










 Custom services
Custom services
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
Permalink
Introduction
In Brazil, mobile Pre-Hospital Care (APH) is divided into primary and secondary. The first aims to address the victim early after an injury classified as an urgent or emergency (clinical, surgical, traumatic, psychiatric) that could lead to suffering, sequelae, or death. To be responsible for the care and/or transportation to a hierarchical health service integrated into the Unified Health System (SUS). Secondary mobile APH, known as inter-hospital removal, is when the request comes from a public health institution where the patient has already received first care but needs to be transported to a more complex service for treatment follow-up.1,2
The Mobile Emergency Care Service (SAMU) is present in 3,049 municipalities in Brazil, most of which are concentrated in the Northeast and South regions, with an estimated coverage of 76.28% of the population in 2015, therefore, more than 155 million inhabitants. In the country, this service is controlled by 210 regulation centers, which structure the care provided by multidisciplinary teams with the support of around 3,108 ambulances, establishing indispensable communication between the health system and the public.3
Local and municipal administrations need to act in the promotion and maintenance of the equipment used by health professionals, make investments in the service and its collaborators, as well as in the information and knowledge of its users about the role of the emergency service in public health with the objective of that there is safety and quality in care procedures.4
Thus, the management of axes related to the regulation of occurrences is capable of helping to organize actions and human resources.5) In addition to contributing to a better structuring and territorial distribution of the service. Such data can provide managers with essential information for building strategies and structural adaptation of health services, especially hospital emergency rooms and the SAMU itself, as well as prevention, promotion, recovery, and health qualification, aiming at a better articulation of the entire Health Care Network in the municipality.6) In addition, it provides contributions to the planning of the municipal government, concerning the demands of traffic and public roads.
A nationwide data analysis found that the mortality rate from traffic accidents in the year in question was 21.0 deaths per 100,000 inhabitants, with the Midwest region presenting the highest rate (29.9 deaths per 100,000 inhabitants). per 100 thousand inhabitants). Still, among these deaths due to land transport incidents, the majority occurred in males (34.9 deaths per 100,000 men) and more than half corresponded to blacks, young adults (24.2%), individuals with low education (24.0%), and motorcyclists (28.5%). So, throughout Brazil, in 2013, more than one million years of potential life were lost due to car accidents.7
In the case of mobile service in the State of Rio Grande do Norte, in 2014, SAMU-192 had 24 bases allocated in 52 cities that serve approximately two million inhabitants, reaching 75% of the Potiguar population, according to statistics from the year, operating with specialized teams in synchrony with services included in the SUS.8
In the municipality of Mossoró/Rio Grande do Norte, SAMU-192 was implemented in 2005. The team is composed of doctors, nurses, nursing technicians, and drivers who are divided into three basic support units (USB) and two support units. advanced (USA). According to SAMU reports from 2017 to 2019, about 90 thousand services were provided in Mossoró and the region, on average, there are about 70 to 100 services per day and approximately 400 thousand since its creation.9,10,11
In view of the above, there is a need to collaborate with the monitoring of urgencies and emergencies and, thus, facilitate intersectoral integration in the municipality, providing increasingly optimized services, based on the predominant demand of each region. Therefore, this study aims to outline the epidemiological and geospatial profile of incidents attended by the Mobile Emergency Care Service.
Methodology
This is an epidemiological, cross-sectional, retrospective descriptive study, of a quantitative nature, developed at SAMU in the city of Mossoró/Rio Grande do Norte. The universe researched was composed of medical regulation forms and pre-hospital care bulletins, referring to the occurrences attended in the year 2019, in which vehicles were sent. The choice of the year 2019 was due to the pandemic, considering that the great contamination by COVID -19 changed the clinical profile of the occurrences, directing them to this type of service, in addition to having modified population habits, allowing the creation of a study design without analysis bias.
Medical regulation forms consist of information to be filled in on data collected at the Medical Regulation Center related to the call, such as number, date and time, regulating physician, Medical Regulatory Assistant Technician (TARM), reason, requester, and telephone; to the patient, full name and address; the help, type (psychiatric, traumatic, clinical case, obstetric) and requester's complaint; the assessment of the patient by the regulating physician, state of consciousness, airways and oxygenation, pulse, trauma and presumed severity; description, if hospitalization and transport are required (type of ambulance, place of origin and destination); to the radio, time and staff; local evaluation of the patient; mission execution, final destination and incidents; and finally, description of the reason, whether clinical or traumatic and presumable diagnosis.
APH bulletins are used only when a vehicle is dispatched and consist of primary data collected at the Medical Regulation Center, such as name, address, age and sex of the victim, date and time, ambulance sent, if it is a removal inter-hospital, names of professionals (physician and/or nurse and/or nursing technician and vehicle driver) if it refers to an accident at work, reference point and nature of the occurrence. In the information on the approach to the victim, to be completed by the team that will provide care on-site; the care bulletin guides professionals on the steps to be followed in the primary assessment with the ABCDE of trauma, patient responsiveness, chest expansion, central pulse, and hemorrhages; in the secondary assessment, from the collection of the SAMPLE history and vital signs; scene description in trauma kinematics; medical notes; drug prescription; nursing notes/evolution; patient's fate; proof of delivery of values; term of refusal of service.
As an inclusion criterion for the research, regulatory records/occurrence reports attended by ambulances in the municipality of Mossoró/Rio Grande do Norte during the year 2019 were selected. And in relation to the exclusion criteria, those that perhaps have been attended to by the local SAMU, but outside the municipality limits; those with incomplete filling, erasures or illegibility; those referring to cases of patient evasion from the location, removal carried out by third parties, those that did not receive interventions other than guidance on site or those where the victim was not found; cases that resulted in death; and cases in which there was no vehicle sent, just medical advice via regulation.
To construct the sample for this study, manual accounting of the completed and stored medical regulation forms was carried out, separated by each day of the year. After this process, a random number was drawn that corresponded to one of the forms, and the process was repeated if the selected form did not meet the research eligibility criteria. Using this selection methodology, a total of 363 medical records were sampled. The collected data were tabulated and analyzed using the Statistical Package for Social Science (SPSS) software, version 20.
For the analysis of the epidemiological profile of attendance, the absolute and relative frequencies were calculated from the gender and age group variables. For the variables' nature of occurrence, days of the week, ambulance sent, inter-hospital removal, and patient destination, absolute and relative frequencies were calculated. Based on the type of occurrence variables, namely, clinical case, traumatic, psychiatric and obstetric, the neighborhoods of the occurrences were identified to carry out the spatial distribution.
Geospatial treatment data was inserted in a spreadsheet and subsequentely attached to the base map of Mossoró neighborhoods, producing a Geographical Information System - GIS with data geoespacialized by zones, or polygons. For this process we used the software QGIS 3.10 version 'A Coruña to produce geospatial analysis and maps, identifying geographic clusters.
The main limitation of the study involved the use of secondary databases, more specifically, the high amount of ignored data identified in the service's database, which portrays the team's deficiency in recording information, since these are related to the correct completion of records of first responders, physicians, and nurses.
This project follows the determinations of Resolution nº 466/2012 of the National Health Council for Research with Human Beings, approved by the Ethics Committee in Research with Human Beings of the State University of Rio Grande do Norte (UERN), under the opinion of No. 5,130,066. The present study dispenses with the need for an Informed Consent Form due to its methodological design, which includes the use of information available from a secondary data source belonging to the institution. Data were analyzed anonymously, not allowing the identification of research participants.
Results
The sample consisted of 363 occurrences, 221 (60.9%) of a clinical nature, 115 (31.7%) of a traumatic nature, 24 (6.6%) of a psychiatric nature, and three (0.8%) of a psychiatric nature. gynecological/obstetric. Of which, regardless of the nature of the care, 115 (31.7%) were inter-hospital removals, and 248 (68.3%) comprised approaches to patients on public roads/at home. During the construction of the study design, the average of daily occurrences was 40.8, with August having the highest average (44.4) and October having the lowest (34.5).
There was a predominance of occurrences due to clinical causes on all days of the week. Regarding the traumatic nature, there was a predominance on Mondays and Wednesdays, and weekends, and on Sundays there was an increase in the absolute number of visits of a traumatic nature, configuring the day on which it occurred the most (fig. 1). It is important to emphasize that interhospital transfers accounted for more than 20% of all daily consultations, especially on Mondays and Thursdays, with 38.8% and 47.0%, respectively, surpassing the cases of attendance by traumatic nature at some points.
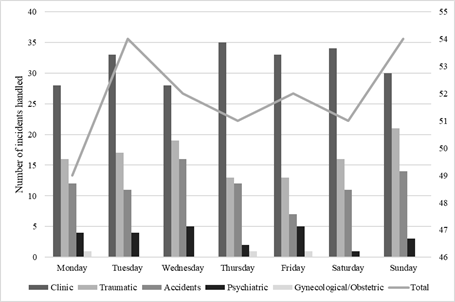
Source: Prepared by the authors, 2022.
Fig. 1 - Occurrences attended by SAMU-192-Mossoró according to a day of the week and nature of occurrences from January to December 2019. Mossoró, Rio Grande do Norte, Brazil, 2022.
The times with the highest peak of occurrences are located in the intervals: 16:00 to 20:00, 7:00 to 8:00, and 10:00 to 12:00. As such, it can be suggested that the predominance of morning shifts, plus the majority of clinical causes, are periods when activities start and caregivers arrive. Specifically, traumatic causes have a higher incidence at 7 am and 6 pm, and at 9 am, 2 pm and 8 pm there is a greater decline in traumatic events in general.
The mean age of all incidents was 51 years old and the median was 51.7 years old. The minimum age was zero years (11 days of life) and the maximum was 102 years. Table 1 shows that the age group corresponding to young adults concentrated the highest proportion of total occurrences (52.3%), traumatic causes (79.1%), and psychiatric causes (79.2%); the elderly had the highest incidence of consultations due to clinical causes (57%); of the total number of services, 8% were aimed at children and adolescents.
Table 1 - Nature of occurrences assisted by SAMU-192-Mossoró according to age group and gender from January to December 2019. Mossoró, Rio Grande do Norte, Brazil, 2022
| Variables |
|
|
|
|
|
|---|---|---|---|---|---|
| N (%) | N (%) | N (%) | N (%) | N (%) | |
| Age Range | |||||
| Children and teenagers | 17 (7.7) | 09 (7.8) | 02 (8.3) | 01 (33.3) | 29 (100) |
| Young adults | 78 (35.3) | 91 (79.1) | 19 (79.2) | 02 (66.7) | 190 (100) |
| Elderly | 126 (57.0) | 15 (13.0) | 03 (12.5) | - | 144 (100) |
| Sex | |||||
| Female | 111 (50.2) | 36(31.3) | 11 (45.8) | 03 (100) | 161 (100) |
| Male | 110 (49.8) | 79 (68.7) | 13 (54.2) | - | 202 (100) |
Source: Prepared by the authors, 2022.
The sizing by nature of cause shows that there was a greater expression of consultations due to clinical causes in females (50.2%), despite a very similar percentage in males (49.8%). However, it points out that men had a higher risk of incidents due to traumatic causes (68.7%).
Table 2 indicates that 58.7% of occurrences due to clinical causes fit into three main groups: diseases of the cardiovascular system, with 13.6% (with cases of acute myocardial infarction accounting for 60% of care in this group); neurological disorders (9.1%) - containing cases of seizures (5.9%) and stroke (3.2%), the latter being morbidity with a great capacity to leave sequelae and easily identified in more common cases; and diseases of the respiratory system (8.1%), including asthma attacks (1.8%), chronic obstructive pulmonary disease (2.7%), acute pulmonary edema (1.8%) and pneumonia (1.8 %). Also noteworthy is the fact that 60.6% of consultations due to clinical causes had their motivation not identified.
In terms of traumatic causes, transport accidents accounted for 72.2% of occurrences, followed by 14.8% of falls from standing heights. As for occurrences of a psychiatric nature, psychotic episodes represent 87.5% of the cases. Gynecological and obstetric reasons are not well known (Table 2).
Table 2 - Reasons for occurrences attended by SAMU-192-Mossoró according to the nature of the occurrence from January to December 2019. Mossoró, Rio Grande do Norte, Brazil, 2022
| Nature of occurrence | Reason for occurrences | N | % |
|---|---|---|---|
| Clinic (n = 221) | Brain stroke | 07 | 3.2 |
| Cardiovascular | 30 | 13.6 | |
| Hypertensive crisis | 07 | 23.3 | |
| Acute myocardial infarction | 18 | 60.0 | |
| Cardiopulmonary arrest | 03 | 10.0 | |
| Atrial fibrillation | 02 | 6.7 | |
| Convulsive crisis | 13 | 5.9 | |
| Asthma attack | 04 | 1.8 | |
| Chronic obstructive pulmonary disease | 06 | 2.7 | |
| Acute lung edema | 04 | 1.8 | |
| Pneumonia | 04 | 1.8 | |
| Hypoglycemia | 03 | 1.4 | |
| Other clinical causes* | 16 | 7.2 | |
| Not identified | 134 | 60.6 | |
| Traumatic (N = 115) | Transport accidents | 83 | 72.2 |
| Aggressions | 07 | 6.1 | |
| Fall from own height | 17 | 14.8 | |
| Fall from height | 01 | 0.8 | |
| Cerebral hemorrhage | 01 | 0.8 | |
| Not identified | 06 | 5.2 | |
| Psychiatric (n = 24) | Psychotic break | 21 | 87.5 |
| Suicide attempt | 02 | 8.3 | |
| Schizophrenia | 01 | 4.2 | |
| Gynecological/Obstetrics (n = 3) | Transport accident | 01 | 33.3 |
| Vaginal bleeding | 01 | 33.3 | |
| Labor | 01 | 33.3 |
Legend: *They are choking/obstruction by a foreign body, erysipelas, cystic fibrosis, upper digestive hemorrhage, lower digestive hemorrhage, hyperglycemia, acute renal failure, intestinal obstruction, cancer, sepsis, liver cirrhosis, and anaphylaxis.
Source: Prepared by the author, according to data from SAMU-192, Mossoró/Rio Grande do Norte, 2019.
In terms of land transport accidents, it is possible to identify that cars were involved in 42 of the 83 traffic accidents overall, while motorcycles were involved in 76, in the same sample space. Also, it appears that, among the collisions, those involving car and motorcycle add up to 43.4% of the weighted accidents, while a motorcycle colliding with a motorcycle represents 18.1% of the total, followed by the collision between motorcycle and animal with 3.6 % of the total. In the analysis of falls, there is a discrepancy between the frequency of motorcycle falls (24.1% of all accidents) and car falls (2.4% of all accidents).
The geospatial distribution of occurrences by nature on a public road/domicile is shown in figure 2. It is observed that, because of the 248 total pre-hospital care, 14.1% were carried out in the Santo Antônio neighborhood, followed by the neighborhoods: Alto de São Manoel, Abolição and Aeroporto. Within the scope of clinical causes, 14 districts had an incidence greater than or equal to 50%, with emphasis on Bela Vista, Pintos, and Barrocas. In terms of traumatic causes, the neighborhoods of Alto da Conceição, Doze Anos, and Centro stand out, this sector is characterized by many vehicles circulation, because are central neighborhoods where most traumas were caused by traffic accidents. As for psychiatric care, the neighborhoods of Lagoa do Mato, Redenção and Nova Betânia stand out. The only pre-hospital gynecological/obstetric care, which was labor and delivery, took place in the Santo Antônio neighborhood.
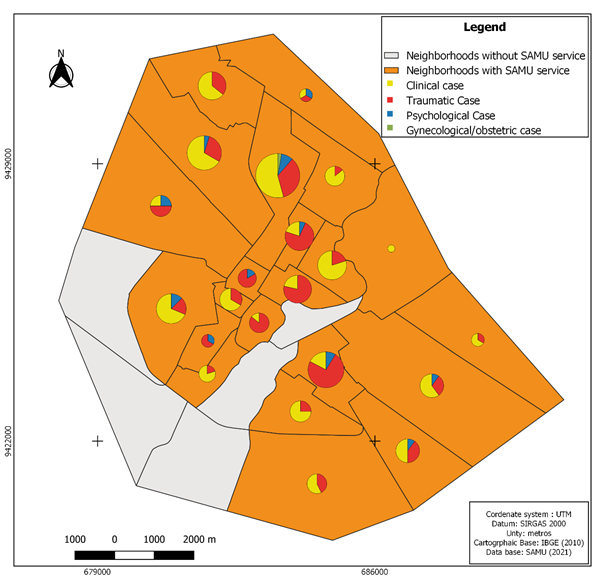
Source: Prepared by the author.
Fig. 2 - Spatial distribution of pre-hospital care on public roads/at home by SAMU-192-Mossoró according to the nature of the occurrence from January to December 2019. Mossoró, Rio Grande do Norte, Brazil, 2022.
The composition of the figure above is highlighted only by the occurrences in public roads/homes, because they are primary care, therefore, unpredictable, dependent on the information provided by the requester and the sending of the correct human resources and materials in the midst of the unknown. Since, in the removals, they are patients already in a hospital environment, that is, controlled, with medical assistance and predicted diagnostic hypothesis.
The spatial distribution according to the number of visits due to traffic accidents in each district of the municipality of Mossoró is represented in figure 3, demonstrating that the Alto de São Manoel district has the highest incidence of this type of trauma, followed by the Santo Antônio and Center. The vehicle circulation, also, seems to be decisive, mainly for the Alto de São Manuel with 16 occurrences. It is observed that the south zone of Mossoró, was responsible for the majority of treatments for traumatic causes, having requested 46 (40.0%) of the 115 analyzed occurrences, ahead of the north zone 20 (17.4%), east zone 18 (15.7%), west zone 15 (13.0%), central zone 13 (11.3%) and, finally, rural zone two (1.7%).
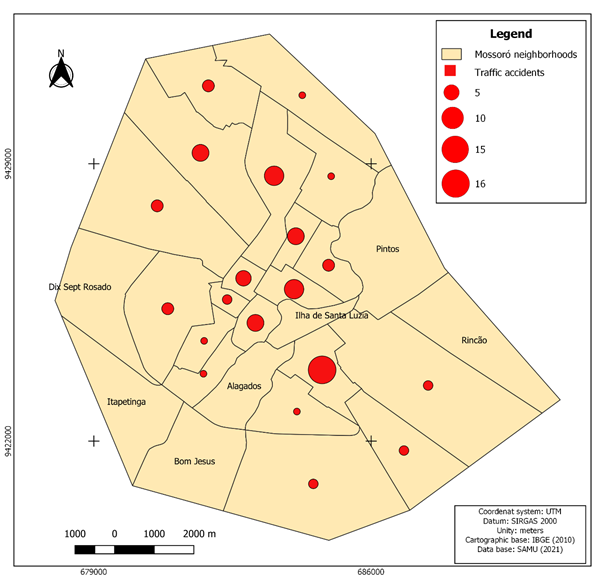
Source: Prepared by the author.
Fig. 3 - Spatial distribution of land transport accidents attended by SAMU-192-Mossoró according to neighborhoods from January to December 2019. Mossoró, Rio Grande do Norte, Brazil, 2022.
As mentioned above, SAMU-Mossoró is made up of a fleet of five different ambulances, two USAs, and three USBs, which are located at the SAMU-192 base in the municipality. In this scenario, there is a higher frequency of dispatch of USB (87.3%), both for care on public streets/homes and for inter-hospital removals. However, a striking fact is that, when used, the AUS is mostly intended for transfers between hospital units (76.1%), representing 31.7% of the total occurrences.
As for the hospital unit of final destination for assistance, most patients were transported to the Hospital Regional Tarcísio Vasconcelos Maia (59.8%), a reference institution for trauma in the western region of Rio Grande do Norte, which, however, admits both victims for traumatic causes (50.5%) and clinical causes (48.6%). Following him, we have the UPA in the Santo Antônio neighborhood as the second unit to receive a more expressive number of patients (17.9%), and of these, emphasis should be placed on receiving 15 (23.4%) of the 24 occurrences of the psychiatric type. The portion of the ignored destinations was due to the composition of four on-site visits, which were carried out in long-stay institutions and the prison, and one heading to the capital, Natal.
Discussion
The characterization of the clinical-epidemiological profile of mobile pre-hospital urgent and emergency care services, presented here, was able to provide useful information to the managing bodies of the local health sector and the municipality.
Similar to our findings, most incidents of traumatic causes occurred among individuals aged 19 to 59 years.12) As well, males had a higher number of occurrences, as they presented more risk factors when compared to females, such as alcohol abuse, dangerous driving in cars, carelessness with chronic diseases, and menial services with greater risks of physical harm.13) Young men deserve evidence regarding the performance of actions to promote and prevent urban traffic accidents since they are the most affected by this condition.14) According to the World Health Organization (WHO), these groups are about three times more likely to die in a transport accident than young women.15
According to a similar data survey, carried out at SAMU-192-Olinda, in 2006, among the occurrences due to external causes, transport accidents were responsible for 52.7% of these; pedestrians being responsible for 61.1% of transport accidents, while collisions for 26.1%, followed by 8.9% of falls in traffic and 3.9% of rollovers, in contrast to data obtained from SAMU-192-Mossoró, where collisions were predominant, followed by falls and being run over, respectively. Despite this, another study found collisions (14.3%) as the most frequent traumatic cause.16) Still, according to the study carried out at SAMU-192-Olinda, the similarity of the data referring to the days of the week in which the highest number of occurrences of a traumatic nature occur, except for Wednesday, which at SAMU-192-Mossoró was right after Sunday.17
According to an analysis by the Federal Council of Medicine, an average of 20 peoples are admitted to a public health hospital per hour with a serious injury resulting from a land transport accident. If the total number of serious traffic victims in the last ten years is analyzed, it appears that 60% involved victims between 15 and 39 years old, with a lower frequency in the age groups from zero to 14 years old (8.2%) and in those over 60 years old (8.4%); and, still, almost 80% of the victims were male.18) Accordingly, this data collection at SAMU-192-Mossoró found that the municipality follows the standards of this national average, considering that occurrences of a traumatic nature, which are mostly transport accidents, occurred in adults and young males.
The results cited in this study reaffirm that the observation of service peaks can help in the planning of health activities and the allocation of resources.17) It is considered that this information is explained by the time when people are coming and going from work, the increase in the flow of vehicles, and displacements.19) In addition, it can be weighted according to events, interdictions, or any other events that modify the flow of people and vehicles in the municipality.
Another study showed a higher frequency of occurrences due to clinical causes in both genders, and of these, a greater proportion was due to cardiovascular diseases, corroborating the data found in the current research.6) According to WHO information, the leading cause of death in Brazil is due to diseases of the circulatory system (29.4%), approximately 308,000 individuals die each year, mainly from infarction and stroke.20) In addition, these numbers are expected to increase due to increased life expectancy and an aging population, as well as the continuation of inadequate eating habits and physical activity.21
Still referring to intercurrences of clinical cause, a survey carried out in the city of Chapecó informs a percentage of this nature of occurrence of 41.0% versus 35.4% of traumas.22) It also reports the ineffectiveness of public policies for prevention and health promotion. Concerning neurological disorders, a study epidemiologically delineated the victims rescued by a SAMU and pointed out that 59% of the visits were due to stroke and 11% due to seizures, the latter close to the finding at SAMU Mossoró, which was 14.9%.23
Faced with the difficulties in offering, structuring, and organizing care on the part of the basic service network, the availability of SAMU-192 encourages other means of acting in the face of illness. Inefficient connections between users and the team and/or health professional, low perspectives regarding the competence of the service to meet immediate needs, even if the home is close to a certain urgent and emergency service or even in areas benefited by the Family Health Strategy (ESF), present themselves as obstacles,22 which seem to be in accordance not only with the behavior of care for the elderly but also when identifying cardiovascular diseases.
As for the care network, the municipality of Mossoró has 71 Family Health Strategy teams with a coverage of 69.49% of the population. It has 46 Basic Health Units (UBS), 32 in urban areas and 13 in rural areas; three Emergency Care Units (UPAs), located in the Alto de São Manoel, Santo Antônio, and Belo Horizonte neighborhoods. With Mossoró as the hub city of the western region of the State of Rio Grande do Norte, it is common for citizens, locals, and neighbors, to report to UBS-centered services such as the Tarcísio de Vasconcelos Maia Regional Hospital (reference for multiple trauma patients) and the Almeida Maternity Hospital Castro (mother-infant reference).
As for the units used in the consultations, it is in line with other studies, in which the USB was used 57.3% of the time, followed by the USA with 42.7%, and with a survey carried out in the North of Minas Gerais Macroregion, in which the USB were shipped at 89%.16,24) However, the present study outlines the possible problem that in the circumstance of increased user demands, considering the workloads of the vehicles, the request to remove patients can compromise the availability of ambulances, making the system more congested.25
Individually, in the health area, the most important logistical problems pervade the positioning and performance of ambulances that provide emergency care, management and allocation of teams and resources, and integration with the care network. The location and operation of this equipment are sensitive to the level of complexity required, mainly characterized by the response time to the service or request. Poor quality coverage or communication between services may result in vital damage or the appearance of sequelae.26
That said, Ordinance No. 2657 of the Ministry of Health, of December 16, 2004, presents the concept of a Decentralized Base, which authorizes the existence of decentralized operational bases that act as outposts for ambulances and their teams, trying, in this way, to guarantee a time of quality response to SAMU users.27
In inter-hospital transfers, responsible for 115 (31.7%) of the occurrences in Mossoró, the level of assistance must be established before the transfer, through communication and opinion between the SAMU and the hospital of origin physicians, who must decide what level of life support the patient requires, whether basic or advanced, given the severity of the condition, what are the possible changes or deterioration of clinical conditions, also assess age and comorbidities, or even if the removal needs to be immediate or not.28) In addition, all the equipment that makes up the vehicles that will carry out the transport must be in perfect condition for use. During the years 2005 to 2011, it showed an average of 8,841 occurrences/year in the SAMU of this nature, a number that is much higher than the data found, even when considering that the capital of Piauí has a population almost three times greater than that of the municipality in question.29
As for the units of destination, the results analyzed were consistent with research in which a large number of victims were taken to a referral hospital for trauma in the city.30,31) In the municipal scenario, this is the Tarcísio de Vasconcelos Maia Regional Hospital (HRTVM), which, despite being a reference for polytrauma patients, also receives most clinical conditions, even after the implementation of the UPA, since 2002, the urgency and emergency network. It should be noted here that psychiatric cases, although not very expressive, are referred to the UPA Conchecita Ciarlini in the Santo Antônio neighborhood.
In short, managers and decision-makers of rescue systems need to be aware of the condition and level of service offered to users so that they can properly assess the configurations, protocols, and performance measures of their teams and collaborators. This is to have the sufficient foundation to balance the state of assistance with the required investments that are capable of offering an adequate, quality, and effective emergency service.25
Thus, from the above, the importance of monitoring and managing the occurrences attended by SAMU-192 is evident, since the data found to provide a solution to the identified obstacles, to demonstrate the need to organize and systematize health care properly so that achieve and obey the principles of the SUS.
Conclusion
It is important to know the geographic distribution and location of the servers, whether ambulances or health units and the incidence of a certain type of occurrence, to assist in the dispatch policy of emergency vehicles, as well as, direct services. In this way, the data provide subsidies for decision-making at the public power level. As well as for the establishment of new health planning and surveillance strategies. Therefore, the emergency service, territorialized and mobile, means that ambulances need to be strategically distributed, to improve and optimize the response time between calls and directing to reference services.
The information ratifies the need for joint intersectoral work, involving different municipal administration bodies. The use of spatial analysis shows how fundamental the integration between health management and related bodies is, for the implantation and implementation of preventive and corrective measures, with emphasis on the problem of transport accidents and the improvement of protocols and pre-established forms. As well as contributing to the construction, with the help of the public authorities and before the population, of a care scenario consistent with reality.

