uncu.edu.ar/5915 [ Links ]
Dutill, Y., Echemendía, A., y Núñez, I. (2020). Ejercicios para mejorar la fuerza y equilibrio en pacientes con ictus isquémico. Acción, 16. http://accion.uccfd.cu/index.php/accion/article/view/115 [ Links ]
Fitz-Allan, D., y Lozada, M. (2022). Estudio de la hemiplejia en San Vicente y las Granadinas. Olimpia, 19 (1), 56-67. https://revistas.udg.co.cu/index.php/olimpia/citationstylelanguage/get/ieee?submissionId=2908 [ Links ]
Herrera, M., y Gómez, M. (2018). Análisis biomecánico de la marcha patológica: un estudio de caso. Deporvida, 15(35). https://deporvida.uho.edu.cu/index.php/deporvida/article/view/431 [ Links ]
Lombillo, L., Martínez, S., Serra, Y., y Rodríguez, L. (2014). Complicaciones en pacientes hemipléjicos por ictus. Revista Cubana de Medicina 53(2). http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S0034-75232014000200004 [ Links ]
Martínez, J., y Hernández, A. (2012) Alternativa de ejercicios físicos en la rehabilitación a pacientes adultos con hemiplejía por infarto cerebral en el municipio Santa Rita. Estado Zulia. Deporvida , 9(17). https://deporvida.uho.edu.cu/index.php/deporvida/article/view/183 [ Links ]
Mushett, I., Gómez, E., y Romero, C. (2021). Ejercicios físico terapéuticos para rehabilitar pacientes hemipléjicos. Famadeportes, 11(20) [ Links ]
Novo, C., Gámez, O., Montoya, P., Zulueta, A., y Zamora, L. (2016). Descripción cinemática de la marcha en pacientes con ataxia espinocerebelosa tipo 2. Versión On-line ISSN 1029-3019. MEDISAN 20(12), Santiago de Cuba. http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S1029-30192016001200003 [ Links ]
Ramírez, S; Gómez, A: Vázquez, Y., y Ramírez, D. (2019). Indicadores biomecánicos para el estudio de la marcha en pacientes con ataxia espinocerebelosa tipo 2, en estadio I. Olimpia , 16(57). https://redib.org/Record/oai_articulo2407180-indicadores-biomec%C3%A1nicos-para-el-estudio-de-la-marcha-en-pacientes-con-ataxia-espinocerebelosa-tipo-2-en-estadio-i-original [ Links ]
Taro, J., y Gómez, A. (2019). Rehabilitación de la Hemiplejia Crónica. Un modelo de superación desde la actividad física adaptada. Deporvida , 16(39), 72-88. https://deporvida.uho.edu.cu/index.php/deporvida/article/view/693 [ Links ]
Taro, J., Gómez, A., y Hernández, M. (2018). Formación de profesionales de la actividad física en el trabajo con personas aquejadas de hemiplejia. Efdeportes, 23 (245). https://efdeportes.com/efdeportes/index.php/EFDeportes/article/view/341 [ Links ]
Received: April 07, 2022; Accepted: July 20, 2022

